Surgical Anatomy of the Head and Neck
Michael D. Maves
Anatomy is the basic science of all surgery. Surgery in the region of the head and neck cannot be considered safe unless the surgeon thoroughly understands the anatomy of this area and its important variations. Although anatomic structures and the relations between them do not change, our knowledge of anatomy must be continually updated to meet the challenge of new surgical techniques and approaches. This chapter is an overview of the surgical anatomy of the head and neck with a focus on the major regions. It is not a substitute for thorough anatomic knowledge, which can be gained only through intensive study in a cadaver laboratory and an operating room.
THE CRANIUM
Scalp
The cranium is covered by the hair-bearing scalp, which is divided into layers of skin and subcutaneous tissue, galea aponeurotica, loose connective tissue, and periosteum or pericranium covering the calvarial vault. The blood supply of the scalp comes from the paired supraorbital and supratrochlear arteries anteriorly, the terminal branches of the superficial temporal arteries laterally, and the occipital vessels posteriorly. This rich vascularity provides a network on which small scalp flaps can be based and rotated, as in the management of male pattern baldness. Sensation to the scalp is provided by branches of cranial and spinal nerves.
Calvaria
The bony vault of the cranium, the calvaria, consists of the unpaired frontal bone, the paired parietal bones, and the unpaired occipital bone (Fig. 1.1). In the lateral aspect, the greater wing of the sphenoid bone and the temporal bone complete the cranium. There is a rich layer of diploic bone between the inner and outer tables of the calvaria. This is a source for split-thickness calvarial bone grafts, which often are used in head and neck reconstruction. The calvarium is thickest at the external occipital protuberance and in the parietal region. It is thinnest over the temporal region. This allows ready access for neurotologic operations on the middle fossa. The venous circulation of the calvaria is provided by diploic veins, which drain to the veins of the scalp or into the dural venous sinuses. In some instances, the diploic veins are connected to each other, and this communication allows osteomyelitis that originates in the frontal sinus to involve the frontal bone, scalp, and dura.
CRANIAL FOSSAE
The intracranial cavity is roughly divided into three fossae. The anterior or frontal cranial fossa contains the paired frontal lobes and provides access to the nasal cavity for the olfactory nerves through the cribriform plate. The crista galli provides superior midline extension of the nasal septum. The middle cranial fossa contains the temporal lobes. In this important junction of the cranial cavity, the middle meningeal artery arises from the foramen spinosum, and the trigeminal nerve enters through the superior orbital fissure (V1), the foramen rotundum (V2), and the foramen ovale (V3). Cranial nerves II, III, IV, and VI, which traverse the cavernous sinus and enter the orbit, also course through the middle cranial fossa. The internal carotid artery is in its place in the carotid siphon as it traverses the cavernous sinus in this region. The posterior cranial fossa contains the paired cerebellar hemispheres and the brainstem. In this location, the internal auditory meatus is associated with the seventh and eighth cranial nerve complex. The jugular foramen, transverse sinus, and foramen magnum are the major landmarks of the posterior cranial fossa.
 Figure 1.1 Scalp, cranium, and intracranial cavity. A: 1, Coronal suture; 2, superior temporal line; 3, inferior temporal line; 4, os parietale; 5, squamous suture; 6, parietomastoid suture; 7, lambdoid suture; 8, occipital bone; 9, occipitomastoid suture; 10, mastoid process; 11, external acoustic meatus; 12, styloid process; 13, condyle of mandible; 14, coronoid process of mandible; 15, body of mandible; 16, mental foramen; 17, zygomatic bone; 18, infraorbital foramen; 19, frontal process (maxilla); 20, anterior nasal spine; 21, nasal bone; 22, lacrimal bone; 23, orbital lamina of ethmoid bone; 24, glabella; 25, sphenoid bone; 26, pterion; 27, temporal bone. B: 1, Sphenoid bone; 2, frontal bone; 3, anterior cranial fossa; 4, anterior clinoid process; 5, carotid sulcus; 6, middle cranial fossa; 7, petrous portion of temporal bone; 8, internal acoustic meatus; 9, jugular foramen; 10, mastoid foramen; 11, hypoglossal canal; 12, foramen magnum; 13, posterior cranial fossa; 14, sulcus for greater and lesser petrosal nerves; 15, foramen spinosum; 16, foramen ovale; 17, foramen lacerum; 18, foramen rotundum; 19, superior orbital fissure; 20, optic canal; 21, anterior ethmoidal foramen; 22, anterior ethmoidal foramen; 23, foramen cecum. |
EYELID, ORBIT, AND EYE
Eyelids
The upper and lower eyelids are similar in structure, although the upper eyelid is more mobile and has features not found in the lower eyelid. The space between the eyelids is known as the palpebral fissure, which is limited medially and laterally by the canthi. At the medial canthus is the lacrimal caruncle, where there is a small lake of tears and the tiny papillae of the lacrimal duct system. The conjunctiva is a thin mucous membrane layer that covers the inner aspects of the eyelids and extends onto the surface of the globe.
Tarsus
The upper tarsal plate provides rigidity to the upper eyelid and is larger than the lower tarsus (Fig. 1.2). Each eyelid consists (from without inward) of skin, subcutaneous tissue, voluntary muscle of the orbicularis oculi, orbital septum, tarsus, smooth muscle, and conjunctiva. The more freely mobile upper lid receives the insertion of the levator palpebrae superioris muscle. The orbicularis oculi is the sphincteric muscle of the upper and lower eyelids. It attaches at a medial palpebral ligament and spreads in an arc laterally and inferiorly to provide a sphincteric muscle to the eye. It receives innervation from the temporal and zygomatic branches of the facial nerve. This muscle interdigitates with the frontalis muscle and the corrugator supercilii.
Blood Supply
The arterial supply of the eyelids is provided by the angular branch of the facial artery, which forms an anastomotic network with the supraorbital and supratrochlear artery and shares a small contribution from the superficial temporal vessels. The veins of the eyelids are larger and more numerous than the arteries and drain into the ophthalmic and angular veins medially and the superficial temporal vein laterally. Accompanying the peripheral arterial arcade of the upper eyelid, the veins of the small venous plexus drain into the ophthalmic vein, which drains posteriorly to the cavernous sinus. The veins in this region of the face do
not have valves and may propagate septic emboli posteriorly. This is a particularly dangerous situation for patients who have infections in the areas of the eyelids or periorbital abscess. These patients are at risk of cavernous sinus thrombosis.
not have valves and may propagate septic emboli posteriorly. This is a particularly dangerous situation for patients who have infections in the areas of the eyelids or periorbital abscess. These patients are at risk of cavernous sinus thrombosis.
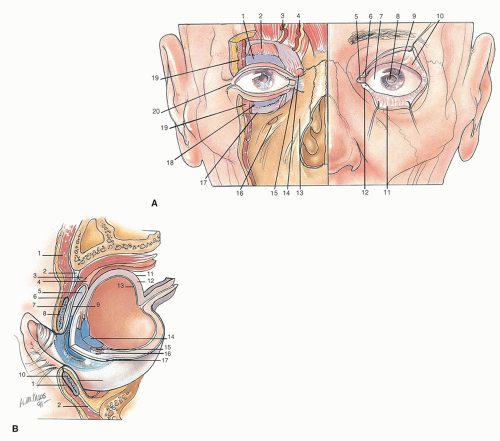 Figure 1.2 Eyelids and external adnexa. A: 1, Superior tarsus; 2, levator palpebrae superioris muscle; 3, supraorbital artery and nerve; 4, supratrochlear artery and nerve; 5, lacrimal caruncle; 6, superior lacrimal papilla and puncta; 7, bulbar conjunctiva over sclera; 8, pupil; 9, cornea; 10, superior palpebral conjunctiva; 11, inferior palpebral conjunctiva; 12, inferior lacrimal papilla and puncta; 13, maxilla; 14, lacrimal sac; 15, medial palpebral ligament; 16, infraorbital foramen; 17, orbital septum; 18, inferior tarsus; 19, orbicularis oculi muscle (cut); 20, lateral palpebral ligament. B: 1, Orbicularis oculi muscle; 2, orbital septum; 3, levator palpebrae superioris muscle; 4, superior tarsal muscle (Müller muscle); 5, superior conjunctival fornix; 6, orbicularis oculi muscle (palpebral portion); 7, superior tarsus; 8, tarsal glands; 9, palpebral conjunctiva; 10, inferior tarsus; 11, sclera; 12, choroid; 13, retina; 14, lens; 15, iris; 16, anterior chamber; 17, cornea. |
Lacrimal System
The lacrimal apparatus consists of a secretory portion, the lacrimal gland, its ducts, the drainage apparatus, the lacrimal canaliculi and sac, and the nasolacrimal duct (Fig. 1.3). The lacrimal gland is partially divided into two portions by the lateral horn of the aponeurosis of the levator palpebrae. The larger orbital portion of the gland lies in a shallow fossa on the frontal bone and is in contact anteriorly with the orbital septum. The excretory ductules of the lacrimal gland run through the orbital part of the gland, run through or close to the posterior part of the palpebral portion, and are joined by ducts from this portion.
Removal of the palpebral portion can destroy the drainage of the entire gland.
Removal of the palpebral portion can destroy the drainage of the entire gland.
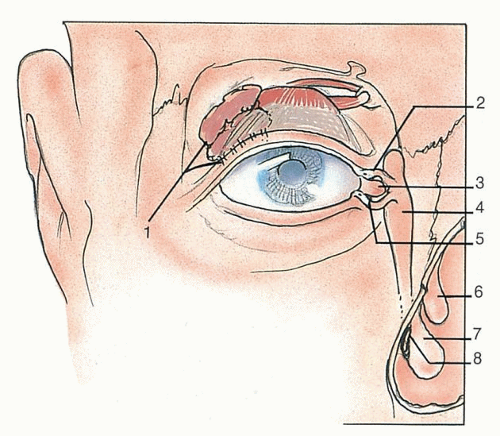 Figure 1.3 Lacrimal apparatus and drainage system. 1, Lacrimal gland and ducts; 2, superior lacrimal papilla and puncta; 3, lacrimal caruncle; 4, lacrimal sac; 5, inferior lacrimal papilla and puncta; 6, middle nasal concha; 7, inferior nasal concha; 8, opening of nasolacrimal duct. |
 Figure 1.4 Bony orbit. |
Movement of the eyelid distributes tears over the surface of the eye, and any excess tends to accumulate in the lacrimal lake. This structure drains into the paired superior and inferior canaliculi and from there into the lacrimal sac. The lacrimal sac is housed in the bony lacrimal fossa of the medial orbital wall. This drains into the nasal lacrimal duct and eventually into the inferior meatus of the nose.
Orbit
The bony orbit consists of the medial wall occupied largely by the ethmoid bone, lacrimal bone, and a portion of the nasal process of the maxilla (Fig. 1.4). The floor of the orbit consists of the roof of the maxilla. The inferior orbital fissure is at its lateral extent. The zygomatic bone and greater wing of the sphenoid form the lateral orbital wall and join the frontal bone superiorly to complete the pyramidal bony orbit. On its medial aspect are the paired ethmoidal foramina, which provide a route to the orbit for the anterior and posterior ethmoidal arteries. The optic canal posteriorly transmits the optic nerve and ophthalmic artery. The superior orbital fissure transmits cranial nerves III, IV, V, and VI and provides an aperture for the ophthalmic vein.
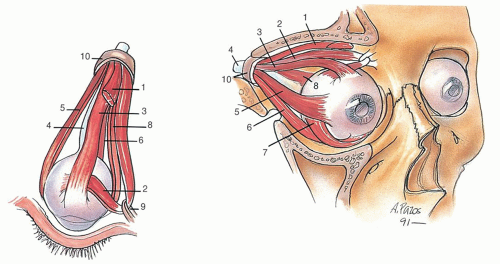 Figure 1.5 Eye muscles. 1, Levator palpebrae superioris muscle; 2, superior oblique muscle; 3, superior rectus muscle; 4, optic nerve; 5, lateral rectus muscle; 6, inferior rectus muscle; 7, inferior oblique muscle; 8, medial rectus muscle; 9, trochlea; 10, annular tendon. |
Eye
The eye consists of the cornea and sclera in the anterior aspect. The anterior chamber protrudes as a second sphere on the structure of the orbit. The lens and iris form the posterior portion of the anterior chamber. Contained within the substance of the eye is the vitreous. The retina rests on the choroid. The fovea centralis is the focal point of the eye. Asymmetric to the structure of the orbit is the insertion of the optic nerve and ciliary arteries.
The seven voluntary muscles of the orbit are the levator palpebrae superioris; the superior, inferior, medial, and lateral rectus muscles; and the superior and inferior oblique muscles (Fig. 1.5). The smooth muscles of the orbit are the orbitalis muscle, the superior and inferior tarsal muscles, and ciliary and iridial muscles within the eye. The superior oblique is supplied by cranial nerve IV, the lateral rectus
is supplied by cranial nerve VI, and the other voluntary muscles of the orbit are supplied by cranial nerve III. The tarsal and orbital muscles (of Müller) are supplied by sympathetic fibers derived from the carotid plexus and from the superior cervical ganglion. The dilator pupillae, the sphincter pupillae, and the ciliary muscle are supplied by parasympathetic fibers through the oculomotor nerve (III).
is supplied by cranial nerve VI, and the other voluntary muscles of the orbit are supplied by cranial nerve III. The tarsal and orbital muscles (of Müller) are supplied by sympathetic fibers derived from the carotid plexus and from the superior cervical ganglion. The dilator pupillae, the sphincter pupillae, and the ciliary muscle are supplied by parasympathetic fibers through the oculomotor nerve (III).
The primary blood supply to the orbit is through the ophthalmic artery. The primary drainage is through the ophthalmic vein, which drains directly into the cavernous sinus. An additional anastomotic network is present on the anterior aspect of the face in the form of an arcade of vessels around the eyelids and through the pterygoid plexus.
THE EAR
The development and the anatomic and physiologic features of the ear are discussed in Chapters 140 and 141.
NOSE AND PARANASAL SINUSES
External Nose
The external part of the nose is a roughly pyramidal shape. The skeleton of the external nose is partly bony and partly cartilaginous and membranous. The nasal bones, which are usually narrow and thicker above, wider and thinner below, articulate firmly above with the nasal part of the frontal bone and with each other laterally with the nasal process of the maxilla (Fig. 1.6). Attached to the inferior aspect of the nasal bones are the upper lateral cartilages. These are continuous with the cartilaginous septum. In the inferior aspect, the lobule of the nose is formed mostly by the lower lateral cartilages, which consist of a medial and lateral crus. There are several small cartilages within the nasal ala. The chief arterial supply of the nose is from the facial artery through the angular artery and superior labial arteries. Venous drainage is similar, with a component gaining access to the ophthalmic vein through draining vessels from the trochlear and angular veins.
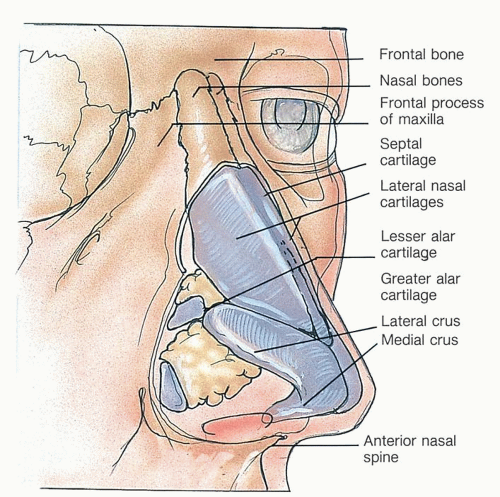 Figure 1.6 Bony and cartilaginous anatomic configuration of the external nose. |
Nasal Cavity
The nasal cavities are also known as the nasal fossae. The nasal septum consists of the nasal septal cartilage, the nasal crest of the maxilla, the nasal crest of the palatine bone, the vomer, and the perpendicular plate of the ethmoid bone. The lateral nasal wall is formed by the prominent nasal turbinates. The meatus are situated below the corresponding turbinates (Fig. 1.7). The inferior meatus provides drainage
for the nasolacrimal duct. The middle meatus provides drainage for the anterior nasal sinuses, namely the frontal sinus, anterior ethmoid sinuses, and the maxillary sinus. The superior meatus provides drainage for the posterior sinuses, namely the posterior ethmoid and sphenoid sinuses.
for the nasolacrimal duct. The middle meatus provides drainage for the anterior nasal sinuses, namely the frontal sinus, anterior ethmoid sinuses, and the maxillary sinus. The superior meatus provides drainage for the posterior sinuses, namely the posterior ethmoid and sphenoid sinuses.
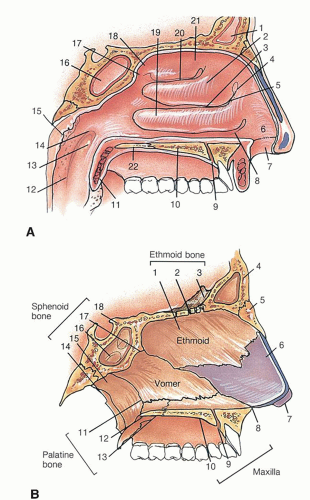 Figure 1.7 A: Lateral nasal wall. 1, Frontal sinus; 2, middle nasal concha; 3, middle nasal meatus; 4, agger nasi; 5
Get Clinical Tree app for offline access
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree


|