23

Dacryocystorhinostomy
Contemporary surgical techniques developed for the treatment of patients with obstructed paranasal sinuses can be similarly applied for the treatment of patients who present with epiphora or dacryocystitis from lacrimal obstruction. West1 first described intranasal drainage of an obstructed lacrimal sac in 1914. Since that time a variety of intranasal dacryocystorhinostomy (DCR) approaches have been utilized for the successful treatment of lacrimal obstruction.2,3 Until recently, however, the clinical applicability of intranasal DCR has remained limited because of difficulty with visualization and exposure of the lacrimal sac when operating in the narrow confines of the superior nasal cavity. With the introduction of endoscopic instrumentation for nasal surgery, technical difficulties with intranasal access to the lacrimal sac have been largely overcome.4–7 In addition to avoiding a skin incision, endoscopic DCR enables the surgeon to identify and correct common intranasal causes of DCR failure, such as adhesions, an enlarged middle turbinate, or an infected ethmoid sinus.
 Endoscopic Anatomy
Endoscopic Anatomy
From an endoscopic intranasal perspective, the lacrimal sac can be found beneath the bone of the lateral nasal wall just anterior to the attachment of the middle turbinate (Fig. 23–1). The superior border of the sac may extend above the level of the turbinate attachment. The posterior edge of the sac often extends beneath the middle turbinate, behind a landmark referred to as the maxillary line. The maxillary line is an important landmark for endoscopic DCR. It is readily identified as a curvilinear eminence along the lateral nasal wall that runs from the anterior attachment of the middle turbinate to the root of the inferior turbinate. Its location corresponds to the suture line between the maxillary and lacrimal bones that runs in a vertical direction through the lacrimal fossa. Exposure of the posterior half of the sac typically requires removal of the thin uncinate process and underlying lacrimal bone located posterior to the maxillary line. In contrast, exposure of the anterior sac necessitates removal of thicker bone located just anterior to the maxillary line. As the nasolacrimal duct courses inferiorly, it passes an average of 10 mm (range 8–17 mm) anterior to the natural ostium of the maxillary sinus. Injury to the duct can occur if the maxillary ostium is enlarged too far in an anterior direction. In clinical practice this injury is relatively uncommon because the hard surrounding maxillary bone protects the duct.
The inferior end of the lacrimal sac tapers as it enters the nasolacrimal canal formed by the maxillary, lacrimal, and inferior turbinate bones. The nasolacrimal duct runs within this osseous canal for a distance of ~12 mm. It continues beneath the inferior turbinate as a membranous duct for an additional 5 mm before opening into the inferior meatus. The duct orifice is found at the junction of the middle and anterior thirds of the meatus ~8 mm behind the anterior tip of the inferior turbinate and 29 mm from the anterior nasal spine. It is often covered by a flap of mucosa, known as Hasner’s valve, which is thought to prevent reflux of nasal secretions. Gentle pressure over the medial canthal region will often produce fluid or bubbles at the duct orifice to confirm its location.
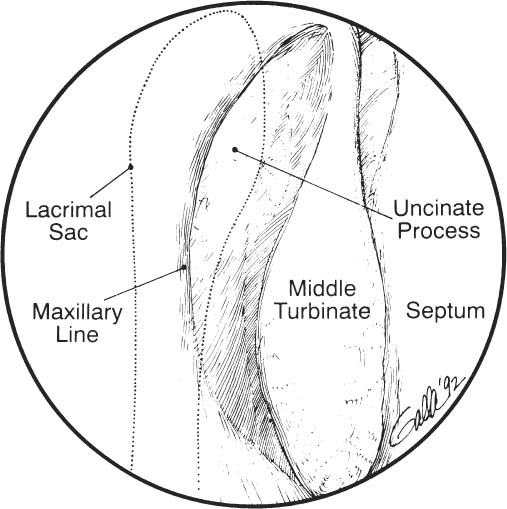
FIGURE 23–1 Endoscopic view of right nasal cavity shows location of the lacrimal sac (dotted outline) underlying the lateral nasal wall. The maxillary line, a bony eminence that originates at the attachment of the middle turbinate, corresponds to a vertical suture line that runs through the lacrimal sac.
 Surgical Technique
Surgical Technique
Endoscopic DCR may be performed under either local or general anesthesia, depending on the condition of the patient and the preference of the surgeon. The operation is typically performed with a video camera attached to the endoscope, so that the assistant surgeon can observe the entire procedure on a video monitor. With the patient supine and the head slightly elevated to decrease venous pressure at the operative site, nasal packing soaked in a 4% cocaine solution is placed along the lateral nasal wall to initiate mucosal decongestion. The nose and affected eye are draped in the operative field. A 0-degree, 4 mm diameter nasal endoscope is used for visualization, as submucosal injections of 1% lidocaine HCl with epinephrine 1:100,000 are placed in the middle turbinate and the lateral nasal wall just anterior to the attachment of the turbinate.
Surgical dissection is begun with removal of an ~1 cm diameter circle of mucosa and bone along the lateral nasal wall overlying the lacrimal sac. Initial tissue removal usually includes a portion of the uncinate process located posterior to the maxillary line. An air space is often entered that corresponds to the infundibulum or an anterior ethmoid air cell overlying the lacrimal sac. As dissection is carried more anteriorly, the lacrimal bone is opened, and the underlying medial wall of the sac will be exposed.
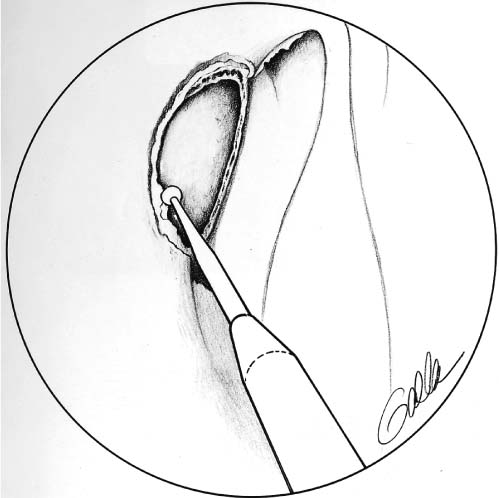
FIGURE 23–2 Once mucosa has been excised from the lateral nasal wall in the region of the maxillary line, a drill is used to remove thick bone overlying the lacrimal sac. It is important that bone anterior to the maxillary line is removed to expose the entire medial sac wall.
Next, the maxillary bone, which forms the anterior aspect of the lacrimal fossa, must be removed. Removal of this relatively thick bone is technically the most difficult step of the surgery. Bone removal may be accomplished with a curette, bone-biting forceps, microdebrider, or drill (Fig. 23–2). The surgical laser also has been used for endoscopic DCR because of its ability to remove bone with excellent hemostasis.8 After the medial sac wall has been exposed, it is entered with an angled Blakesley forceps. Use of the laser provides for a more hemostatic sac opening, whereas the forceps allow for a tissue specimen to be obtained for pathologic examination to rule out occult neoplasm. It is often helpful to use a lacrimal probe within the sac to tent up the medial sac wall as it is opened. This maneuver serves to isolate the medial wall and prevent inadvertent injury to the underlying structures. Once the sac is entered, the probe will be visible.
PEARL
A light pipe may be inserted into the punctum, illuminating the sac and overlying bone and making the identification of the sac easier. The light pipe also serves to tent up the lacrimal sac mucosa.



