Surgery to Correct Nystagmus
Michael X. Repka
A patient with nystagmus seeks surgical correction for one of three reasons: to correct an anomalous head posture induced by a nystagmus, to reduce oscillopsia, or to improve visual acuity that is degraded by nystagmus.
CORRECTION OF AN ANOMALOUS HEAD POSTURE
Background
A subset of patients with congenital nystagmus adopts anomalous head postures. They adopt large face turns and anomalous head postures in the horizontal direction, the vertical direction, or both (Fig. 95-1). These patients do this to place the eyes in the null position. This position also is known as the zone of minimal intensity of the nystagmus, where the eyes have the smallest amplitude of nystagmus. Assuming this head position, the patient generally achieves the highest level of visual acuity.
 Figure 95.1. A 6-year-old patient with a 45° right gaze preference and a left head turn. This position was adopted to view objects at distance and near. |
Anderson1 and Kestenbaum2 were the first to propose surgical procedures for the correction of anomalous horizontal head postures. Their surgical procedures were an attempt to move the null position toward the primary position. Many authors subsequently have addressed the surgical treatment of anomalous head postures associated with congenital nystagmus, most recently Scott and Kraft,3 Mitchell et al,4 Biglan et al,5 and Kraft et al.6 Such corrective surgery has been shown to be beneficial by eye movement recordings. There is a shift of the null position toward the primary position and a decrease in the intensity of the nystagmus.7,8,9 In addition, the eye movement recordings demonstrate that the null region is broadened in some patients, allowing a wider angle of best visual acuity compared with the preoperative state.
Indications
The usual indication for such a surgical procedure is to reduce or eliminate an extreme head posture. Some patients are bothered by neck and back pain from long-standing torticollis. Others achieve the desired reconstruction of eye position, improved visual acuity, and improved stereoacuity.
Preoperative evaluation mirrors that for any patient with nystagmus. A complete ophthalmologic history and examination is needed to elicit the cause of the congenital nystagmus. A pupillary examination for evidence of optic neuropathy or paradoxical pupillary reactions is prudent in the search for a sensory cause. Electroretinography may be done if there is markedly reduced vision. Neuroimaging is not necessary, unless the nystagmus is acquired or there is optic atrophy. The examiner should observe the patient for at least 10 minutes to be certain that the preferred gaze direction is constant. Congenital nystagmus can present with a periodic, alternating waveform with two different null zones. In such a situation, a Kestenbaum-Anderson type of surgery would be potentially harmful. Four-muscle recession surgery has been suggested for these patients (see later).10
Contraindications
There are no absolute contraindications. Surgery probably is best deferred until at least age 4 or 5 years. This allows for the surgeon to more accurately determine the operative angle and for the patient to be visually mature so that binocularity is less vulnerable to disruption.
Surgical Procedure
The surgical approach for patients with straight eyes is to move each eye by an equal amount in the direction of the face turn. If there is a strabismus in addition to an anomalous head posture, the surgeon needs to decide whether to correct both in one operation or to pursue correction in two operations.
The approach to the patient with straight eyes and an anomalous head posture follows: The operation should be viewed as one in which the surgeon mechanically moves the eyes in the direction of the face turn (opposite the gaze preference). Thus, a patient in left gaze with a right face turn would undergo a resection of the right lateral rectus, a recession of the right medial rectus, a resection of the left medial rectus, and a recession of the left lateral rectus muscles. The surgeon should take a diagram to the operating room clearly outlining the surgery to be performed (Fig. 95-2). It is easy during the course of the performance of the surgery to get confused about which muscle undergoes which surgical procedure.
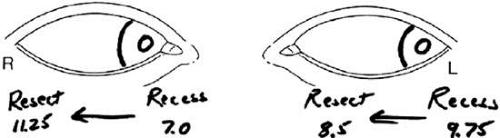 Figure 95.2. A diagram documenting the surgical plan should be taken into the operating room to ensure performance of the appropriate surgery. In this illustration, the patient’s eyes are drawn in left gaze. The planned recessions of the left lateral rectus and right medial rectus, as well as the planned resections of the left medial rectus and right lateral rectus, are identified. |
The amounts of surgery to be performed are controversial. The classic maximum amount of surgery was formulated by Parks and Mitchell.11,12 Their operation used the guidelines of 5-6-7-8 for the amounts of surgery. These were based on a 5.0-mm medial rectus muscle recession, the maximum medial rectus muscle operation of that period. In my example of a right face turn, the surgery would entail a 5.0-mm recession of the right medial rectus, an 8.0-mm resection of the right lateral rectus, a 7.0-mm recession of the left lateral rectus, and a 6.0-mm resection of the left medial rectus muscle. Notice that the millimeters of surgical correction provided are the same for each eye. Unfortunately, this amount of surgery left many undercorrected patients. Surgeons responded over the ensuing two decades by increasing the amounts of surgery beyond these “maximal amounts.”3,4,13
Before selecting the amount of surgery to be performed, the surgeon must determine the magnitude of the head turn. The patient views a letter chart at distance with the smallest size optotype visible. This helps to establish the maximum deviation. An orthopedic goniometer is one convenient tool for measuring the deviation.4 The head turn is measured in degrees, not prism diopters. The size of the head turn dictates the amount of surgical augmentation. For an anomalous head posture of ≤20° in the horizontal direction, an augmentation of 20% over the 5-6-7-8 guidelines is necessary. Surgical amounts are augmented by 30% for an anomalous position of 21° to 39°. An augmentation of 40% is necessary for head turns of ≥40°. The amounts of horizontal surgery for these head postures are listed in Table 95-1. Nelson et al13 suggest that for head postures <45°, an augmentation of 60% is beneficial.13 No other reports lend further substantiation to the efficacy of this marked augmentation.
TABLE 95-1. Surgical Correction of Anomalous Head Postures | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


