8

Headache and Rhinosinusitis
Otolaryngologists frequently see patients with the symptom of headache, and the patient often believes the headache is sinus related. Yet, for the majority of patients who believe they have sinus headaches, it is not. Therefore, it behooves the otolaryngologist to have a thorough understanding of headache and how the symptomatology may or may not relate to the sinuses. Patients want the headache to be sinus related because it is far more socially acceptable if a patient is suffering from a “sinus headache” than from the most frequently seen headache, a “tension headache.” The media have made sinus headaches appear quite common when in fact other types of headache are more common. Various over-the-counter cold and sinus medications relieve the headache, not because of the nasal and/or sinus medication they contain, but rather because of the analgesics or sedative effect of the antihistamines that are part of the medication.
Pain from nasal and/or sinus disease can be present in many areas of the face and be referred to a distant area of the head or neck. Physicians are taught that percussion of sinuses will reveal the site of sinusitis if pain is elicited, yet this is quite inexact and often provides misleading information. Because tension headaches can cause tenderness of the facial muscles and scalp, percussion of the forehead may elicit pain, causing the physician to suspect erroneously frontal sinusitis. The understanding and diagnosis of facial pain are far more complicated than this
Pain in the forehead may be a frontal or ethmoid sinus problem or a muscle contraction tension headache (Fig. 8–1). Pain in the maxillary sinus may be located over the maxillary sinus or radiate to the canine teeth and into the temporal region (Fig. 8–2). Ethmoid sinusitis can produce pain most often in the medial canthal area, but also the pain can extend into the parietal and temporal areas and into the upper cervical area (Fig. 8–3). Sphenoid sinusitis will generally produce a retro-orbital headache, but it can extend to the temporal area, vertex, occiput, and even into the shoulder and canine teeth (Fig. 8–4).
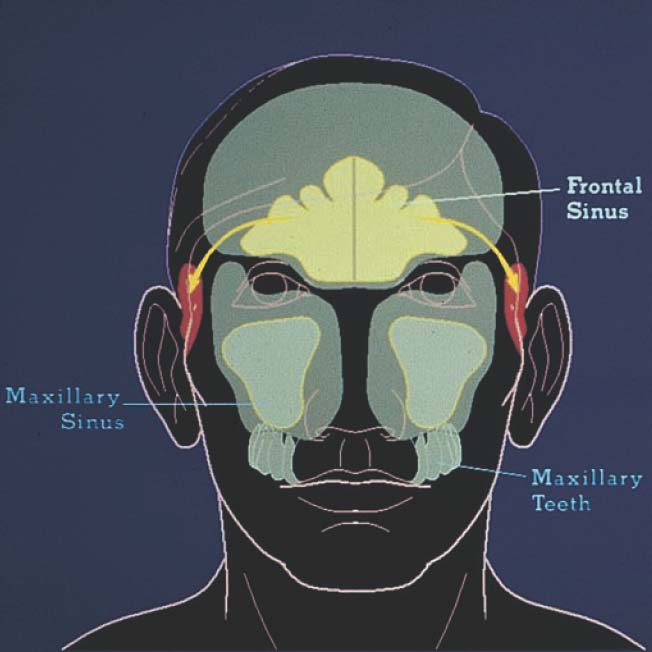
FIGURE 8–1 Pain in the forehead may be frontal or ethmoid sinus disease or muscle contraction tension headache.
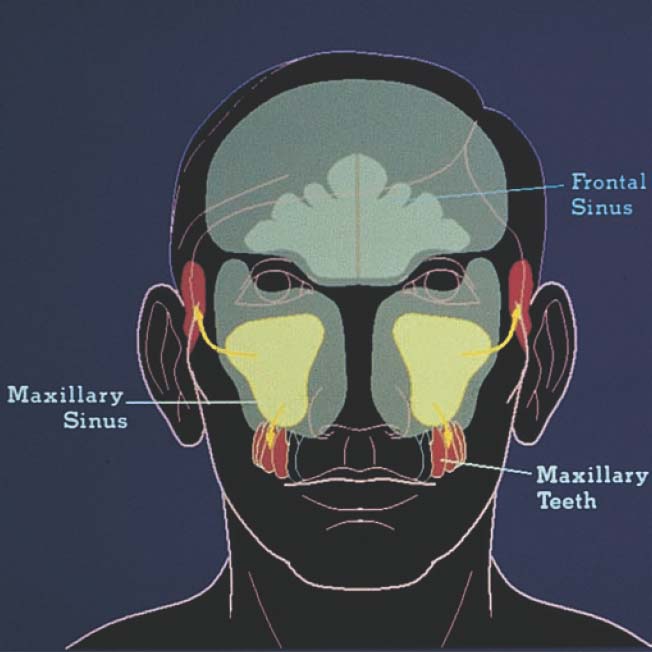
FIGURE 8–2 Pain in the maxillary sinus may be located over the maxillary sinus or radiate to the canine teeth and into the temporal region.
Although this breakdown of areas of pain is important and valuable, it is unusual for a patient to come to the physician with sinusitis in a single sinus. Involvement of multiple sinuses makes the pain and symptoms complicated. Multiple sinus involvement causes the pain to be in several locations, and for the patient with other causes of facial pain, the etiology may be confusing for the practitioner (Fig. 8–5). Therefore, it often takes some understanding of symptomatology to be certain about the diagnosis. This is especially true as it relates to the symptom of facial pain and pressure.
The headache history is important in trying to sort out the etiology of facial pain and pressure. It is important to know the location of the pain, the nature of the pain (steady, pulsating, squeezing, vicelike, stabbing, sharp, dull, mild, severe, etc.), and the duration and frequency of the headache. Many patients have more than one kind of headache. It is important to know how many kinds of headaches are present, what makes the headache better or worse, and whether there are associated symptoms such as aura, nausea, vomiting, photophobia, and phonophobia. It is important to know about associated nasal and/or sinus symptoms such as nasal obstruction, nasal drainage, and alteration in taste and/or smell.
Many years ago a physician, H. G. Wolfe, wrote a textbook on headaches.1 What Wolfe did was fascinating. He stimulated certain areas within the nasal cavity and showed to which head and neck locations pain was referred. If there is disease in the anterior nasal septum, such as ulceration, the pain was referred not only to the medial canthal area but also to the lateral part of the orbit (Fig. 8–6). Ulcerations like this can occur with atrophy of the nasal septum. This is seen in individuals with a severe nasal septal deviation and in some elderly individuals. Small polyps or edema putting pressure in the anterior ostiomeatal complex may cause disease isolated to the anterior aspect of the middle turbinate. Pain also may occur along the supratrochlear area (Fig. 8–7).
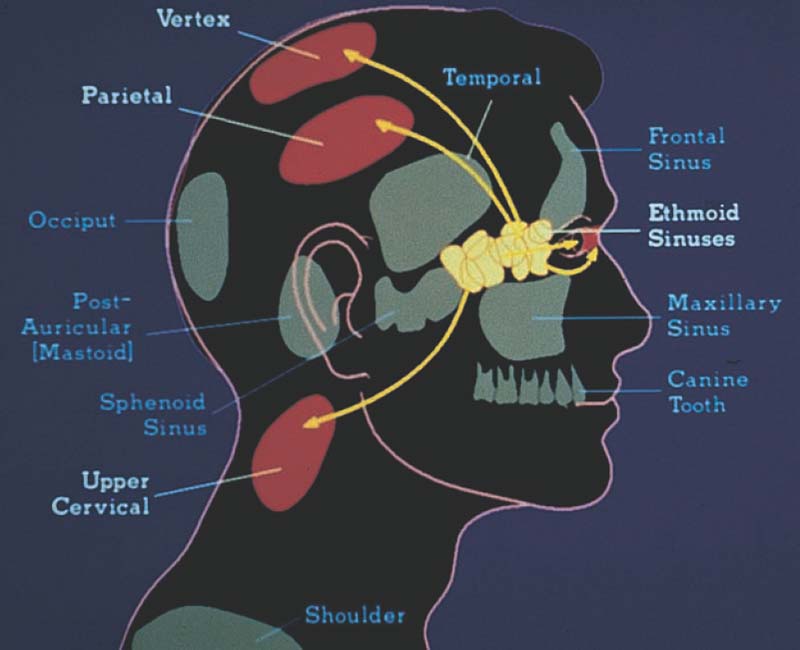
FIGURE 8–3 Ethmoid sinusitis can produce pain, most often in the medial canthal area. The pain also can extend into the parietal and temporal areas and into the upper cervical area.
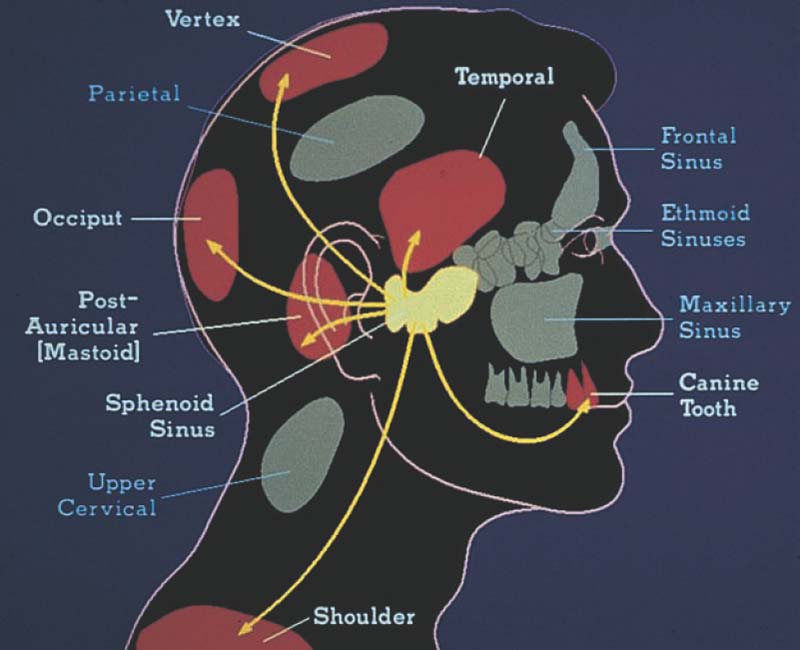
FIGURE 8–4 Sphenoid sinusitis will generally produce a retro-orbital headache, but it can extend to the temporal area, vertex, occiput, and even into the shoulder and canine teeth.
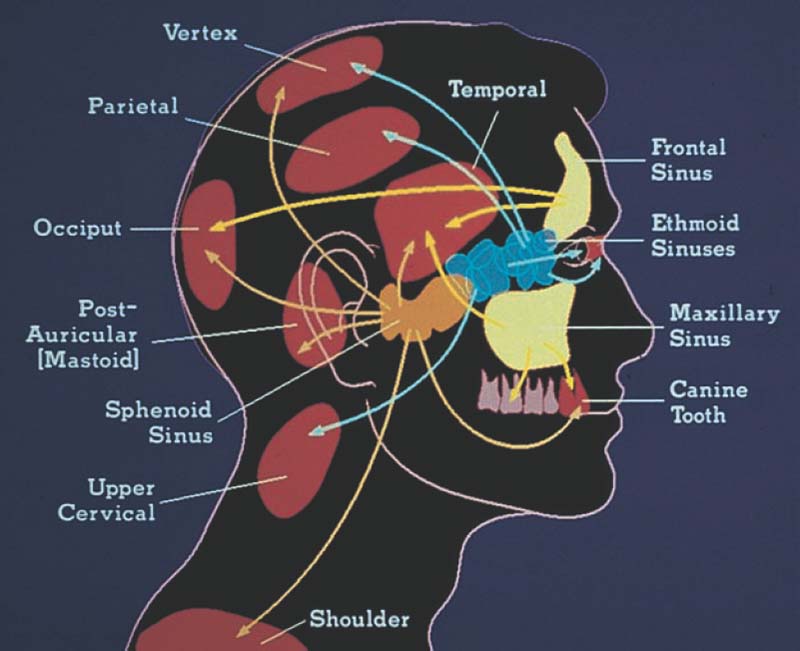
FIGURE 8–5 Multiple sinus involvement causes the pain to be in several locations. For the patient with other causes of facial pain, the etiology may be confusing.
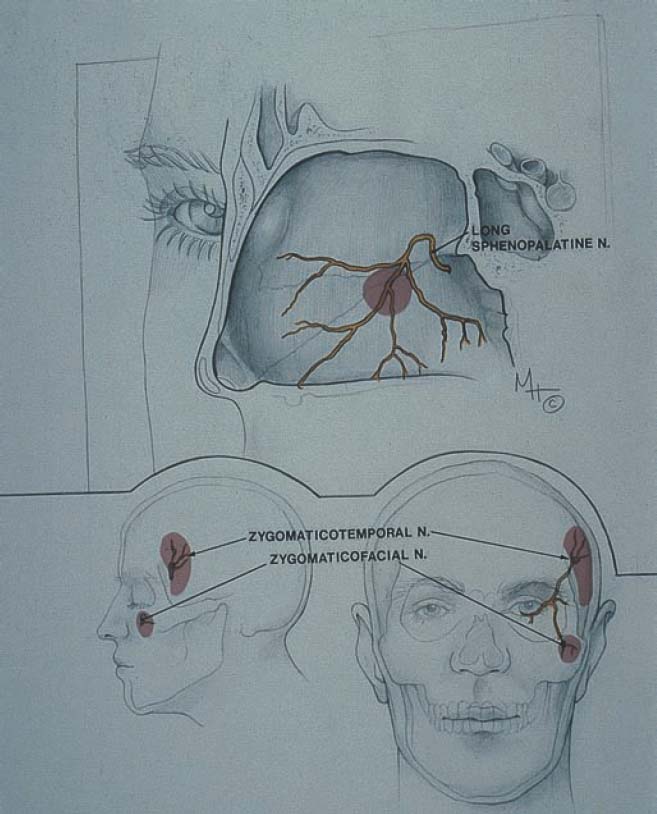
FIGURE 8–6 If there is disease in the anterior nasal septum, such as ulceration on the anterior septum, the pain was referred not only to the medial canthal area but also to the lateral part of the orbit.
Patients may have disease and/or pathology in the ostiomeatal complex, perhaps from polyposis, an abnormality of the middle turbinate, which with a small amount of edema puts pressure on this area. A paradoxically bent middle turbinate may be asymptomatic, but it can cause pressure in the middle meatus that at times can cause pain in these various areas (Fig. 8–8). Minimal pathology may cause edema in the anterior osiomeatal complex, resulting from air pollutants, nasal congestion, or allergies. Abnormalities of the uncinate process may also cause intermittent obstruction in the anterior ostiomeatal complex. The pain from pathology in this region is along the zygomaticotemporal nerve laterally into the temporal region (Fig. 8–9).
Disease may occur in the posterior ostiomeatal complex (sphenoethmoid recess) caused by abnormalities of the superior turbinate such as a concha bullosa, edema, or polyposis.
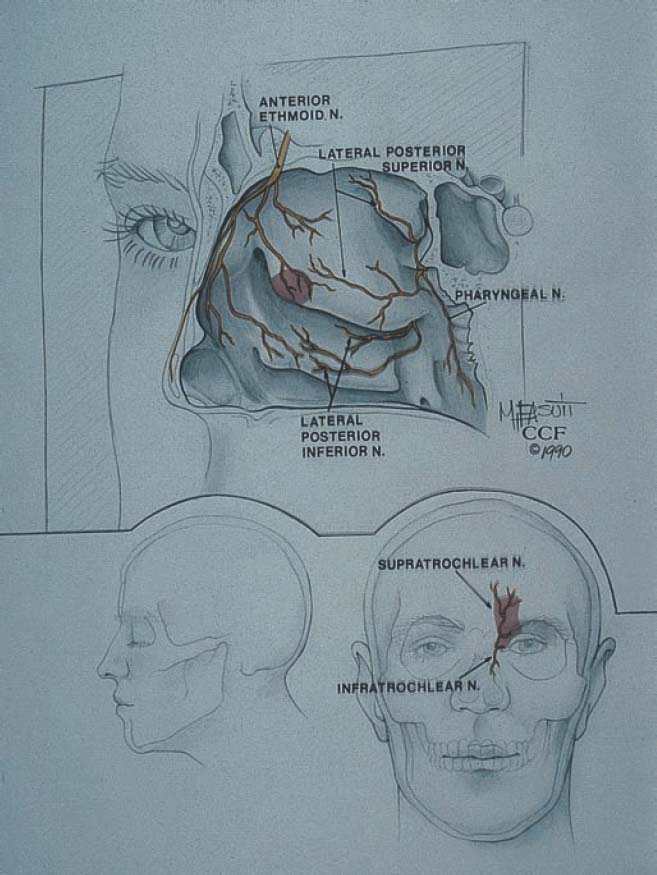
FIGURE 8–7 Small polyps or edema creating pressure in the anterior ostiomeatal complex may cause disease isolated to the anterior aspect of the middle turbinate.

FIGURE 8–8 A paradoxically bent middle turbinate may be asymptomatic, but it can cause pressure in the middle meatus that at times can cause pain in these various areas.
FIGURE 8–9 Abnormalities of the uncinate process may cause intermittent obstruction in the anterior osteomeatal complex. The pain from pathology in this region is along the zygomaticotemporal nerve laterally into the temporal region. The uncinate process may have several shapes, such as elongated (as seen on the right side) or short, thickened, and bent (as seen on the left side).
PEARL
It has become common for rhinologists and radiologists to refer to the middle meatus as the ostiomeatal complex. This region comprises the uncinate process, infundibulum, hiatus semilunaris, and the adjacent associated structures. It is reasonable to call this the “anterior” ostiomeatal complex because there is a similar region posteriorly. The superior turbinate, the front face of the sphenoid, and the nasal septum form the sphenoid ethmoid recess. This should be referred to as the “posterior” ostiomeatal complex.



