Surgical Approach to the Rectus Muscles
Albert W. Biglan
The earliest reports of the use of a procedure to correct strabismus occurred in the middle of the 18th century, when an itinerant charlatan, Chevalier, John Taylor, proceeded from city to city in Europe, with an entourage of coaches and assistants, performing procedures to treat cataracts and to correct strabismus. For the strabismus procedure, he immobilized the patient by having the subject’s head held securely by a masked fool. Taylor probably performed an incidental tenotomy when taking a snip of conjunctiva. He thought that he was cutting the nerve to the muscle. The patient’s eyes were patched, and instructions were given to remove the patch no sooner than 3 days after the procedure. Taylor then had sufficient time to collect his fee and leave town, placing a comfortable day or two between a dissatisfied patient and the “surgeon.”1,2,3,4 The results of Taylor’s procedure are not reported.
In 1839, Johann Freidrich Dieffenbach, of Berlin, successfully performed the first myotomy of an internal rectus muscle.1,2,3,4,5 Surgery was performed without antisepsis or skin preparation; the patient sat in a chair during the procedure. Even though Dieffenbach’s procedures were performed before general anesthesia was available, restraint of the patient was discouraged. Three assistants, and as many as seven instruments, were used to perform the procedure. An incision was made into the nasal conjunctiva, and muscle tissue was brought into the wound and severed.5 The operation was considered to be “among the most valuable surgical improvements of this age.”5 Florent Cunier performed a myotomy of a lateral rectus only 3 days after Dieffenbach’s procedure.4,6
Jones,7 in an 1847 textbook on the principles and practice of ophthalmic medicine and surgery, showed the primitive level of understanding of the causes and nonsurgical treatment of strabismus. One of the treatments for convergent strabismus included a “calomel purge or two,” or mercurial chalk given orally with a laxative, followed by “tonics.” When these measures failed, “section of the internal rectus muscle” was recommended. To accomplish this treatment, a vertical incision was made through the conjunctiva, and the internal rectus muscle was grasped with toothed forceps. A bent probe or a blunt hook was placed behind the tendon of the internal rectus, and the tendon was cut from its insertion, resulting in a free tenotomy. Two assistants were recommended, one to separate the eyelids and one to sponge blood to provide better visualization. Scleral perforation with loss of vitreous was listed as an uncommon complication.7
In 1853, von Graefe recommended performing a tenotomy at the insertion rather than a myotomy. He should be credited with providing a better understanding of the anatomy of the extraocular muscles. He refined the procedure by applying information gained after cadaver dissection. He recommended preserving Tenon’s capsule and the “muscle sheaths.”3 He also introduced new instrumentation to perform surgery.
In 1892, in a translated textbook of ophthalmology by Fuchs, Duane recounted recent advances in strabismus surgery.8 Topical application of cocaine was used for anesthesia. If convergent strabismus was found to be large, surgery was performed on both eyes. The surgical technique used at the end of the 19th century consisted of grasping the internal rectus muscle with forceps through a conjunctival incision made over the muscle insertion. The muscle was cut from its insertion. If an overcorrection occurred, advancement of the internal rectus muscle was recommended. This maneuver was accomplished by passing a silk suture through the conjunctiva at the limbus and attaching it to the muscle that was subsequently retrieved with a forceps. Scarring of the conjunctiva was recognized as a complication, as were exophthalmos and “sinking in of the caruncle.”8
Patients with divergent strabismus were treated with tenotomy of the lateral rectus muscle with a similar technique. Overcorrections were reported as “uncommon.” Tenotomy of the inferior rectus muscle was advocated to elevate eyes that had an inferior iris coloboma so that the visual axis could pass through the coloboma.8
In 1913, in a book titled Ophthalmic Surgery, Metter and Sweet9 recommended the use of a local anesthetic, either topical or subconjunctival, for muscle advancement procedures. To weaken the internal rectus muscle, a tenotomy was performed at the insertion of the muscle. They graded the effect by regulating the extent of the tenotomy. If an eye was undercorrected, silk support sutures were secured at the temporal limbus, passed through the upper and lower eyelids, and tied externally for 24 hours to hold the eye in an abducted position. If the operation produced an overcorrection, a “counteracting suture” was added. This suture was placed through the conjunctiva at the nasal limbus, passed back through the muscle tendon, and tied on the conjunctival surface. A tenotomy combined with an advancement procedure of the ipsilateral antagonist muscle was recommended to treat the “highest grades” of convergent strabismus.9
In 1936, in an essay on the treatment of concomitant strabismus, Travers10 stated that tenotomies of the medial rectus muscle “yielded unsatisfactory results” because “there were three times as many overcorrections as satisfactory results.” He recommended a recession of the internal rectus muscle combined with an advancement procedure of the lateral rectus muscle, to treat convergent strabismus. Surgery was performed “early”; in most cases, patients were between 3 and 6 years old. To recess a muscle, three fine chromic catgut sutures were inserted into the sclera as far behind the old insertion as one wished to displace the muscle. Sutures were passed through a portion of the muscle, which was held with a Prince forceps.10
Over the last four decades, three techniques for gaining access to a rectus muscle have been described. In 1954, Swan and Talbot11 advocated making a vertical conjunctival incision behind the insertion of the muscle. This incision was followed by a second incision into Tenon’s capsule that was made parallel to the rectus muscle. “Intermuscular membranes are cut with blunt tipped scissors and fine absorbable sutures, threaded on small atraumatic cutting needles,” were used to secure the muscle to its new position.
Two approaches were described in the 1960s. von Noorden12 used illustrations to detail the steps needed to gain access to a rectus muscle through an incision made at the limbus. A conjunctival incision was made at the limbus with blunt-tipped scissors. The conjunctiva and Tenon’s tissue anterior to the muscle insertion were reflected so that the muscle could be visualized directly. Following these steps, a recession or resection of the muscle could be performed.
In 1968, Parks13 described the fornix (cul-de-sac) incision for horizontal rectus muscle surgery. Previous techniques had used an approach to the rectus muscles in which incisions were made directly over or just anterior to the muscle. The fornix approach was unique because the incision was made behind the eyelid on the bulbar conjunctival surface, just above the cul-de-sac, or near the lower fornix of the lower eyelid.
The location of the rectus muscle is identified with a Stevens’ hook, which is replaced with a Green’s hook. The muscle is moved into the incision by reflecting the conjunctiva and Tenon’s capsule over the Green’s hook. At the completion of the operation, the wound is left unsutured. Both recession and resection procedures of the horizontal rectus muscles can be performed with this technique. This incision has been adopted to approach the vertical rectus muscles and the oblique muscles.
Recently, these suture techniques have been refined or improved. The introduction of adjustable sutures has provided the surgeon greater precision in achieving ocular alignment.14 The hang-back recession technique provides the ability to perform larger recessions of the rectus muscles safely, with reduced risk of scleral perforation. The augmented recession techniques have permitted large deviations to be corrected with surgery on fewer muscles.15,16,17 Posterior fixation or retroequatorial myopexy has enabled the surgeon to treat incomitant forms of strabismus.18,19
Over the last 40 years, it has become evident that great respect must be given to the Tenon’s capsule tissue that surrounds the extraocular muscles. It is important to minimize tissue trauma if restriction of movement of the globe is to be avoided. The use of excessively deep and frequent passage of muscle hooks in search of a muscle can result in bleeding and incorporation of fat and Tenon’s tissue. This damage can produce fibrosis, which later may produce restricted eye movements. Surgery now is performed with magnification and focal illumination.
There have been changes in instrumentation. Helveston has redesigned and modified instruments to perform strabismus surgery in a less traumatic and more precise fashion. (Katina Products, Inc., Denville, NJ 07834) The replacement of catgut suture with synthetic absorbable suture material has increased the reliability of securing the muscle to its new insertion. These biodegradable synthetic materials have reduced tissue reaction and decreased the tissue response to healing. The fine-wire needles with spatulated tips enable the surgeon to secure the muscle to the globe with greater safety and accuracy. The amount of muscle to be resected or recessed usually is measured to the nearest 0.5 mm. The amount of surgery performed is graded to the size of the alignment defect, the degree of restriction of movement of the globe, and the presence of paresis of the extraocular muscles.
The form of anesthesia used has come full circle; once again, ophthalmologists are returning to the use of topical and subconjunctival anesthetics to approach the extraocular muscles.20,21,22,23 For the last three decades, most strabismus surgery has been performed in outpatient or surgical short-stay facilities.
INDICATIONS
Surgery on the extraocular muscles is recommended when optical and other nonsurgical measures have not corrected strabismus. Surgery on a rectus muscle may be undertaken to align the eyes; eliminate diplopia; restore binocular vision;24,25,26,27,28 correct an abnormal head posture; reduce restricted eye movements; reduce nystagmus; enhance binocular function; prevent abnormal sensorial adaptations to strabismus; decrease asthenopia; and in rare situations, perform a biopsy on an extraocular muscle. In addition, surgery may be performed to increase the field of vision for a patient with an esotropic eye,29,30,31 repair trauma or disruption of an extraocular muscle, improve a patient’s appearance and ability to secure employment,32 enhance a child’s self-image,33,34,34a or provide patients with the ability to achieve comfortable eye-to-eye contact.
TIMING
Most surgeons will correct infantile forms of strabismus after a patient is 6 months old. Usually, a child takes up to 4 to 5 months to develop a strong fixation reflex. If a patient is born prematurely and has strabismus, a waiting period that is 6 months from the expected normal 40-week gestational date is recommended. For other forms of comitant strabismus, rectus muscle surgery is performed after nonsurgical measures are unsuccessful and there is stability in the size of the deviation. A waiting period of at least 6 months is suggested before incisional surgery is performed to correct paralytic strabismus. In some cases, occupational or other considerations may justify exceptions to this guideline. Further discussion of the indications for the treatment of specific problems is covered in their respective sections.
CONTRAINDICATIONS
Contraindications to rectus muscle surgery may be absolute or relative. An absolute contraindication is an inadequate understanding of the patient’s strabismus problem or uncertainty as to which muscle or muscles must be repositioned to correct the problem. For example, surgery on a horizontal rectus muscle rarely corrects symptoms related to torsional diplopia. Another absolute contraindication is the presence of a health problem that limits life or precludes the safe administration of anesthesia. In these cases, alternative methods of treatment may be considered, such as the use of botulinum A toxin.
Relative contraindications include guidelines as to when to avoid or postpone surgery, but exceptions may occur. Surgery is relatively contraindicated when measurement of the size of a deviation is variable or inconsistent.
Patients who are young enough to be treated for amblyopia should have treatment to correct the amblyopia before undergoing surgical alignment of the eyes.
If two rectus muscles have been removed previously, detaching a third or fourth rectus muscle should be avoided because doing so may compromise the vascular circulation of the anterior segment of the eye and produce anterior segment ischemia or necrosis.35
Additional relative contraindications include operating on a patient’s dominant or preferred eye and operating on a patient who has one useful eye. For example, a monocular patient may have a face turn caused by nystagmus with a null point. A recess-resect procedure or a monocular Kestenbaum operation may be considered. In these situations, the patient and the parents should be informed of the remote risk of the development of a surgically related problem that may cause reduced vision. Surgeons should be cautious about performing surgery on a child whose parents have an unrealistic expectation of the result.
SURGICAL PROCEDURE
Two approaches are used to access the rectus muscles: the fornix approach and the limbal approach. The advantages and disadvantages of these procedures are listed in Tables 1 and 2.
Table 1. Advantages of Surgical Approaches to the Rectus Muscles | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 2. Disadvantages of Common Surgical Approaches to the Rectus Muscles | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The type of anesthetic is chosen after consultation between the parent or patient and the surgeon. During this discussion, the advantages and disadvantages of each form of anesthesia should be explained and the most suitable form selected. The surgeon should assist the parent or patient in choosing the anesthetic. The use of a general anesthesia is most suited for the young or anxious patient. If the surgeon anticipates difficulty with the procedure, such as a re-operation, or if a “lost” muscle is going to be “found,” general anesthesia is the preferred technique. If both eyes require surgery, it is undesirable to administer a retrobulbar anesthetic that temporarily may decrease the patient’s visual acuity. In these situations, topical, perimuscular, or general anesthesia is preferred.
If the result of forced duction testing is critical in determining the amount of surgery to be performed, a local or topical anesthetic may be considered. During general anesthesia, the use of a depolarizing agent, such as succinylcholine, can alter the tone of the extraocular muscles temporarily. This alteration may affect the result of forced duction testing.36 The increased tone of the extraocular muscles can be avoided with the use of a nondepolarizing agent, such as pancuronium. If postoperative suture adjustment is required, it may be several hours before the patient recovers sufficiently from general anesthesia to permit the adjustment to be performed.
Local anesthesia has been used for strabismus surgery for two centuries. Recent advances have made local anesthesia the preferred anesthetic in mature, cooperative patients.23 Because of the myotoxicity of bupivacaine, this agent should be avoided if a retrobulbar block will be used.37 Intravenous sedation with fentanyl citrate combined with midazolam will prepare cooperative adolescents for the administration of either retrobulbar anesthetic (1.0 to 2 ml of a 2% mepivacaine (Carbocaine) solution or a perimuscular block injected subconjunctivally over the muscle insertion. Topical anesthetic, either 4% lidocaine hydrochloride or a 1% to 4% solution of cocaine supplemented with intravenous sedation also may be used. The latter methods provide the patient with anesthesia of the globe without akinesia and permit the patient to participate in suture adjustment in the operating room if needed.
Table 3 lists instruments that are used frequently for strabismus surgery.
Table 3. Surgical Instruments Commonly Used for Strabismus Surgery | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
PREPARATION
Instrument selection is reviewed by the surgeon (Fig. 1). The patient is positioned so that the head is stabilized, and a shoulder bolster or “roll” is placed under the patient’s shoulders to extend the neck slightly (Fig. 2A). The patient is identified, as is the eye to receive surgery (see Fig. 2B).
 Fig. 1. Instruments to be used are checked by the surgeon. |
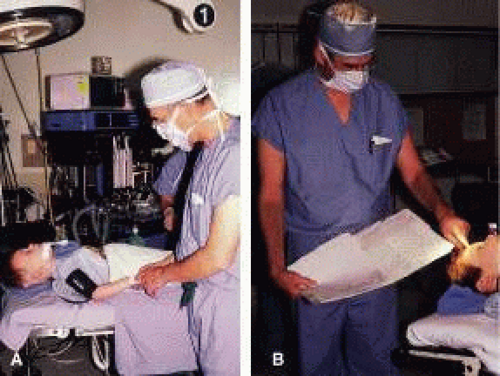 Fig. 2. A. The patient is positioned with the head slightly extended. B. The surgeon identifies the patient and the correct eye; the clinical record is checked before proceeding with the procedure. |
The eyelids and surrounding skin are prepared with two scrubs using a 10% povidone iodine (Betadine) solution that is diluted 50:50 with warm saline38,39,40,41 (Fig. 3A and B). The conjunctival cul-de-sacs are irrigated with a bulb syringe and warm saline. Silver protein precipitating solutions, such as Argyrol are not used. A drop of 1% phenylephrine hydrochloride may be instilled into the conjunctival cul-de-sacs to reduce conjunctival bleeding (Fig. 4). The surgical field is isolated with a sterile adhesive barrier drape (see Fig. 4 and Fig. 5). The instrument tray is positioned, and sterile cotton-tipped applicators are placed on either side of the head so that they are available for sponging the field (Fig. 6). A wet-field or bipolar cautery is available. The surgeon is seated at the head of the operating table. The assistant sits to the left of the surgeon, and the surgical technician sits to the right (Fig. 7). Consistency in the procedures that are used to prepare a patient for surgery, such as positioning of the patient and location of the surgeon and the assistants, helps to eliminate confusion among the operating room staff before each procedure. Surgical instruments can be placed on a Mayo stand if a surgical technician is not available to pass instruments to the surgeon (see Fig. 6). The clinical record is positioned where the surgeon can refer to it.
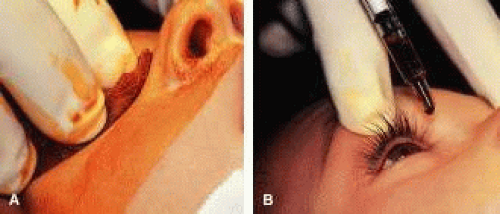 Fig. 3. A. The periorbital tissues are cleansed with two scrubs of povidone iodine (Betadine) solution diluted with warm saline. B. A drop of 5% povidone iodine is instilled into the conjunctival cul-de-sac. |
 Fig. 4. A drop of 1% of phenylephrine hydrochloride is instilled into the conjunctival cul-de-sac. |
 Fig. 5. An adhesive barrier drape is used to isolate the surgical field. |
 Fig. 6. The patient after the adhesive barrier drape has been applied. A Mayo stand provides easy access to instruments if a resident assistant is not available. |
 Fig. 7. The surgeon sits at the head of the operating room (OR) table. The assistant is to the surgeon’s left. The surgical technician is positioned to his or her right. |
RECESSION PROCEDURE: FORNIX INCISION
This procedure is recession of the right medial rectus muscle. The eyelids are separated with a Barraquer open-blade wire eyelid speculum (Fig. 8). The open-blade design provides more room for exposure and makes it easier to pass the suture needles, especially in small children or when large recessions are performed. The globe is grasped with a Lester forceps at the limbus. It is best to grasp the limbus with the forceps held perpendicular to the globe and then to position the forceps so that they are rotated and lie tangential to the globe. Forced ductions are performed to detect any restriction of movement of the globe (Fig. 9).
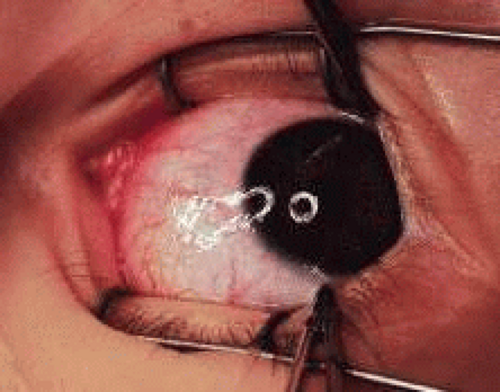 Fig. 8. The lids are separated with a Barraquer open-blade wire speculum. The eye is abducted to test for restriction. |
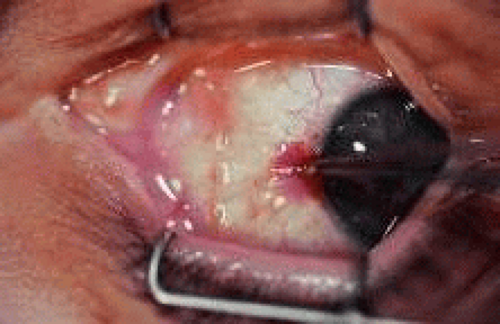 Fig. 9. A Lester forceps grasps the limbal conjunctiva to perform a forced duction test. Care is taken not to allow the globe to move posterior during this maneuver. Restriction of globe rotation should be recorded, and, if it is significant, adjustments in the surgical procedure may be considered. |
The globe then is gently elevated from the orbit or proptosed at the same time it is abducted or adducted to prepare for the incision. Elevation of the globe helps to separate the horizontal rectus muscle from the inferior rectus muscle so that the inferior rectus muscle is not cut when the incisions are made. The conjunctiva is grasped by the assistant with a Manhattan toothed forceps (Fig. 10). This forceps has teeth that are angled outward and are designed to grasp conjunctiva, as well as the deeper subconjunctival tissue, so that when the blunt-tipped Westcott scissors cuts into the tented tissue, an incision is made into the conjunctiva and Tenon’s capsule (Fig. 11A and B). If the incision does not completely penetrate Tenon’s capsule and the intermuscular septum to the scleral surface of the eye, additional tissue (anterior Tenon’s tissue and/or intermuscular septum) is grasped with the Manhattan forceps and at least one additional cut is made.
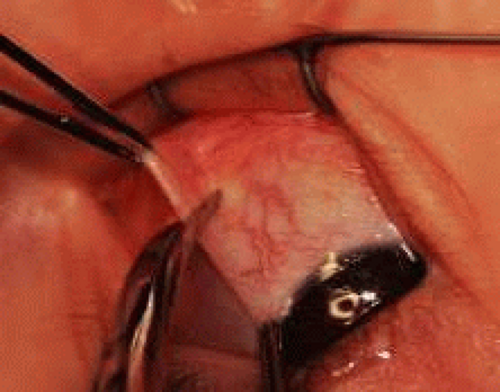 Fig. 10. The conjunctiva is tented between two forceps. |
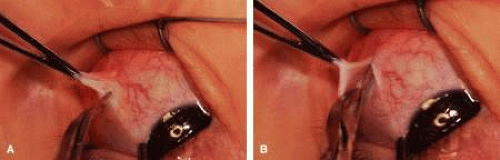 Fig. 11. A. A blunt-tipped Westcott scissors, held perpendicular to the globe, is used to make an incision through the conjunctiva, Tenon’s tissue, and intermuscular septum. B. In this view, the surgeon is spreading the scissor blades and viewing bare sclera. |
A Stevens’ tenotomy hook is passed by the surgeon into the incision and is rotated so that it can be slid underneath the muscle insertion with the tip of the hook held tangential to the globe (Fig. 12). The hook should be passed 2 to 3 mm posterior to the expected location of the muscle insertion. Care is taken not to incorporate intramuscular septum or other adventitial tissue on the hook. When the lateral rectus muscle is secured with the Stevens’ or Jameson muscle hook, care should be taken not to bring the inferior oblique muscle up to the insertion (Fig. 13). When the muscle is secured with the Stevens’ hook, the hook and the inferior edge of the muscle insertion are elevated and a Jameson muscle hook is passed between the tented muscle tissue and the sclera to secure the muscle at its insertion (Fig. 14). Care is taken to include the entire insertion of the tendon on the hook. The tip of the Jameson hook is gently elevated by depressing the heel of the hook. This maneuver helps to ensure that the entire tendon of the muscle remains captured on the hook. A Stevens’ tenotomy hook is placed in the incision, this time anterior to the insertion beneath the conjunctiva (Fig. 15). The Stevens’ hook is passed posterior over the orbital surface of the muscle (Fig. 16). Gentle pressure on the Stevens’ hook is directed posterior so that the check ligaments and Tenon’s tissue that overlie the muscle belly are separated from the muscle capsule with blunt dissection. The hook usually is passed posterior for about 10 mm. When recessing a lateral rectus, attachments between the underside of the lateral rectus and inferior oblique are broken (Fig. 17). Two or three passes over the muscle are made, and, with simultaneous countertraction on the Stevens’ hook and the Jameson hook, the conjunctiva is elevated and pulled over the tip of the Jameson hook (Fig. 18A and B).
 Fig. 12. The incision is held open with a Manhattan forceps. A Stevens’ tenotomy hook is introduced into the incision. The hook is being placed under the rectus muscle without dragging Tenon’s tissue and intermuscular septum into the insertion. |
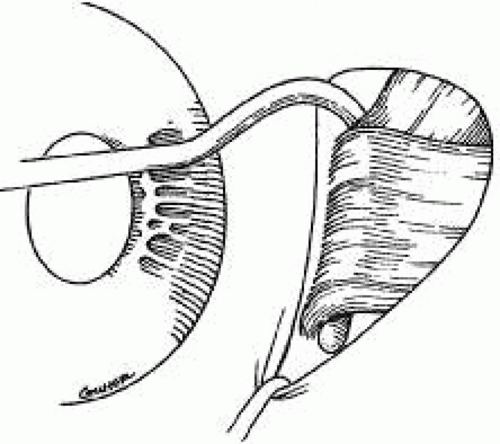 Fig. 13. When approaching the lateral rectus, the inferior oblique muscle can be brought up to the lateral rectus insertion. In this instance, the tendon of the lateral rectus muscle should be separated from the inferior oblique muscle with blunt dissection and repositioned back into the incision. |
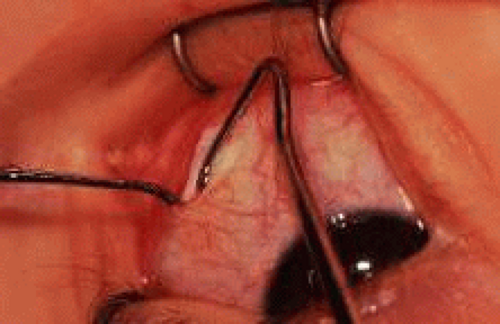 Fig. 14. A Jameson hook is used to spread the incision open with countertraction against the Stevens’ hook, which is under the rectus muscle. Then, the Stevens’ hook elevates the conjunctiva and the muscle insertion. The Jameson muscle hook is inserted underneath the Stevens’ hook to secure the entire insertion of the tendon of the rectus muscle. |
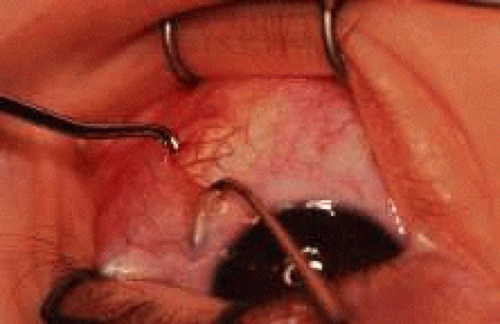 Fig. 15. The Jameson hook has been placed under the rectus insertion. A Stevens’ tenotomy hook is introduced anterior to the muscle insertion, and with an anterior-posterior movement, the conjunctiva is bluntly dissected free from the anterior extension of the rectus muscle. The Stevens’ hook is moved anterior underneath the conjunctiva to approximately 3 or 4 mm anterior to the rectus muscle insertion. It is then passed over the insertion and directed posterior, following a path similar to the course of the muscle from its origin. The hook is carefully passed posterior for about 8 to 10 mm to separate adhesions between the muscle capsule and the overlying Tenon’s tissue. |
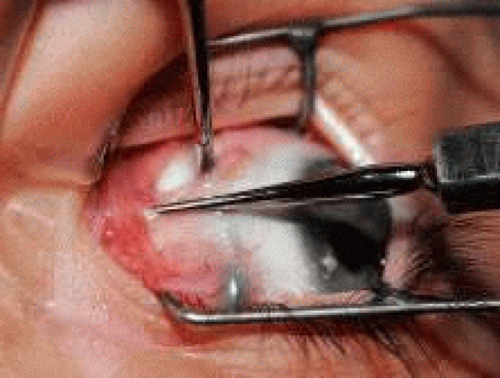 Fig. 16. Countertraction between the Stevens’ hook and the Jameson hook will open the incision over the muscle insertion, exposing the muscle tendon on the Jameson hook. The intermuscular septum and anterior Tenon’s capsule remain at the upper pole of the insertion. Exposure is provided by a Stevens’ tenotomy hook.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|