Surgical and Nonsurgical Trauma
Kevin Engel
Michael Page
Sandra Montezuma
J. Douglas Cameron
NORMAL OCULAR WOUND HEALING
Successful wound healing in the eye is a precise, ordered series of events that results in reestablishment of functional ocular anatomy.1
The goal of therapeutic intervention in the setting of accidental ocular trauma and ophthalmic surgery is to promote the repair process and to allow it to proceed as rapidly as possible. In addition, one needs to restore ocular architecture as completely as possible without compromising ocular function.2
Cellular and Extracellular Components
The four basic cell types participating in wound healing are fibroblasts (fibromyocytes), vascular endothelial cells, inflammatory cells (many types), and surface epithelial cells. Specialized cell types that participate in ocular wound healing include corneal endothelial cells, retinal pigment epithelial cells, and Müller cells of the retina.
Specific cell populations enter an area of injury under the influence of complex biochemical and biophysical processes involving proteins of the extracellular matrix and the coagulation system. Intracellular proteins, such as tubulin and actin, and myosin filaments function in cell locomotion. Extracellular matrix proteins, such as fibronectin, laminin, and type IV collagen, orient and regulate cell migration and adhesion.3 Coagulation proteins, such as von Willebrand’s factor and plasminogen, also function in regulating the cellular events of healing. Vascular endothelial cells of regional intact vascular channels are stimulated to leave their resting state, digest basement membrane, proliferate, migrate, and eventually differentiate under the direction of multiple angiogenic growth factors.4
A wound usually is filled initially by fibrin coagulum. Neutrophils, lymphocytes, and histiocytes (macrophages) enter the wound along the fibrin scaffolding to clear necrotic debris and confine toxic or foreign substances.
Granulation tissue often is the first type of reparative tissue in wound healing (Fig. 6.1). Although its composition varies somewhat depending on the tissue environment, small-caliber vascular channels in a delicate collagenous stroma infiltrated by acute and chronic inflammatory cells are the basic components. This amorphous tissue serves as a template for more definitive repair.
Metaplasia is the transformation of a cell population from one adult cell phenotype to a second cell phenotype. In advanced wound healing, fibroblasts acquire intracytoplasmic characteristics of smooth muscle cells (myofibroblasts).5 The myofibroblasts are able to contract and bring wound edges together.
Vascular endothelial cells proliferate and migrate into the wound from preexisting adjacent vessels. The new “vessel” migrates initially as a solid bulb of endothelial cells. This solid cord of cells will canalize and differentiate into mature arterioles, venules, and capillaries. Fibroblasts grow into the wound in a radial manner but will eventually reorient and secrete collagen along lines of established tissue tension.
Epithelial cells cover and protect surfaces of tissue. Two distinct types of epithelial cells cover the ocular surface: corneal epithelial cells and conjunctival epithelial cells. Cell replacement is accomplished by division of stem cells located at the limbus for the corneal epithelium6,7 and at the mucocutaneous junction and possibly throughout the conjunctiva for the conjunctival epithelium.8 Migration and proliferation of surrounding healthy epithelial cells restores surface continuity.
Apoptosis is a fundamental cell population control process leading to programmed cell death. Cell death in apoptosis results from intracellular messages generated in response to intracellular conditions. In necrosis, cell death results from toxic external factors (e.g., hyperosmolality). Apoptosis allows for elimination of entire populations of cells without damage to surrounding cells and does not stimulate an inflammatory response.9 Elimination of certain cells is advantageous in embryology (e.g., when scaffolding structures are no longer necessary as with the primary vitreous). In certain neoplastic conditions, however, defects in apoptosis may lead to disadvantageous accumulation of cells. Apoptosis also seems to be highly influential in all types of inflammation, including wound healing. In wound healing, apoptosis may function to control the type and degree of tissue response. In the anterior cornea, keratocytes have been observed to undergo apoptosis during wounding of the cornea.10 Abnormalities of apoptosis may be responsible for such conditions as keloid formation in the skin, keratoconus, and the formation of pterygia.11,12,13,14
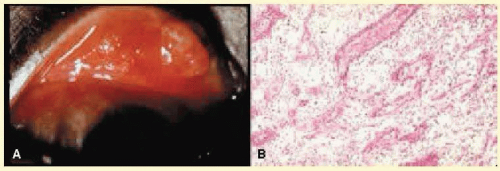 FIG. 6.1 Granulation tissue. A: Clinical photograph of granulation tissue (often mistakenly called a pyogenic granuloma) at the site of a ruptured chalazion. B: Granulation tissue growth in the region of a chalazion. The tissue has responded by forming multiple fine-caliber vascular channels associated with an infiltrate of acute and chronic inflammatory cells. The lightly stained areas in the tissue represent the response of fibroblasts and vascular endothelial cells to alter and augment the extracellular matrix. (Hematoxylin-eosin stain, ×100.) |
Wound healing of highly specialized tissues of the eye has several unique features when compared with the benchmark processes in skin.
Corneal Healing
The healing of the cornea is unique relative to other soft tissues because the tissue lacks blood vessels and because it is lined on its anterior and posterior surfaces by layers of epithelial-like cells. Epithelial cells of the cornea can produce essential wound-healing factors normally produced by platelets.15 Architectural repair is accomplished at the level of the corneal stroma.
Abrasions are injuries generally involving only the superficial layer (epithelium) of the cornea (Fig. 6.2). Abrasions are commonly caused by mechanical injuries or anoxia resulting from contact lens overwear. Some or all of the layers of the surface epithelium are lost, but Bowman membrane remains intact. Spontaneous and recurrent corneal epithelial erosions are common with minimal trauma in conditions that produce faulty integrity of the epithelial basement membrane. Autosomal dominant anterior basement membrane dystrophy is the most common of these conditions, which also include the corneal stromal dystrophies (e.g., lattice dystrophy) and calcific band keratopathy. After a delay of approximately 1 hour, uninjured epithelial cells at the margin of the wound loosen their intercellular and basal attachments and migrate “en masse” toward the injured area.16 The shape of the wound margin and the biochemical characteristics of the exposed tissue influence the direction and extent of the migration.17 If the entire corneal epithelium is abraded, migrating epithelial cells derived from the limbal stem cells are able to cover the defect completely within 48 to 72 hours. The epithelium will be much thinner than normal until mitotic division reestablishes normal thickness. Re-formation of epithelial basement membrane may not be detectable for as long as 6 weeks after injury.18 Clinically, the healed wound is transparent.
Small defects of Bowman membrane (Fig. 6.3) do not heal by fibrous proliferation of the stroma. The defect is filled by proliferating epithelial cells (epithelial facet formation) that reestablish the surface continuity of the cornea. The facet may be seen clinically as a focal, well-demarcated, superficial corneal opacity. Most often, this type of defect is caused by a corneal foreign body.
Penetrating corneal injuries involving at least onethird of the stroma (Fig. 6.4) are covered initially by proliferating surface epithelium that may extend for a considerable distance into the stroma. The extent of corneal epithelial migration is controlled at least in part by contact inhibition of migration once contact with healthy corneal endothelial cells is established.19 Bowman membrane has elastic properties that tend to pull the anterior margins of the wound apart. Exposure of the normally dehydrated corneal stroma to tears and blood will cause swelling of the corneal stroma. This swelling of the stroma tends to close the wound. As the stroma heals, new collagen is produced by keratocytes or transformed monocytes. The repair collagen is different from the native collagen in size and in orientation. Epithelial cells will regress toward the surface, except in rare cases such as epithelial ingrowth, where corneal epithelium may proliferate and migrate along the posterior corneal surface to cover the iris and anterior chamber angle. This may occur following penetrating trauma or surgical corneal penetration. This phenomenon of ingrowth can lead to corneal haze and secondary open-angle glaucoma. Epithelial ingrowth into the lamellar intrastromal space created by formation of LASIK flaps or anterior lamellar keratoplasty flaps may also represent a vision-compromising surgical complication. The typical partial-thickness healed wound is densely opaque and obvious clinically, but it may be detected histologically only by the break in Bowman membrane.
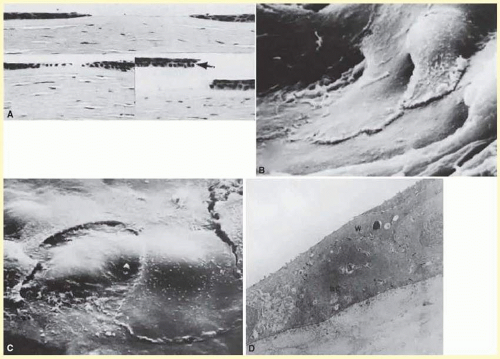 FIG. 6.2 Corneal epithelial cell repair of an abrasion. A: Early in the repair process, epithelial cell layer attenuation is present at the edges of the abrasion (top). The epithelial wound heals by epithelial migration over Bowman membrane (lower left). Artifactual epithelial breaks have right-angle contours (lower right, arrow). (Hematoxylin-eosin stain, ×136.) B: Scanning electron micrograph (SEM) of the leading edge of the corneal epithelium 1 hour after mechanical abrasion. C: SEM of the leading edge of the migrating epithelium. Superficial cells not directly involved in migration may be desquamated. D: Transmission electron micrograph of the leading edge of migrating corneal epithelium 2 hours after mechanical abrasion. Desmosomes are continuous with the wing (W) cell layer overlying a rounded basal cell (BC). Note the loss of hemidesmosomes and the many lateral desmosomes (arrows) between the adjacent basal cells. There are few apical desmosomes between the basal cell on the right and the adjacent wing cell. (B-D: rabbit, ×4000.) |
Full-thickness wounds of the cornea are associated with retraction of Descemet membrane and separation of the posterior aspect of the wound (Fig. 6.5). Secondary aqueous, a proteinaceous coagulum, may seal the wound posteriorly until healthy surrounding endothelial cells can spread and migrate into the injured area. Mitotic division of the endothelial cells possibly plays an important role in younger patients, but probably is not clinically significant in adults. Ultimately, migrated endothelial cells will produce a new Descemet membrane.20,21,22,23 The portions of Descemet membrane displaced into the stroma are not resorbed, but remain as the histologic marker of the site of injury.
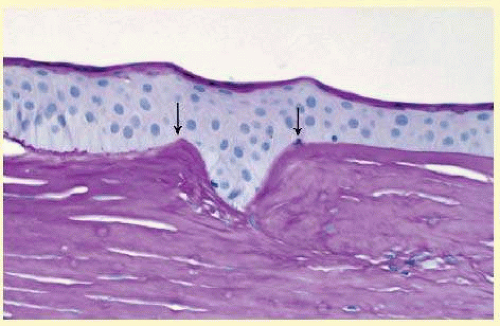 FIG. 6.3 Epithelial facet. The superficial defect between the cut edges of Bowman membrane (arrows) is filled with epithelial cells in such a manner as to reestablish the original surface contour of the cornea. Bowman membrane will not regenerate in this area. Because of the limited extent of the injury, the underlying collagenous tissue does not participate in the wound-healing process. (Periodic acid/Schiff stain, ×200.) |
Conjunctival Healing
Conjunctival healing differs from corneal healing due to the presence of blood vessels and a lymphatic system. The conjunctival epithelium heals by migration and mitosis.24 Conjunctival stem cells are thought to originate at the mucocutaneous junction and migrate to the fornix.25 Goblet cells are produced by epithelial progenitors and appear once conjunctival epithelial cell continuity has been reestablished.26 The presence of vascular tissue in the substantial propria of the conjunctiva allows for the formation of granulation tissue and scar tissue, as found in soft tissues elsewhere.
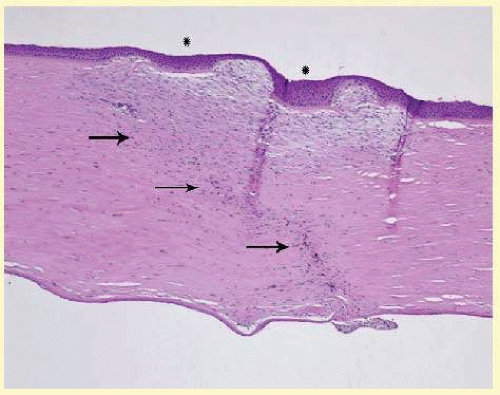 FIG. 6.4 Deep stromal defect (arrows). In the area of the defect (asterisks), the epithelium is hyperplastic (thickened), Bowman membrane is absent, and the corneal stroma is hypercellular. A stromal scar is characterized by an increased number and haphazard arrangement of keratocytes and extracellular matrix. (Hematoxylin-eosin stain, ×100.) |
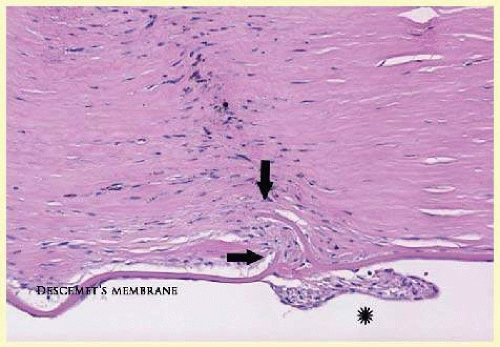 FIG. 6.5 Descemet membrane has elastic properties that cause inward curling when incised (arrows). The fibrous reaction between cut ends of Descemet membrane indicate a wound of long standing. A retrocorneal membrane (asterisk) has formed on the posterior surface of Descemet membrane through the process of fibrous metaplasia of the corneal endothelium. (Hematoxylin-eosin stain, ×200.) |
Scleral Healing
The sclera itself does not participate directly in tissue repair. Partial-thickness injuries are healed by formation of granulation tissue from the episcleral tissue in external wounds or from uveal tissue in internal wounds. Full-thickness defects of the sclera heal by granulation tissue originating in the episcleral tissue and uveal tract. Mitomycin is used in filtering procedures specifically to prevent the formation of granulation tissue and to promote establishment of an aqueous fistula.27
Surgical Limbus Healing
With current cataract phacoemulsification techniques, the corneal wound is typically placed in the peripheral clear cornea as opposed to the anatomic limbus to reduce induced astigmatism and to shorten the natural history of cataract wound healing.28 The healing of the wound is similar to that found in central corneal incisions.
Healing at the site of a limbal surgical incision, typically used in glaucoma filtration procedures, involves a combination of the features of repair of the cornea, conjunctiva, and sclera. Conjunctival epithelium will heal over an area of granulation tissue originating from the substantia propria of the conjunctiva and the episclera. The granulation tissue seals the wound if the wound edges are well apposed. The remainder of the healing process is similar to the healing of an external scleral wound. Granulation tissue is not formed in the internal portion of the wound because the uveal tract is not involved. The internal wound is healed by endothelial migration and re-formation of Descemet membrane in a manner outlined above for full-thickness corneal wounds.29,30
Because of the lack of blood vessels, the rate of wound healing is slow relative to that of the skin. Whereas an injury to the skin may have regained its tensile strength in 7 to 10 days, injuries to the surgical limbus may require as long as 12 months to regain a stable tensile strength. The tissues of the wound remain structurally weaker than the surrounding uninjured tissue. The healing of a clear corneal cataract incision proceeds as described above.
Uveal Healing
Wound healing of the posterior uveal tract follows the general principles for healing of vascularized tissue. The iris, however, heals differently. When the iris wound is perpendicular to its circumferential ridges, such as in a typical peripheral iridectomy or iridotomy, the cut edges pull apart. Granulation tissue does not form to close iridectomy incisions probably because of the inhibitory effect of the aqueous flowing through the opening of these small incisions. Iridotomies created by argon laser (Fig. 6.6) may be anatomically closed by apparent migration of iris pigment epithelium.31
Lens Healing
Proliferation and fibrous metaplasia of the lens capsular epithelium occurs with interruption of the lens capsule either associated with trauma or surgery (Fig. 6.7). After maturation of the fibrous tissue, the most superficial epithelial cells will form a new lens capsule. Most wounds to the lens, small and large, result in cataracts. Small wounds, however, may result in tiny focal opacities.32,33 Lens epithelial cells undergo fibromyoblastic transformation when stimulated by injury. The transformed cells are able to produce type I and type III collagen and glycosaminoglycan.34 This is the fundamental process resulting in opacification of the posterior lens capsule after extracapsular cataract extraction or phacoemulsification. Apoptosis (programmed cell death) also plays a role in the formation of secondary cataracts.35
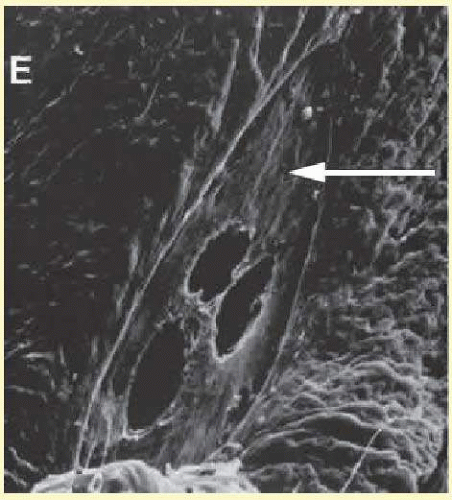 FIG. 6.6 Scanning electron micrograph of the posterior surface of the iris in a case of angle-closure glaucoma treated with argon laser iridotomy. Centrally, there are three areas of penetration of iris tissue. Iris pigment epithelium has been lost for a considerable distance from the actual opening (arrow). Normal iris pigment epithelium is present peripherally. |
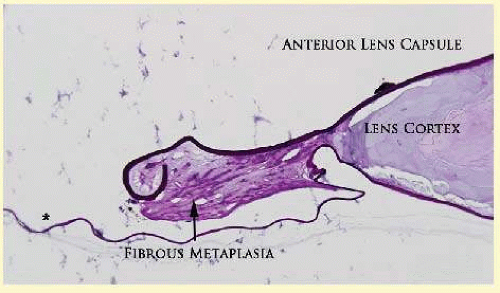 FIG. 6.7 Light micrograph at the site of anterior capsulectomy. The anterior and posterior segments of lens capsule have sealed, sequestering remaining lens cortex. The remaining viable lens epithelial cells have undergone fibrous metaplasia to create an adhesive fibrous scar (arrow). The posterior capsule (asterisk) in the visual axis remains transparent because the fibrous process has not extended across the posterior capsular surface to involve the visual axis. (Periodic acid/Schiff, ×100.) |
Retinal Healing
Healing of the neurosensory retina follows the principles of generalized wound repair. There is an initial removal of all necrotic tissue by phagocytosis, followed by proliferation of cells to form a chorioretinal bond. The healing, however, is modified in most instances by the lack of participation by the blood vessels.36,37,38 Astrocytes from the neurosensory retina proliferate from the peripheral viable tissue into the wound and downward into the area of the subretinal space (Fig. 6.8). Retinal pigment epithelial cells from the peripheral viable tissue undergo fibrous metaplasia and proliferate upward into the area of the subretinal space and wound. When the two proliferating cell types unite, a tight chorioretinal bond is formed. Increased retinal adhesiveness has been estimated to be 140% of the normal degree of adhesiveness 2 weeks after photocoagulation.39 Retinal holes may heal spontaneously if supported by an intact vitreous base or if located adjacent to the retinal pigment epithelium (Fig. 6.9).40 For the retinal pigment epithelium to differentiate, it must be in contact with Bruch membrane.41 Choriocapillaris repair from a photocoagulation wound of the retina appears to proceed in a manner similar to that of repair of capillary thrombosis in other tissues. The vascular repair process may not reproduce the lobular architecture of the native choriocapillaris. The choriocapillaris may regenerate in areas of restored retinal pigment epithelium. Proliferative vitreoretinopathy is an expression of abnormal retinal wound healing.42
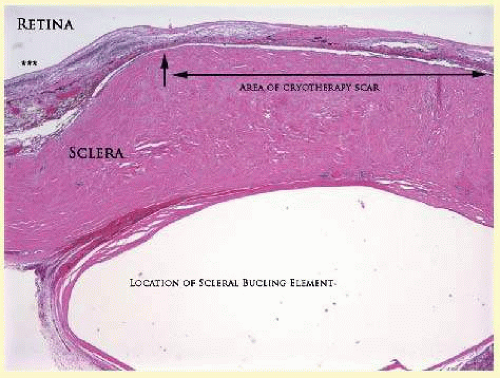 FIG. 6.8 Light micrograph of an area over a retinal buckling element for retinal reattachment. Cryotherapy has been applied in the area (double-headed arrow), causing atrophy of the neurosensory elements of the retina. There is an intimate association of the remaining glial elements of the retina with proliferated retinal pigment epithelial cells in the plane of the former subretinal space. A portion of the retina (triple asterisks) not affected by cryotherapy is posterior to the buckling element. The adhesion prevents intraretinal separation in this area. (Periodic acid-Schiff stain, ×100.) |
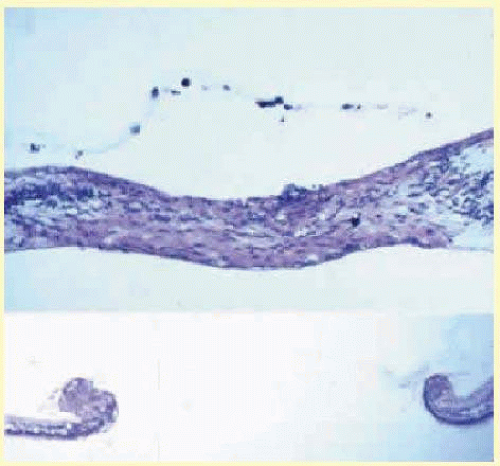 FIG. 6.9 Retinal healing by proliferation of glial cells. In the presence of an intact vitreoretinal interface acting as scaffolding, retinal glial cells are able to proliferate and seal small retinal holes. The arrow indicates artifactually detached vitreoretinal interface. |
Interruption of Bruch membrane may allow the ingrowth of fibrovascular tissue from the choroid into the subretinal space, resulting in a modified granulation wound-healing process and subretinal scarring.43
HISTOLOGY OF OCULAR SURGICAL PROCEDURES
Cataract Extraction
The cataract incision is made into the anterior chamber in such a way as not to injure the trabecular meshwork or unduly injure the cornea. The more traditional scleral tunnel wound extends from the episcleral tissue posterior to the surgical limbus (defined by the insertion of the conjunctiva and Tenon capsule) through the corneoscleral tissue to enter the anterior chamber by perforating Descemet membrane anterior to Schwalbe line. The more modern and more commonly performed biplanar or triplanar clear corneal cataract incision involves only the peripheral cornea. Special circumstances may occur in which a more posterior or anterior route of incision may be desirable, for example, in eyes that have previously undergone penetrating or lamellar keratoplasty or those with suspicion for iris hypermobility (“floppy iris”).44,45
A clear corneal cataract incision is barely visible either histologically (Fig. 6.10) or clinically. The wound extends from a small hiatus of Bowman membrane obliquely through the corneal stroma to exit well anterior to the anterior chamber angle structures. Repair occurs only in the region of Bowman membrane and Descemet membrane. The stromal portion of the wound remains relatively weak indefinitely. Occasionally, a fibrous plaque is present at the level of Descemet membrane. This plaque is another example of fibrous metaplasia, in this instance of the corneal endothelial cells.
The capsulotomy incision is anterior to the insertion of the zonules through a relatively thick area of the anterior capsule. The traditional can-opener style capsulotomy has been largely replaced by a continuous circular capsulorrhexis technique, which results in a stable circular anterior capsular edge rather than free flaps. Most of the lens epithelial cells are removed with the anterior capsule, although some cells may remain in the region of the equator of the lens. The residual lens capsule is thinnest at its posterior pole. The remaining anterior capsular tissue often adheres to the posterior capsule, encasing any residual cortical material and lens epithelial cells. Lens epithelial cells may grow to form large cells, called bladder cells, or may undergo fibrous metaplasia to form a collagenous plaque. Lens cortex may remain inside the lens capsule, particularly at the equator where a negative image of an intraocular lens loop may be identified histologically (Fig. 6.11). In complicated cases of lens extraction, the crystalline lens remnants and a negative image of the intraocular lens may be encased in reactive fibrous tissue affecting both the anterior and posterior chambers (Fig. 6.12).
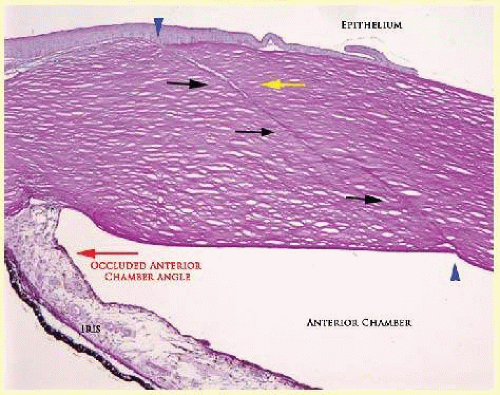 FIG. 6.10 The clear cornea cataract incision extends from Bowman membrane (blue arrowhead), obliquely through the corneal stroma (black arrows), and exits well anterior to the trabecular meshwork structures through Descemet membrane (blue arrowhead). Healing occurs at the extremes of the wound (blue arrows), but not along the course of the stromal wound. Separation of the wound in this case is evident in its anterior portion (yellow arrow). In this case, the eye was enucleated because of iris neovascularization and anterior angle closure. The disturbance of the epithelium (bullae formation and intraepithelial basement membrane) is due to corneal decompensation. (Periodic acid/Schiff, ×20.) |
Peripheral iridectomies, which are rarely performed in modern routine cataract phacoemulsification except in cases of severe uveitis or placement of an anterior chamber intraocular lens, are peripheral to the iris sphincter in the midportion of the iris rather than at the less accessible iris base. Complete or sector iridectomies include the iris sphincter but do not extend to the iris base. The edges of an iridectomy may show some rounding of contours, but granulation tissue does not form and iris pigment epithelial proliferation does not generally occur. The iris pigment epithelium may be absent for a considerable distance from an iridectomy produced by laser energy.
Intraocular lens material (acrylic, silicone, or polymethylmethacrylate) often dissolves during tissue processing. Outdated intraocular lenses containing metal components must be removed before embedding because metal will cause extensive artifacts and damage to microtome knives. Often the only clues to the presence of an intraocular lens are subtle compression changes of the iris or ciliary sulcus. Occasionally, residual synthetic material can be identified by polarized light. Anterior chamber lenses may cause a fibrous reaction in the anterior chamber angle (Fig. 6.13).
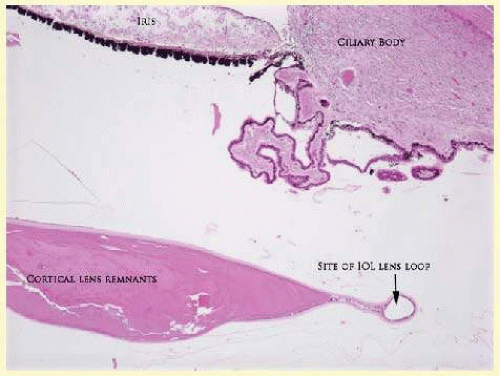 FIG. 6.11 Light micrograph of retention of an excessive amount of lens cortex in a case of cataract extraction. The intraocular lens has been placed within the lens capsule. The negative image of the lens loop within the lens capsule is present at the peripheral equator of the lens remnants. The image of the lens optic is not at this plane of section. (Hematoxylin-eosin, ×20.) |
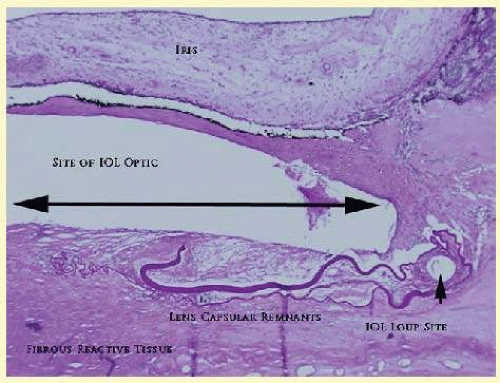 FIG. 6.12 The anterior chamber from a case of complicated cataract extraction. The IOL optic and loop can be identified in surrounding fibrous reactive tissue. The polymer of the lens has been dissolved by organic solvents during tissue preparation. The fibrous reaction has formed a cyclitic membrane posterior to crystalline lens remnants. (Periodic acid/Schiff, ×200.) |
Occasionally, collagenous tissue will completely encircle a lens. Iris-supported lenses are associated with the loss of central iris pigment epithelium or residual nylon suture in the posterior chamber. Posterior chamber lenses are the most difficult to identify unless surrounded by lens remnants, in which case a negative image of the optic or loops can be seen. Sulcus-fixed lenses will show focal areas of iris pigment epithelial depigmentation or iris stromal erosion. The lens loop may displace the peripheral iris to come in contact with the trabecular meshwork.
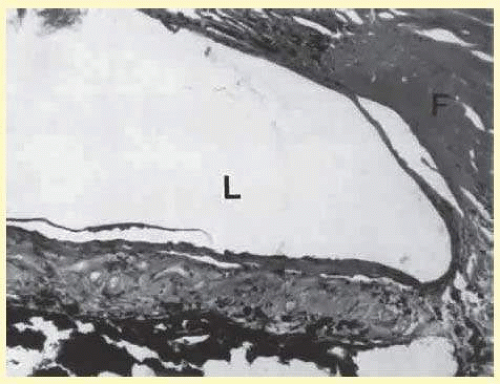 FIG. 6.13 Light micrograph of fibrous reaction to the presence of an anterior chamber-type intraocular lens (L). The fibrous tissue (F) has completely occluded the filtration tissue of the anterior chamber angle, causing secondary open-angle glaucoma. (Periodic acid-Schiff stain, ×40.) |
Penetrating Keratoplasty
Penetrating keratoplasty involves replacement of diseased full-thickness host tissue with normal full-thickness donor tissue. The concave-convex host specimen usually is 7.0 to 8.5 mm in diameter and translucent because of fixation. The cone, which may be eccentric in the specimen, needs to be identified during gross examination to be included in the histological section. During examination, Gross orientation of the specimen is important if pertinent changes are to be represented in the histologic section.
Penetrating keratoplasty wounds in enucleation specimens can be identified by the changes in Descemet membrane (Fig. 6.14). If donor tissue is from a younger person than the host, Descemet membrane of the graft may be thinner than the peripheral membrane of the host. Occasionally, redundant Descemet membrane from the host intentionally will be left behind in this region by the surgeon (Fig. 6.15). Often small areas of retrocorneal fibrous plaque mark the posterior area of the wound, even in cases of clinically uncomplicated wound healing. In time, the stromal portion of the wound may be undetectable histologically although some malorientation of the collagen lamellae often is present. Bowman membrane does not re-form as a distinct membrane-like structure. Needle tracks or suture material may be seen in the tissue adjacent to the wound. Occasionally, epithelial cells may extend for a considerable distance along these suture tracks.
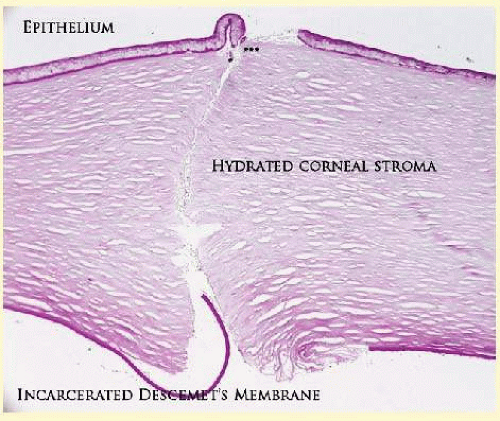 FIG. 6.14 Light micrograph of a healed penetrating keratoplasty incision. Collagenous reactive tissue is just beginning to form in the anterior wound (triple asterisks). The corneal stroma exposed to tears and aqueous has become hydrated and self-sealed. Descemet membrane has become incarcerated into the posterior wound, which will limit the ability of the posterior wound to repair. (Periodic acid-Schiff stain, ×200.) |
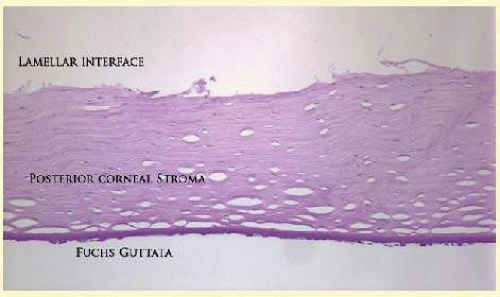 FIG. 6.15 Light micrograph of a specimen removed from a posterior lamellar graft procedure. In this procedure, only the posterior corneal tissue including abnormal endothelium characterized by the formation of Fuchs guttata was removed and replace with healthy posterior donor tissue. (Periodic acid/Schiff stain, ×100.) |
Lamellar Keratoplasty
Lamellar keratoplasty procedures are classified and named according to anatomic location. Anterior lamellar keratoplasty (ALK) involves removal of a lenticule of anterior corneal stroma, Bowman membrane, and epithelium, typically 50 to 300 µm in thickness, and replacement with a similarly sized donor lenticule of anterior corneal tissue. The donor and recipient tissue may be cut with either microkeratome or femtosecond laser, and sutures may or may not be present.46 In deep anterior lamellar keratoplasty (DALK), the recipient’s corneal stroma and epithelium are removed while Descemet membrane is conserved. The donor lenticule consisting of full-thickness corneal stroma and epithelium is sutured into place. There may be duplication of Descemet membrane at the base of the specimen, if Descemet membrane is not stripped from the donor lenticule prior to implantation. Deep lamellar endothelial keratoplasty (DLEK) involves removal of the posterior corneal stroma and Descemet membrane, with implantation of a donor posterior corneal lenticule (Fig. 6.16). A step-off may be present peripherally, and fibrosis may be noted in the interface between donor and recipient stroma. Descemet stripping endothelial keratoplasty (DSEK) has largely replaced DLEK, and involves removal of recipient Descemet membrane with subsequent implantation of a thinner (70 to 200 µm) donor lenticule of deep corneal stroma, Descemet membrane, and endothelium (Fig. 6.17). Histologically, there may be duplication of Descemet membrane noted peripherally where the graft overlaps the area of Descemet stripping, and there is less fibrosis at the donor/recipient stroma-stroma interface as compared with DLEK.
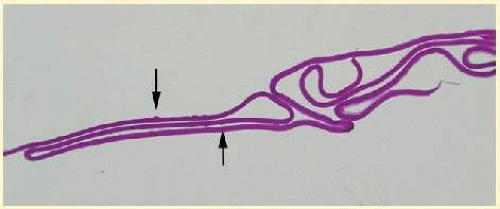 FIG. 6.16 Lightmicrograph of tissue removed from a Descemet membrane stripping procedure. Occasional Fuchs guttata can be identified (arrows). (Periodic acid/Schiff, ×200.) |
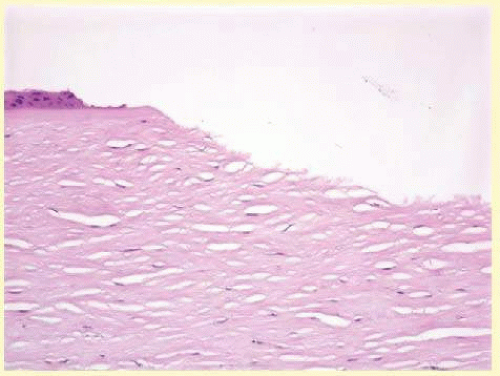 FIG. 6.17 Light micrograph of the wound profile of a LASIK flap prepared with a microtome. There is some disruption of the adjacent epithelium. Bowman membrane wound profile and exposed stromal wound profile is oblique. The stromal profile is slightly irregular. (Hematoxylin-eosin, ×100.) |
Refractive Surgical Procedures
Laser in situ keratomileusis (LASIK) has become the predominant surgical procedure for the correction of refractive error, particularly myopia.47 An estimated 12 to 14 million procedures have been performed overall in the United States.48 Approximately 800,000 procedures were performed in 2007.49 The advantages over previous laser procedures, particularly photorefractive keratectomy, include less postoperative pain, faster return of visual function, less regression of refractive effect, and less central corneal haze.
The LASIK procedure provides access to the central corneal stroma by employing a mechanical oscillating steel microtome (Fig. 6.18) or a femtosecond laser (Fig. 6.19) to create a lamellar flap. The microtome or laser coupling device is stabilized to the anterior globe by a suction device that can raise the intraocular pressure to levels between 80 and 360 mm Hg, depending on the type of microtome used.50 The hinge of the flap may be placed horizontally or vertically. An excimer laser removes a calculated amount of corneal stroma according to an algorithm determined for the type and amount of refractive error. The central corneal epithelium is not disturbed. The anterior corneal flap is repositioned without sutures.
Central corneal thickness has become a critical factor in determining the amount of tissue that can be safely removed to protect corneal endothelial cells. In most cases, the safety zone for the posterior corneal stroma has been established at 250 µm.51,52 This zone is necessary to reduce the risk of endothelial cell damage and the risk of postoperative iatrogenic corneal ectasia. Several studies have shown a marked variation of normal central corneal thickness in a range of 472 to 651 m.53,54 The central corneal thickness is independent of axial length, age, sex, horizontal corneal diameter, and refractive error.53 Preoperative pachymetry is therefore mandatory.
 FIG. 6.18 Scanning electron microscopy of the lamellar bed in LASIK. A: At the edge of the wound, oscillation marks caused by some types of microkeratomes can be identified. The lamellar bed in the center of the wound is moderately irregular. |
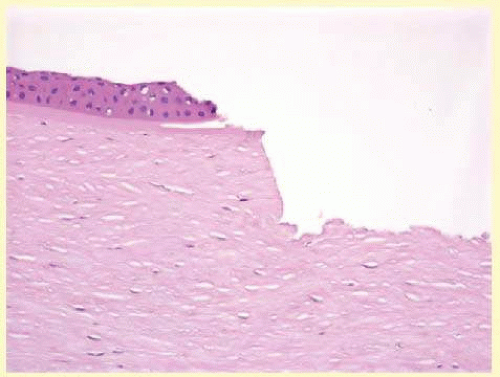 FIG. 6.19 Light micrograph of the wound profile of a LASIK flap repaired with a femtosecond laser. There is less disruption of the adjacent epithelium. Bowman membrane wound profile and exposed stromal wound profile is nearly at right angles to the surface contour. The stromal profile is slightly irregular. (Hematoxylin-eosin, ×100.) |
With several microkeratomes, scanning electron microscopy may show a fine undulating contour up to 0.2 mm at the border of the lamellar bed and flap. This feature is a consequence of “chatter” caused by the microkeratome’s reciprocal action. The frequency of the “chatter” may relate to the nonlinear pass of the microkeratome. Chatter is absent in rotary keratomes and keratomes using a high oscillatory frequency.55 The femtosecond laser, on the other hand, creates a smoother and more predictable incision which is more regular on both histology and electron microscopy.46
The refractive outcome of all refractive procedures depends on the wound-healing response of the corneal epithelium and stroma. The wound-healing response in LASIK is found primarily at the region of epithelial transection at the edge of the flap. In animal models, epithelial reaction and production of type IV collagen is seen at the most peripheral edge of the lamellar flap. Gelatinase B, which is important in basement membrane remodeling, was localized to the basement membrane zone and superficial stroma.56
There is minimal to no inflammatory infiltrate along the margins of the lamellar bed. However, disorganization of the extracellular matrix extending to a depth of 5 µm from the surgical margin has been observed for as long as 9 months after surgery. The disorganization of the extracellular matrix suggests that the wound-healing process is incomplete for a long period after surgery.57 Keratocytes in the region of the edge of the flap can be strongly stimulated by epithelial cell cytokines in part because of the localized absence of Bowman membrane. The potential for anterior stromal haze in the setting of LASIK is limited to the flap border, whereas in photorefractive keratectomy, the haze is most likely to occur centrally.58 In LASIK, there is a combination of intact corneal epithelium not producing cytokines and an intact Bowman membrane limiting the diffusion of cytokines to influence underlying keratocytes.59 With LASIK, however, there appears to be increased interface reflectivity associated with thin lamellar flaps. There also appears to be a loss of keratocytes in the most anterior flap stroma in the period between 6 months and 2 years after surgery.60
With respect to the observed loss of corneal sensation following refractive surgical procedures, the ophthalmic and maxillary branches of the trigeminal nerve supply the cornea. Most of the corneal stromal nerve supply is within the anterior two-thirds of the stroma. Corneal sensation is essential for the maintenance of normal corneal physiology. The LASIK procedure transects nearly all corneal nerves except those located in the hinge of the flap. Corneal sensitivity is reduced 1 to 2 weeks after the LASIK procedure, with the highest sensitivity remaining greatest at the hinge. Sensation has been noted to return during the next 6 months.61
Return of tensile strength to the lamellar incision of the corneal stroma is limited after LASIK. In an animal model, Maurice estimated that the wound-healing process reestablished only 50% of the native tensile strength of the stroma.62 This lack of intrastromal adhesion is expressed in a rate of flap dislodgement estimated to be between 1% and 2% of all LASIK procedures.63
Glaucoma Surgical Procedures
Laser trabeculoplasty causes distortion, shrinkage, and scarring of the collagenous beams of the trabecular meshwork. No perforation occurs into the area of Schlemm canal.
Cyclocryotherapy, cyclodiathermy, and therapeutic ultrasonography apply energy directly to the pars plicata and cause lysis of the ciliary muscle and occlusion of the vascular supply, leading to extensive necrosis and scarring. Pressure lowering is accomplished by a reduction of aqueous production. Heat applied to the sclera may cause necrosis and localized scleral thinning. Cold applied to the sclera, unless extreme, does not cause any clinical or histologic changes.
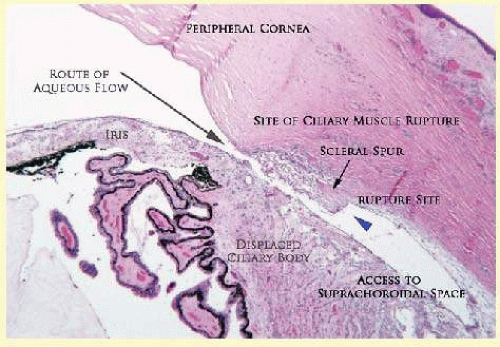 FIG. 6.20 Light micrograph of cyclodialysis. The longitudinal muscle of the ciliary body has been ruptured from its attachment to the scleral spur (blue arrowhead). Aqueous from the anterior chamber has free access to the suprachoroidal space resulting in ocular hypoteny. The displaced ciliary body may spontaneously reappose to the region of the scleral spur causing a sudden increase in intraocular pressure. (Hematoxylin-eosin, ×20.) The long arrow indicates the route of aqueous flow. The short arrow indicates the position of the scleral spur. |
Cyclodialysis (Fig. 6.20) creates a cleft between the sclera and the longitudinal muscle of the ciliary body. Aqueous passes directly from the anterior chamber into the suprachoroidal space. Histologically, the longitudinal muscle of the ciliary body is disinserted from the scleral spur. Diaphanous tissue often is present in the suprachoroidal space along the route of filtration. The presence of this tissue differentiates the surgical site from artifactual disinsertion of the ciliary body, which is a common artifact of ocular tissue preparation.
Many surgical variations are or have been used to create a fistulous tract between the anterior chamber and the episcleral tissue to allow continuous passage of aqueous from the eye. In most cases, the incision is placed at the surgical limbus or more posteriorly in the sclera. The primary variations center on ways to prevent the fistula from closing. Some older procedures simply used a large (2-mm) trephine hole, which was less likely to close than a smaller opening. Cautery placed at the exposed edges of the sclera caused retraction of the wound edge to maintain the fistula. In trabeculectomy, a half-thickness window of posterior peripheral cornea is excised to create a large internal orifice for a fistulous track under a protective scleral flap. Iridencleisis intentionally includes incarceration of iris into the wound to prevent complete scleral healing. Multiple types of foreign material, from horsehair to gold to silicone, in solid or tubular forms, have been fashioned into setons to maintain the opening to the anterior chamber. Current iterations of these types of setons include Baerveldt and Ahmed tube shunts. Some varieties of these setons route aqueous to the equator of the eye, where it can then be resorbed by the surrounding tissue.
Most recently, various agents have been used to control the rate and extent of fibrous proliferation in a surgical fistula. Currently, the most common agent is mitomycin-C, although 5-fluorouracil has been used in the past. The exact mechanism of action is not known, but limitation of proliferation and migration of cells involved in the wound-healing process appears to play a substantial role.64
Trabeculectomy specimens usually consist of a tiny portion of pigmented and translucent tissue. Occasionally, clinically unsuspected epithelial ingrowth can be identified in this type of specimen (Fig. 6.21).
Retinal Reattachment
Retinal reattachment surgery employs one of several strategies: vitrectomy with or without injection of fluorocarbon gas or silicone, sclera buckling, laser photocoagulation, or cryotherapy.
Histologic signs of vitrectomy are usually limited to the site of port placement by a discontinuity of the ciliary pigment epithelium and possible fibrous reaction at the vitreous base. Fluorocarbon gas generally does not alter the architecture of the eye. Silicone, however, may create vacuoles both in reactive tissue and in normal structures of the eye such as the retina (Fig. 6.22) and the optic nerve.65 It is possible for silicone oil to migrate from the vitreous cavity to the brain.66
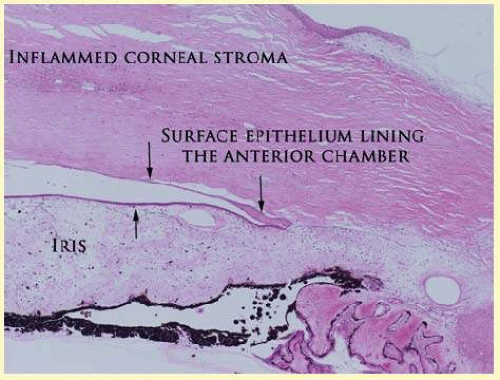 FIG. 6.21 Light micrograph of the peripheral anterior chamber in a pseudophakic eye. Squamous epithelium has gained access to and lined the surfaces of the anterior chamber angle (arrows). In this case, there is angle closure; however, when the squamous epithelium lines trabecular meshwork, the filtration apparatus becomes scarred and nonfunctional. (Periodic acid/Schiff, ×20.) |
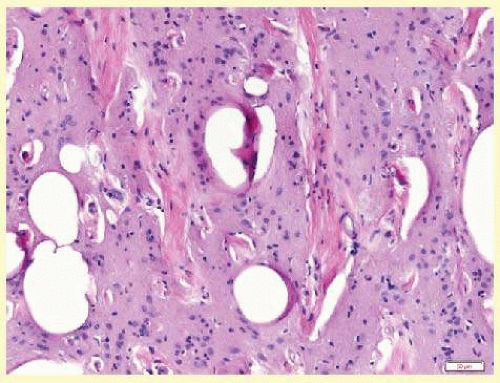 FIG. 6.22 Light micrograph of an area of retinal gliosis contains trapped globules of silicone. The silicone itself has been lost during tissue processing. Silicone may cause a granulomatous foreign body reaction. (Hematoxylin-eosin, ×100.) |
Evidence of a previous scleral buckling procedure is often synthetic bands and other surgical devices on the surface of an enucleated globe. Occasionally, the episcleral fibrous tissue reaction completely encases these materials in a fibrous cloak. This type of device, as with any type of synthetic device, may migrate after implantation, causing functional abnormalities such as strabismus and a subconjunctival mass. In this circumstance, the device must be repositioned or removed.67
Synthetic bands are partially soluble in organic solvents used in tissue dehydration for paraffin embedding. The negative image of the material can be seen, usually in the equatorial region, surrounded by a variable degree of fibrous tissue and focal collections of chronic nongranulomatous inflammatory cells (see Fig. 6.8). Occasionally, a foreign body granulomatous reaction is present near degenerating suture. Often, the uveal tract in the area of surgery is completely atrophic, as is the overlying retina.
Either photocoagulation or cryotherapy will cause depigmentation of the retinal pigment epithelium centrally and fibrous metaplasia of the surviving retinal pigment epithelial cells peripherally.68,69
Laser photocoagulation of the retina at therapeutic energy levels results in a chorioretinal adhesion between proliferating Müller cells and retinal pigment epithelial cells or between the glial component and the denuded inner surface of Bruch membrane. The internal limiting membrane of the retina, the basement membrane of the retinal blood vessels, and Bruch membrane remain intact. Numerous focal areas of choriocapillaris defects remain in the area of photocoagulation.
COMPLICATIONS OF SURGICAL TRAUMA
All ocular surgical procedures are associated with potential complications. A complication is a deviation from the natural course of the expected tissue response after a surgical procedure and, in the case of ocular surgery, usually results in a compromise of ocular function. Complications may arise from the surgical procedure itself or be the result of an aberration of the wound-healing process. All surgeons will encounter surgical complications. Eyes afflicted with severe or multiple disease processes are more likely to develop complications. Early recognition and a thorough understanding of these deviations from normal allow for more effective therapeutic intervention.70
Cataract Extraction
Intraoperative Complications
Complications occurring from the time the patient enters the operating room until the patient leaves the operating room are considered intraoperative.71
Descemet membrane is only loosely adherent to the posterior stroma and may be stripped into the anterior chamber at the time of the corneal incision placement (Fig. 6.23) or injection of viscoelastic material. Splitting off of Descemet membrane from the posterior cornea can lead to postoperative intractable corneal edema.
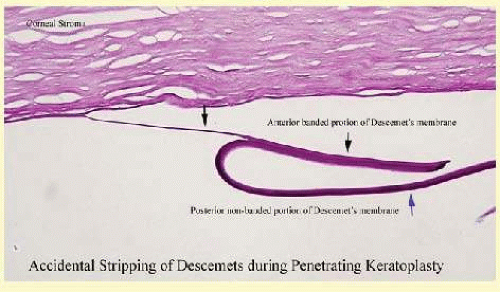 FIG. 6.23 Light micrograph of a portion of Descemet membrane inadvertently dislocated during a penetrating keratoplasty procedure. The area of separation is between the anterior banded portion of Descemet membrane (black arrows) and the later developing posterior Descemet membrane (blue arrow). (Periodic acid/Schiff, ×100.) |
Intraoperative anterior chamber hemorrhage may result from an inadvertent iridodialysis or from an iridectomy wound. The site of hemorrhage is usually found along the scleral side of the cut edge of the wound. This type of hemorrhage rarely leads to serious clinical problems.72
Rupture of the posterior lens capsule increases the risk of vitreous loss and limits options for the implantation of an intraocular lens. Vitreous loss leads to an increased incidence of iris prolapse, bullous keratopathy, epithelial downgrowth, stromal overgrowth, wound infection and endophthalmitis, updrawn or misshapen pupil, vitreous bands, postoperative flat anterior chamber, secondary glaucoma, retinal detachment, cystoid macular edema, optic disc edema, vitreous opacities, vitreous hemorrhage, and other sight-threatening consequences.73,74
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


