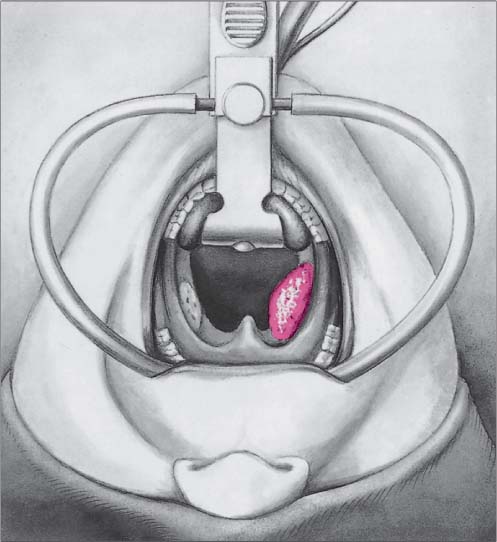
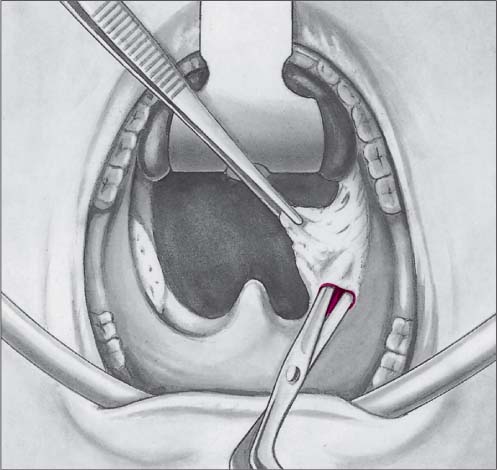
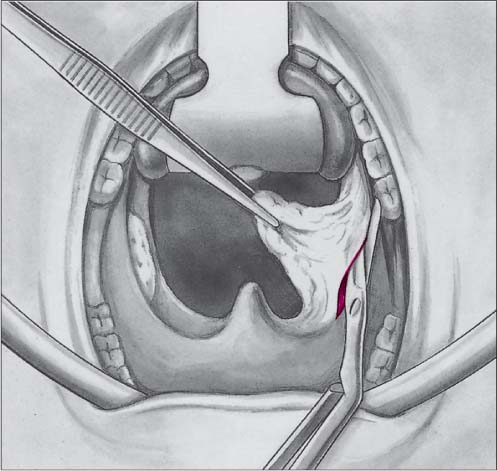
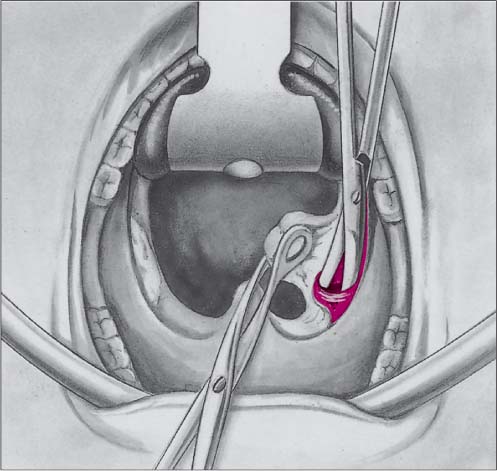
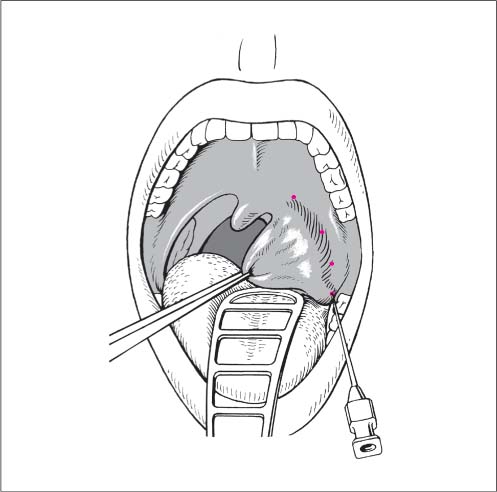
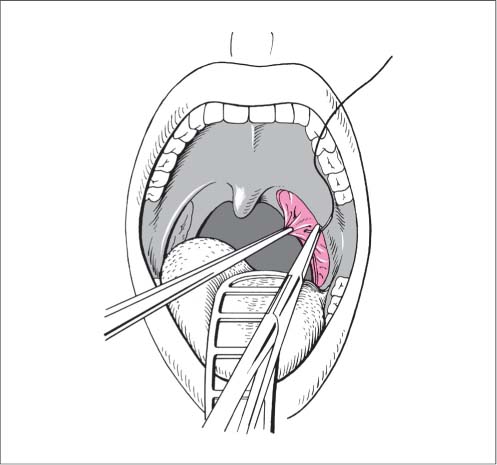
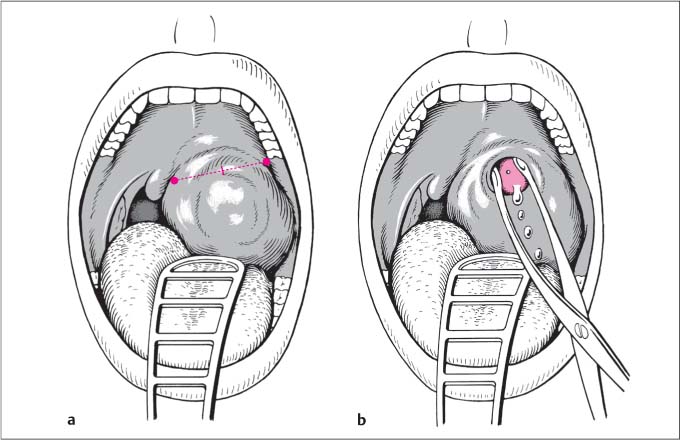
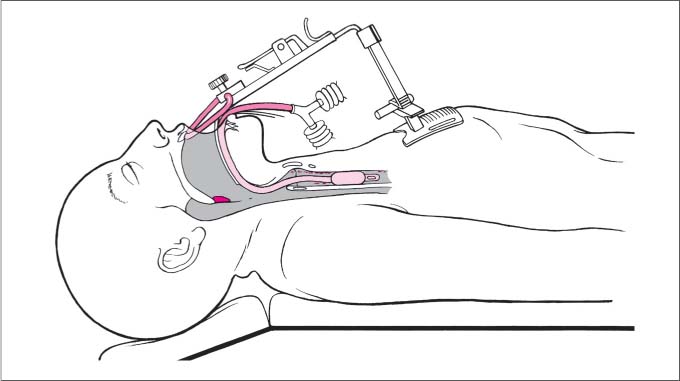
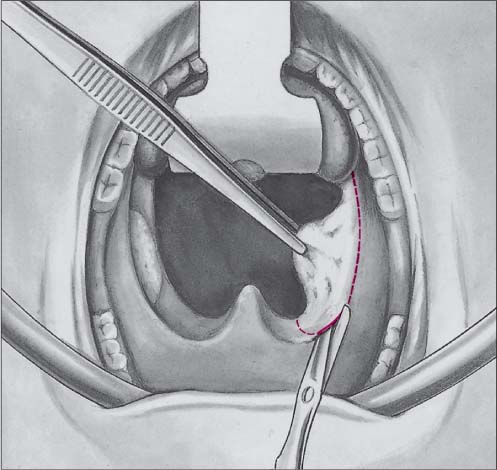
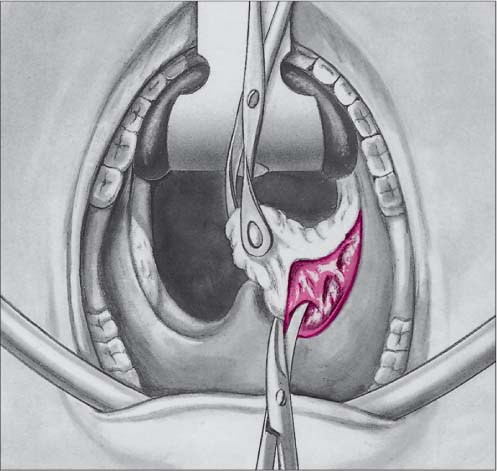
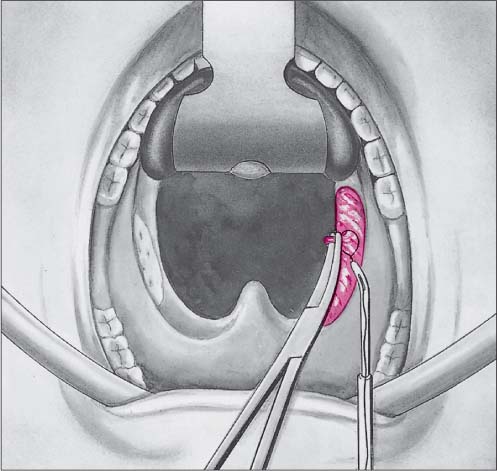
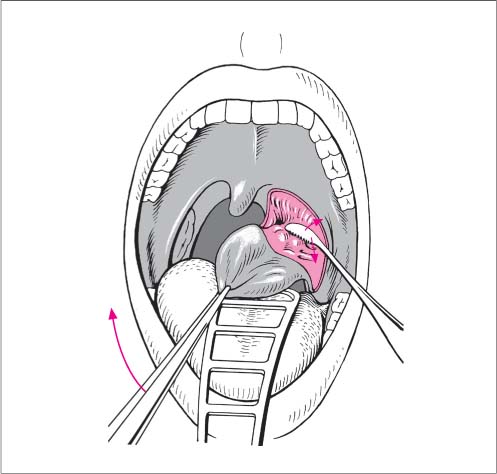
9 Surgery of the Oral Cavity and Oropharynx Complete removal of the tonsillar tissue with its crypts along the capsular plane. – children up to the age of 14 – adults with intellectual or autonomic lability or epilepsy – abscess tonsillectomy – hypertensive patients or patients with coagulopathy (more meticulous hemostasis). Fig. 9.1 Tonsillectomy under general anesthesia. The surgeon sits at the head of the patient, which is slightly lowered and reclined. Exposure of the tonsils (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Positioning. The surgeon sits at the head of the patient, slight head-down position, reclination (Fig. 9.1) (“hanging head” or Rose position). Exposure. The oral intubation tube, fixed exactly in the middle of the lower lip, is fixed in the groove of the McIvor blade. While remaining closed, the McIvor gag is advanced carefully deeper, levering slightly (correct blade size: largely covering the tongue, but not touching the mandibular arch, teeth or posterior pharyngeal wall). The frame of the mouth gag is supported between the canines and the incisors (Fig. 9.2). The gag is carefully opened (risk of overstretching the temporomandibular joint, pressure palsy of the hypoglossal or lingual nerves, kinking of the tube). The tonsil must nevertheless still be visible as far as the glossotonsillar sulcus. The chest support or holder is attached. Incision. The tonsillar tissue is grasped by its superior pole and drawn medially and downward. The mucous membrane is incised with nasal scissors or scalpel along the edge of the anterior soft palate (recognizable by moving the tonsil to and fro) (Fig. 9.3). Careful tangential spreading and retraction of the muscles with the scissors in a lateral direction will allow identification of the capsule, shining through as a grayish-white layer (Fig. 9.4). The tissue is spread apart along the subcapsular plane to allow incision of the anterior pillar down to its attachment to the tongue (Fig. 9.5). Superior pole. While continuous traction is maintained on the tonsil in a medial and downward direction, the superior pole is exposed, using the curved tonsil scissors and keeping strictly to the subcapsular plane (Fig. 9.6). The posterior pillar is undermined with spreading movements in a downward direction. The posterior pillar is then incised (Fig. 9.7). Dissection. The grasping forceps are placed on the tonsil tissue and drawn firmly down in a medial direction. The peritonsillar tissue is swept off using the Henke rasp, small gauze dissector, or tonsil scissors (Fig. 9.8); dissection is always directed away from the tonsil. Readjusting the grasping forceps will keep the tonsillar tissue under tension. Resection. The tonsil is pedicled beyond the triangular fold down to the base of the tongue, to be then resected beneath the inferior pole using the tonsil sling (Fig. 9.9). Hemostasis. Important: when operating on individuals with Down Syndrome, special attention must be paid to a very careful procedure, because they are particularly prone to subluxation of the cervical spine if they are hyperextended. Fig. 9.2 Tonsillectomy under general anesthesia. Larger spurting vessels are grasped with forceps, the tissue cone is drawn laterally, a clamp is passed beneath it (Fig. 9.10) and the tissue is ligated (either a Röder loop is used or the knot is drawn down with a clamp or slider) (Fig. 9.11) or secured with a suture ligation. When passing the needle for the suture ligation, adequate traction must be placed on the clamp before the needle is inserted tangentially at the base of the tissue to avoid collateral damage in the depths (Fig. 9.12). Minor bleeds can be coagulated with the bipolar diathermy forceps (Fig. 9.13). Fig. 9.3 Tonsillectomy under general anesthesia. Incision of the mucosal margin of the anterior pillar, the position of which is confirmed by repeated medial traction (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Fig. 9.4 Tonsillectomy under general anesthesia. Identification of the capsule by spreading and retracting the muscles (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Fig. 9.5 Tonsillectomy under general anesthesia. Incision of the anterior pillar as far as the attachment of the tongue (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Fig. 9.6 Tonsillectomy under general anesthesia. Exposure of the superior pole by undermining along the plane of the capsule (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Fig. 9.7 Tonsillectomy under general anesthesia. Incision of the posterior pillar (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Fig. 9.8 Tonsillectomy under general anesthesia. Dissection of the tonsils by sweeping off the peritonsillar tissue with the Henke rasp (after Theissing in Naumann HH. Kopf- und HalsChirurgie [Head and Neck Surgery]). Fig. 9.9 Tonsillectomy under general anesthesia. Removal of the tonsils at the base of the tongue using a tonsil snare (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Fig. 9.10 Tonsillectomy under general anesthesia. An artery clip is placed after applying traction to the tissue (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Fig. 9.11 Tonsillectomy under general anesthesia. Vessel ligation using a Röder loop (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Fig. 9.12 Tonsillectomy under general anesthesia. Suture ligation. The needle is inserted superficially through the tissue (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Fig. 9.13 Tonsillectomy under general anesthesia. Cauterization using a bipolar forceps (after Theissing in Naumann HH. Kopf- und Hals-Chirurgie [Head and Neck Surgery]). Basic measures: – exclude aspiration, if necessary intubate and perform bronchoscopic suction – check hemoglobin, blood pressure, and pulse – venous access, infusion, if necessary transfusion – clotting profile. Local measures: – suck away coagulated blood, infiltrate the source of bleeding with a vasoconstrictor and local anesthetic – bipolar diathermy or suture ligation of the source of bleeding, under general anesthesia if necessary – cover the wound bed with a collagen fleece soaked in fibrin glue in the presence of coagulopathy. Locally persistent arterial bleeding: – After packing the wound bed and pharynx, ligation from an external approach. Skin incision over the sternocleidomastoid, identification of the carotid sheath, ligation of the facial and retromandibular veins, follow the course of the branches of the external carotid artery, lingual artery, facial artery, ascending pharyngeal artery and ligate as peripherally as possible. – Alternatively, consider the occasional option of performing an angiography and embolizing the damaged vessel. Timely premedication with sufficient atropine administration (salivation interferes with the topical anesthesia and is a hindrance during the operation). Topical anesthesia is sprayed onto the tongue, tonsillar pillars, and posterior wall of the pharynx. Infiltration anesthesia with 20 mL 1 % lidocaine plus epinephrine (1:200 000). The mouth-gag blade is placed directly next to the tonsil to allow the triangular fold to be also placed under tension. Subcutaneous infiltration of the mucosa of the pillars as far as the tongue (Fig. 9.14). The tonsil is displaced medially with forceps and the peritonsillar tissue is infiltrated with three depots of 2 mL each into the groove that then comes into view (Fig. 9.15). The tonsil itself must not be injected. Always aspirate before injecting. Apply 2 mL each to the inferior pole and in the region of the triangular fold. Wait 5–10 minutes to allow for better vasoconstriction. Fig. 9.14 Tonsillectomy under local anesthesia. Subcutaneous infiltration of the mucosa. Fig. 9.15 Tonsillectomy under local anesthesia. Peritonsillar infiltration. Fig. 9.16 Tonsillectomy under local anesthesia. Incision of the mucosa and identification of the tonsillar capsule. Fig. 9.17 Tonsillectomy under local anesthesia. Incision along the anterior tonsillar pillar. Fig. 9.18 Tonsillectomy under local anesthesia. Detachment of the peritonsillar tissue from the capsule using the rasp. Fig. 9.19 Tonsillectomy under local anesthesia. Ligation below the inferior pole of the tonsil using the tonsil snare. Fig. 9.20 Tonsillectomy under local anesthesia. Suture ligation of a vessel. The procedure is the same as for tonsillectomy under general anesthesia and adenoidectomy. If adenoidectomy is done first, the nasopharyngeal pack for hemostasis may be left during tonsillectomy. This saves an additional waiting period while performing hemostasis in the nasopharynx. Removal of the swabs at the end of the operation must be ensured. Instead of the conventional blunt-sharp dissection using instruments, the tonsils may also be dissected using a laser. Nd:YAG and potassium titanyl phosphate (KTP) lasers are preferred, in addition to the CO2 laser. Basically, laser tonsillectomy is associated with less bleeding, although the larger vessels that are disrupted nevertheless require bipolar coagulation. The frequency of postoperative bleeding is the same as in the conventional technique, while wound healing appears to be slightly delayed; usually a somewhat stronger edema of the uvula develops. Postoperative pain lasts slightly longer. Guidelines for laser protection must be followed: protect the tube from igniting, protect the posterior wall of the pharynx from inadvertent radiation by covering it with a damp swab layer, use safety glasses, etc. The technique follows the same steps as for the conventional approach. More traction is needed on the superior tonsil pole to bring the tissue more into the surgical site for dissection because the laser only cuts in a straight line. For tonsillar hypertrophy in infants, where the part of the tonsil that extends beyond the anterior and posterior pillars is resected tangentially, laser tonsillotomy has recently been once again propagated as an alternative to tonsillectomy. Genuine long-term follow-ups, which have led to abandonment of the once-customary tonsillotomy using cutting instruments because of the significant late complications, are so far not available. Argon-plasma coagulation (APC) is a special technique for applying high-frequency radiation for thermal dissection and coagulation. When using Bergler APC dissector, the technical procedure is the same as when using conventional instruments. Operating time is supposed to be shorter because there is less intraoperative bleeding. Incision and drainage of peritonsillar accumulations of pus. Para- (supra-, retro-, intra-) tonsillar abscesses. Needle drainage. Use a syringe with an attached large-bore needle. The needle is inserted directly above the superior pole of the tonsil, in the middle of an imaginary line between the base of the uvula and the superior wisdom tooth, or at the most prominent site. Under continuous aspiration, the needle is advanced deeper in an exactly sagittal direction until pus is encountered. Incision and drainage. From the aforementioned puncture site, an incision is made obliquely downward from medial–superior to lateral–inferior for a distance of 1.5 cm; the incision is also deepened in a sagittal direction to a depth of 1.5 cm with a scalpel or dressing forceps or a tonsil spreader and widened until the abscess cavity is completely drained. The pus is removed by suction (Fig. 9.21a, b). Removal of the tonsils along the subcapsular plane with the simultaneous drainage of the abscess. As a rule, the same as for tonsillectomy (see p. 155); imminent complications such as sepsis, thrombosis of the jugular vein, necrotizing fasciitis, or septic necrosis of the carotid artery, however, outweigh the relative contraindications. As for tonsillectomy (see p. 155). As for tonsillectomy under general anesthesia. As a rule, general endotracheal anesthesia. Be aware of intubation problems; consider fiber-optic intubation. The approach is basically the same as for tonsillectomy under general anesthesia. The mucosal incision is oriented along the base of the uvula and the triangular fold. Suture repair of any incision from a previous abscess incision will avoid tearing it further. Because of the brittleness of the tissue, the capsule and superior pole must be identified without any significant traction on the tonsillar tissue and without pressure on the peritonsillar tissue. This is done by blunt dissection and without abrupt spreading with the tonsil scissors. The curve of the scissor blades lies against the tonsil when releasing the superior pole and the lateral and anterior surfaces of the tonsil. This type of dissection leads inevitably to the abscess cavity. A culture swab for bacteriological examination is taken from the cavity. Fig. 9.21a, b Peritonsillar abscess. a Site for needle drainage/incision. b Spreading open the incision wound. Any significant bleeds are secured by suture ligation, and any minor bleeding is easily controlled by bipolar coagulation. A swab placed temporarily into the tonsillar recess will also stop any oozing. The contralateral tonsil is generally removed as well. As for tonsillectomy (see p. 160). Wide drainage of the abscess. Any retropharyngeal abscess. Usually general anesthesia, but local anesthesia is also an option for adults. Generally as for tonsillectomy; consider enteral nutrition initially. Adjust antibiotics according to the swab results. Open up the incision wound again if there is retention of pus.
Surgery of the Tonsils
Tonsillectomy
Surgical Principle
Indications
 Recurrent tonsillitis: the indication for surgery should be considered most carefully for children under 4 years of age.
Recurrent tonsillitis: the indication for surgery should be considered most carefully for children under 4 years of age.
 Chronic tonsillitis with local symptoms, halitosis, or cervical lymphadenopathy.
Chronic tonsillitis with local symptoms, halitosis, or cervical lymphadenopathy.
 Peritonsillar abscess.
Peritonsillar abscess.
 Tonsillar sepsis or deep neck infection.
Tonsillar sepsis or deep neck infection.
 Infection with suspected tonsillar focus (rheumatic fever, endocarditis, certain forms of glomerulonephritis, palmar plantar pustulosis).
Infection with suspected tonsillar focus (rheumatic fever, endocarditis, certain forms of glomerulonephritis, palmar plantar pustulosis).
 Excessive tonsillar hyperplasia with obstructive sleep apnea syndrome, difficulty in swallowing.
Excessive tonsillar hyperplasia with obstructive sleep apnea syndrome, difficulty in swallowing.
 Monocytic angina with considerable obstruction causing breathing and swallowing difficulties.
Monocytic angina with considerable obstruction causing breathing and swallowing difficulties.
 Suspected tumor of the tonsils (biopsy for histological examination).
Suspected tumor of the tonsils (biopsy for histological examination).
 Suspected tonsillar primary lesion of tuberculous cervical lymphadenopathy.
Suspected tonsillar primary lesion of tuberculous cervical lymphadenopathy.
Contraindications
 Cardiovascular compromise, severe hypertension.
Cardiovascular compromise, severe hypertension.
 Severe general disease.
Severe general disease.
 Leukemia, agranulocytosis.
Leukemia, agranulocytosis.
 Hepatic failure.
Hepatic failure.
 Coagulopathy: in exceptional urgent indications, special techniques (fibrin glue, replacement of blood components, laser surgery) may allow surgery after hematological pre-assessment.
Coagulopathy: in exceptional urgent indications, special techniques (fibrin glue, replacement of blood components, laser surgery) may allow surgery after hematological pre-assessment.
 Overt, repaired, or submucous cleft palate: deterioration in speech is possible despite meticulous protection of the muscles; a speech and language therapist should be consulted if the indication is still clinically urgent.
Overt, repaired, or submucous cleft palate: deterioration in speech is possible despite meticulous protection of the muscles; a speech and language therapist should be consulted if the indication is still clinically urgent.
 Singers: a change in voice is possible due to postoperative alterations to the resonating cavity secondary to scar formation.
Singers: a change in voice is possible due to postoperative alterations to the resonating cavity secondary to scar formation.
 Severe atrophic pharyngitis.
Severe atrophic pharyngitis.
 Polio vaccination: interval of 6 weeks.
Polio vaccination: interval of 6 weeks.
Specific Points Regarding Informed Consent
 Severe intra- and postoperative hemorrhage with the risk of aspiration and hypoxia, hypovolemic shock.
Severe intra- and postoperative hemorrhage with the risk of aspiration and hypoxia, hypovolemic shock.
 Inflammatory complications—infection of the wound bed, cervical lymphadenopathy, retro- and parapharyngeal abscess, deep neck infection, thrombosis of the jugular vein, and mediastinitis.
Inflammatory complications—infection of the wound bed, cervical lymphadenopathy, retro- and parapharyngeal abscess, deep neck infection, thrombosis of the jugular vein, and mediastinitis.
 Disorders of taste, difficulty in swallowing, reduction of tongue mobility.
Disorders of taste, difficulty in swallowing, reduction of tongue mobility.
 Damage to teeth, damage to the temporomandibular joint, velopalatine insufficiency, disturbances in swallowing and speech (change in voice).
Damage to teeth, damage to the temporomandibular joint, velopalatine insufficiency, disturbances in swallowing and speech (change in voice).
Operative Planning
 Any (family) history of bleeding or coagulation problems.
Any (family) history of bleeding or coagulation problems.
 PT, PTT, INR, platelet count, blood count, bleeding time test.
PT, PTT, INR, platelet count, blood count, bleeding time test.
 Perioperative antibiotics if appropriate, e. g., prophylaxis against endocarditis.
Perioperative antibiotics if appropriate, e. g., prophylaxis against endocarditis.
Special Instruments
 Mouth gag, e. g., McIvor gag, in various sizes.
Mouth gag, e. g., McIvor gag, in various sizes.
 Blunt curved tonsil scissors.
Blunt curved tonsil scissors.
 Pointed long scalpel or long angled scissors.
Pointed long scalpel or long angled scissors.
 Henke tonsil elevator.
Henke tonsil elevator.
 Tonsil snare, Röder loop.
Tonsil snare, Röder loop.
 Long clamp, long needle holder, and long forceps.
Long clamp, long needle holder, and long forceps.
 Tonsil grasping forceps.
Tonsil grasping forceps.
 Tonsil sucker.
Tonsil sucker.
 Conchotome (round jaw).
Conchotome (round jaw).
 Bipolar coagulation forceps.
Bipolar coagulation forceps.
 Fenestrated tongue depressor.
Fenestrated tongue depressor.
Anesthesia
 General anesthesia with intubation or laryngeal mask, or alternatively local anesthesia.
General anesthesia with intubation or laryngeal mask, or alternatively local anesthesia.
 General anesthesia is appropriate for:
General anesthesia is appropriate for:
Surgical Technique

 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 Always dissect within the correct plane along the tonsillar capsule. If the capsule is inadvertently breached, then it is identified again, more laterally and caudally, using the same principle.
Always dissect within the correct plane along the tonsillar capsule. If the capsule is inadvertently breached, then it is identified again, more laterally and caudally, using the same principle.
 In the region of the inferior tonsillar pole/triangular fold, the layer sometimes retracts medially and can be lost. The grasping forceps should therefore be placed close to the plane of dissection and the tissue held well under tension in a medial and downward direction. Bipolar hemostasis should be secured during dissection to achieve better visualization. Remains of the triangular fold are removed with the conchotome.
In the region of the inferior tonsillar pole/triangular fold, the layer sometimes retracts medially and can be lost. The grasping forceps should therefore be placed close to the plane of dissection and the tissue held well under tension in a medial and downward direction. Bipolar hemostasis should be secured during dissection to achieve better visualization. Remains of the triangular fold are removed with the conchotome.
 To avoid leaving behind remains of the inferior pole and the triangular fold—which may become the initial site of recurrent local inflammations—incision of the anterior and posterior pillars is continued as far as the glossotonsillar sulcus.
To avoid leaving behind remains of the inferior pole and the triangular fold—which may become the initial site of recurrent local inflammations—incision of the anterior and posterior pillars is continued as far as the glossotonsillar sulcus.
 The wound bed should be well exposed when securing hemostasis to enable adequate visualization of the source of bleeding. Avoid pulling on the grasping clamp and placing suture ligations with large bites, otherwise there is the risk of injuring adjacent structures or breaking off the needle.
The wound bed should be well exposed when securing hemostasis to enable adequate visualization of the source of bleeding. Avoid pulling on the grasping clamp and placing suture ligations with large bites, otherwise there is the risk of injuring adjacent structures or breaking off the needle.
 The pharynx should be carefully suctioned before extubation.
The pharynx should be carefully suctioned before extubation.
 Severe intraoperative hemorrhage from abnormal vessels extending to the tonsillar bed (branches of the external carotid artery, ascending and descending pharyngeal artery, descending palatine artery, lingual artery and, in exceptional cases, the internal carotid artery due to kinking). Strong pulsations of the pharyngeal walls or the tonsils after exposing the pharynx are indications of abnormal courses of the vessels. If a severe hemorrhage cannot be controlled by a suture ligature from an internal access, then the carotid sheath must be exposed from an external approach. If there is any suspicion of injury to the internal carotid artery then a vascular surgeon should be involved.
Severe intraoperative hemorrhage from abnormal vessels extending to the tonsillar bed (branches of the external carotid artery, ascending and descending pharyngeal artery, descending palatine artery, lingual artery and, in exceptional cases, the internal carotid artery due to kinking). Strong pulsations of the pharyngeal walls or the tonsils after exposing the pharynx are indications of abnormal courses of the vessels. If a severe hemorrhage cannot be controlled by a suture ligature from an internal access, then the carotid sheath must be exposed from an external approach. If there is any suspicion of injury to the internal carotid artery then a vascular surgeon should be involved.
 Injury to the glossopharyngeal nerve, which runs near the tonsils in the inferoposterior pillar: this results in disturbances of taste and swallowing and can be caused by transsection, overgenerous suture ligation, or hypertrophic scar formation. Dissection should therefore be performed close to the capsule and suture ligatures with big bites in the region of the infero-posterior pillar should be avoided.
Injury to the glossopharyngeal nerve, which runs near the tonsils in the inferoposterior pillar: this results in disturbances of taste and swallowing and can be caused by transsection, overgenerous suture ligation, or hypertrophic scar formation. Dissection should therefore be performed close to the capsule and suture ligatures with big bites in the region of the infero-posterior pillar should be avoided.
 Postoperative bleeding: most commonly on the day of the operation, on the first postoperative day, as well as between the fifth and seventh postoperative days in the form of a delayed bleed. Postoperative bleeding may occur as late as 14 days after surgery, and in exceptional cases even later.
Postoperative bleeding: most commonly on the day of the operation, on the first postoperative day, as well as between the fifth and seventh postoperative days in the form of a delayed bleed. Postoperative bleeding may occur as late as 14 days after surgery, and in exceptional cases even later.
 Para- and retropharyngeal abscess, wound-bed infection, thrombosis of the jugular vein, deep neck infection, suppurative cervical lymphadenopathy.
Para- and retropharyngeal abscess, wound-bed infection, thrombosis of the jugular vein, deep neck infection, suppurative cervical lymphadenopathy.
 Disturbances of taste, which are rarely permanent (the administration of glucocorticoids may be tried) and are more common in the first postoperative day when they are short-term and disappear spontaneously.
Disturbances of taste, which are rarely permanent (the administration of glucocorticoids may be tried) and are more common in the first postoperative day when they are short-term and disappear spontaneously.
 Scar contracture of the soft palate with velopalatine insufficiency and disturbances of swallowing or hypernasal speech (rhinolalia aperta).
Scar contracture of the soft palate with velopalatine insufficiency and disturbances of swallowing or hypernasal speech (rhinolalia aperta).
 Injury to the hypoglossal nerve secondary to pressure from the McIvor blade.
Injury to the hypoglossal nerve secondary to pressure from the McIvor blade.
 Damage to teeth or disturbances of the temporomandibular joint from the mouth gag.
Damage to teeth or disturbances of the temporomandibular joint from the mouth gag.
Postoperative Care
 Close postoperative monitoring with inspection of the wound bed and attention to signs of internal hemorrhage (hemoptysis, increased swallowing reflex, urge to cough, stridor, aspiration, signs of hemorrhagic shock and hematemesis).
Close postoperative monitoring with inspection of the wound bed and attention to signs of internal hemorrhage (hemoptysis, increased swallowing reflex, urge to cough, stridor, aspiration, signs of hemorrhagic shock and hematemesis).
 Analgesia (no salicylic acid derivatives) especially 20–30 minutes before meals, ice pack applied to the neck.
Analgesia (no salicylic acid derivatives) especially 20–30 minutes before meals, ice pack applied to the neck.
 Antibiotics for focal or acute inflammatory reactions.
Antibiotics for focal or acute inflammatory reactions.
 Nutrition: only tea on the day of the operation, then a soft diet. Fruit and juices may burn significantly because of their acidity. More solid food may be resumed from the second postoperative week. If children are not drinking sufficiently, consider an IV infusion.
Nutrition: only tea on the day of the operation, then a soft diet. Fruit and juices may burn significantly because of their acidity. More solid food may be resumed from the second postoperative week. If children are not drinking sufficiently, consider an IV infusion.
 Initially, patients should avoid washing the hair and taking hot baths.
Initially, patients should avoid washing the hair and taking hot baths.
 Patients should avoid physical exertion completely for 2 weeks and not resume sports until after 3 weeks.
Patients should avoid physical exertion completely for 2 weeks and not resume sports until after 3 weeks.
Alternatives
Tonsillectomy under Local Anesthesia
Local Anesthesia
Surgical Technique
 Positioning: semi-seated. The surgeon stands at the side, next to the patient’s upper body.
Positioning: semi-seated. The surgeon stands at the side, next to the patient’s upper body.
 Spatula insertion: begin with the tonsil that was anesthetized first. The tongue is displaced downward and toward the contralateral side with the self-retaining spatula. The glossotonsillar sulcus must be visualized.
Spatula insertion: begin with the tonsil that was anesthetized first. The tongue is displaced downward and toward the contralateral side with the self-retaining spatula. The glossotonsillar sulcus must be visualized.
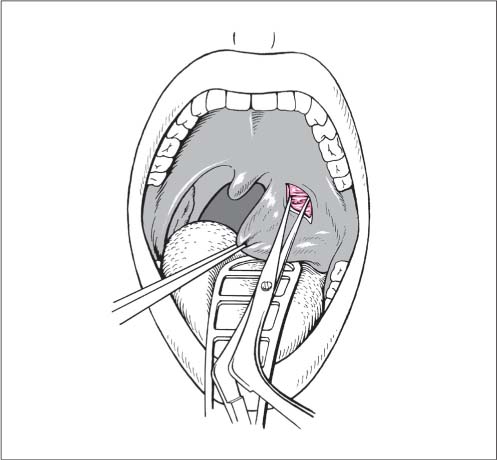
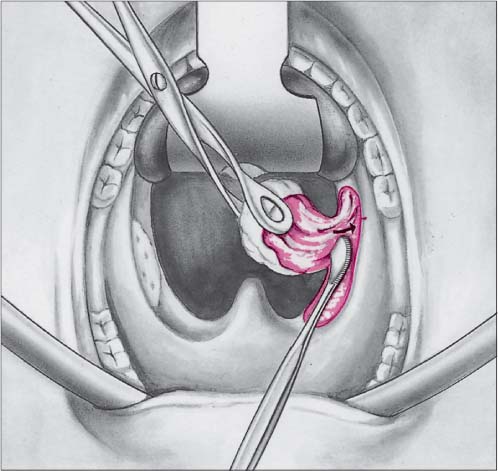
 The steps for dissection are the same as for surgery under general anesthesia, except that they are performed in the opposite direction: incision of the margin of the anterior pillar after drawing the tonsil forward. The capsule is identified with spreading movements (Fig. 9.16).
The steps for dissection are the same as for surgery under general anesthesia, except that they are performed in the opposite direction: incision of the margin of the anterior pillar after drawing the tonsil forward. The capsule is identified with spreading movements (Fig. 9.16).
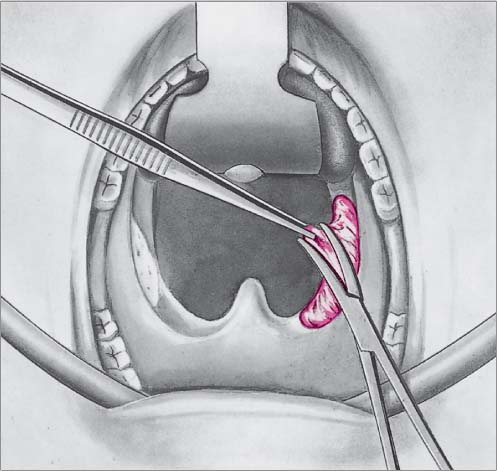
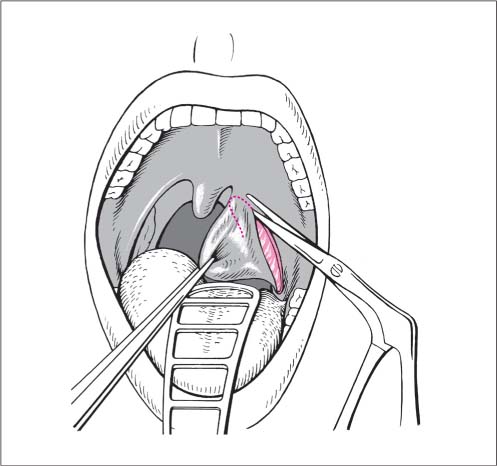
 The anterior pillar is undermined and the superior pole of the tonsil is detached using the spreading curved tonsil scissors. The posterior pillar is also undermined and incised (Fig. 9.17).
The anterior pillar is undermined and the superior pole of the tonsil is detached using the spreading curved tonsil scissors. The posterior pillar is also undermined and incised (Fig. 9.17).
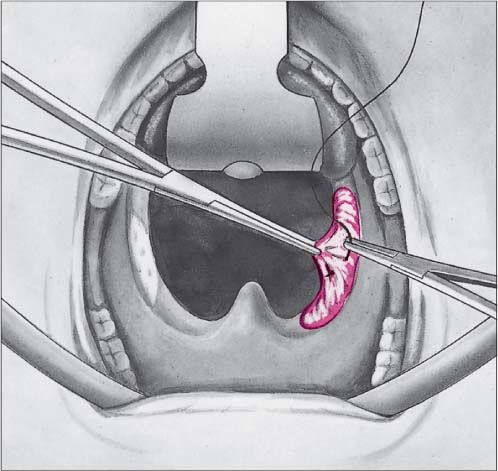
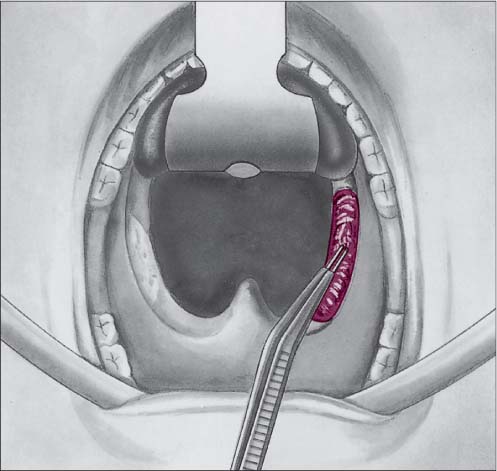
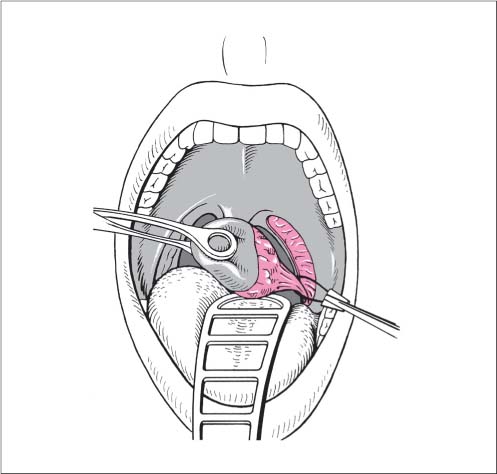
 The peritonsillar tissue is detached by dissecting the muscularis layer from the capsule, pedicled to the base of the tongue (Fig. 9.18) and removed using the tonsil snare (Fig. 9.19).
The peritonsillar tissue is detached by dissecting the muscularis layer from the capsule, pedicled to the base of the tongue (Fig. 9.18) and removed using the tonsil snare (Fig. 9.19).
 The assistant can suction during dissection to avoid aspiration and gagging.
The assistant can suction during dissection to avoid aspiration and gagging.
 More profuse bleeding should be controlled immediately by bipolar diathermy or suture ligation (Fig. 9.20).
More profuse bleeding should be controlled immediately by bipolar diathermy or suture ligation (Fig. 9.20).
Adenotonsillectomy
Laser Tonsillectomy
Tonsillectomy Using the Argon-Plasma Coagulation Dissector
Surgery for Inflammatory Complications Originating from the Tonsils
Incision and Drainage of a Peritonsillar Abscess
Surgical Principle
Indications
Contraindications
 Deep neck infection.
Deep neck infection.
 Hidden (infra- or retrotonsillar) site of the abscess (indication for abscess tonsillectomy).
Hidden (infra- or retrotonsillar) site of the abscess (indication for abscess tonsillectomy).
 Bleeding disorder (relative contraindication, consider just needle aspiration).
Bleeding disorder (relative contraindication, consider just needle aspiration).
Specific Points Regarding Informed Consent
 Aspiration.
Aspiration.
 Hemorrhage.
Hemorrhage.
 Vascular injury.
Vascular injury.
 Abscess tonsillectomy, if indicated.
Abscess tonsillectomy, if indicated.
 Postoperative care, including repeat spreading of the wound.
Postoperative care, including repeat spreading of the wound.
Operative Planning
 Laryngoscopy to exclude a life-threatening glottis edema.
Laryngoscopy to exclude a life-threatening glottis edema.
 Possible administration of cortisone, e. g., 250 mg prednisolone (decongestion of the glottis edema, pain reduction, better localization of the abscess).
Possible administration of cortisone, e. g., 250 mg prednisolone (decongestion of the glottis edema, pain reduction, better localization of the abscess).
 Antibiotics.
Antibiotics.
 Exclusion of a deep neck infection or thrombosis of the jugular vein.
Exclusion of a deep neck infection or thrombosis of the jugular vein.
 Bleeding and coagulation history.
Bleeding and coagulation history.
 PT, PTT, INR, blood count.
PT, PTT, INR, blood count.
Special Instruments
 Syringe with an attached large-bore needle.
Syringe with an attached large-bore needle.
 Scalpel or sharp spreading forceps.
Scalpel or sharp spreading forceps.
 Dressing forceps or slightly curved long tonsil clamp.
Dressing forceps or slightly curved long tonsil clamp.
 Round-headed sucker.
Round-headed sucker.
Anesthesia
 For children, general anesthesia.
For children, general anesthesia.
 For adults, apply local anesthesia using a topical anesthetic and inject lidocaine plus epinephrine intracutaneously into the mucous membrane.
For adults, apply local anesthesia using a topical anesthetic and inject lidocaine plus epinephrine intracutaneously into the mucous membrane.
Surgical Technique
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 The prior administration of cortisone facilitates identification of the abscess.
The prior administration of cortisone facilitates identification of the abscess.
 Premedication with atropine administration improves anesthesia in the highly inflamed tissue.
Premedication with atropine administration improves anesthesia in the highly inflamed tissue.
 Working down in a strictly sagittal plane avoids deviating toward the lateral-running vessels.
Working down in a strictly sagittal plane avoids deviating toward the lateral-running vessels.
 Retro- and infratonsillar abscesses are difficult to identify and are better managed by abscess tonsillectomy.
Retro- and infratonsillar abscesses are difficult to identify and are better managed by abscess tonsillectomy.
 Risks and Complications
Risks and Complications
 Vascular injury with considerable hemorrhage.
Vascular injury with considerable hemorrhage.
 Aspiration of pus into the lungs resulting in secondary pneumonia.
Aspiration of pus into the lungs resulting in secondary pneumonia.
 Glottis edema.
Glottis edema.
 Deep neck infection or jugular vein thrombosis.
Deep neck infection or jugular vein thrombosis.
Postoperative Care
 Daily opening of the wound until only small amounts of serous fluid are drained.
Daily opening of the wound until only small amounts of serous fluid are drained.
 Antibiotics.
Antibiotics.
 Consider proceeding to tonsillectomy after 3–5 days (“tonsillectomy à tiède”).
Consider proceeding to tonsillectomy after 3–5 days (“tonsillectomy à tiède”).
 Abscess tonsillectomy in the presence of severe bleeding or an abscess which is difficult to identify.
Abscess tonsillectomy in the presence of severe bleeding or an abscess which is difficult to identify.
Abscess Tonsillectomy
Surgical Principle
Indications
 Late presentation or delayed healing of incised abscesses.
Late presentation or delayed healing of incised abscesses.
 Deep or parapharyngeal abscesses, when drainage by incision is not possible.
Deep or parapharyngeal abscesses, when drainage by incision is not possible.
 Septic conditions arising from the tonsils associated with peritonsillar inflammation.
Septic conditions arising from the tonsils associated with peritonsillar inflammation.
 Persistent bleeding after abscess incision.
Persistent bleeding after abscess incision.
 Peritonsillar abscess in infants.
Peritonsillar abscess in infants.
 Peritonsillar abscesses, as an alternative to abscess incision, especially if there have been previous abscesses or a relevant history provides the indication for tonsillectomy anyway.
Peritonsillar abscesses, as an alternative to abscess incision, especially if there have been previous abscesses or a relevant history provides the indication for tonsillectomy anyway.
Contraindications
Specific Points Regarding Informed Consent
Operative Planning
 Any (family) history of bleeding or coagulation problems.
Any (family) history of bleeding or coagulation problems.
 PT, PTT, INR, platelet count, blood count, if appropriate bleeding time test.
PT, PTT, INR, platelet count, blood count, if appropriate bleeding time test.
 Inspection of the larynx and pharynx, if appropriate using fiber-optic methods.
Inspection of the larynx and pharynx, if appropriate using fiber-optic methods.
 Ultrasonography of the neck, including the carotid sheath and tonsil region.
Ultrasonography of the neck, including the carotid sheath and tonsil region.
Special Instruments
Anesthesia
Surgical Technique
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 Careful identification of the capsular plane by dissecting with the inverted Henke rasp (V-shaped gouge).
Careful identification of the capsular plane by dissecting with the inverted Henke rasp (V-shaped gouge).
 Careful bipolar coagulation provides better visualization in the surgical field.
Careful bipolar coagulation provides better visualization in the surgical field.
Postoperative Care
Alternatives
 Peritonsillar abscess incision and drainage.
Peritonsillar abscess incision and drainage.
 Laser tonsillectomy.
Laser tonsillectomy.
 Parapharyngeal abscesses extending to the carotid sheath require the additional revision of the neck from an external approach.
Parapharyngeal abscesses extending to the carotid sheath require the additional revision of the neck from an external approach.
Incision and Drainage of a Retropharyngeal Abscess
Surgical Principle
Indications
Specific Points Regarding Informed Consent
 Hemorrhage, aspiration with hypoxia.
Hemorrhage, aspiration with hypoxia.
 Aspiration of pus into the lungs with secondary pneumonia or pulmonary emphysema.
Aspiration of pus into the lungs with secondary pneumonia or pulmonary emphysema.
 Risks involved with the spontaneous course of a retropharyngeal abscess: mediastinitis, thrombosis of the jugular vein, obstruction of the larynx, vascular rupture.
Risks involved with the spontaneous course of a retropharyngeal abscess: mediastinitis, thrombosis of the jugular vein, obstruction of the larynx, vascular rupture.
Operative Planning
 Any (family) history of bleeding or coagulation problems.
Any (family) history of bleeding or coagulation problems.
 PT, PTT, INR, platelet count, blood count, bleeding time test.
PT, PTT, INR, platelet count, blood count, bleeding time test.
 Positioning for general anesthesia is supine and flat, head reclined and hanging down (Rose or “hanging head” position).
Positioning for general anesthesia is supine and flat, head reclined and hanging down (Rose or “hanging head” position).
 Perioperative antibiotics.
Perioperative antibiotics.
 Lateral soft-tissue neck radiography.
Lateral soft-tissue neck radiography.
Anesthesia
Surgical Technique
 Exposure: McIvor mouth gag as for tonsillectomy with hanging-head position.
Exposure: McIvor mouth gag as for tonsillectomy with hanging-head position.
 Aspiration using a large-bore needle.
Aspiration using a large-bore needle.
 Strictly sagittal incision running along an inferior to superior line until the abscess cavity is reached, simultaneous suctioning of the pus with the round-head aspirator, culture swab.
Strictly sagittal incision running along an inferior to superior line until the abscess cavity is reached, simultaneous suctioning of the pus with the round-head aspirator, culture swab.
 To improve drainage, the incision wound should be opened up, or converting it into a cruciate incision may be considered; nasogastric tube.
To improve drainage, the incision wound should be opened up, or converting it into a cruciate incision may be considered; nasogastric tube.
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 In cases of difficult intubation: consider endoscope-assisted intubation or use a Negus rigid emergency endoscope.
In cases of difficult intubation: consider endoscope-assisted intubation or use a Negus rigid emergency endoscope.
 Care is also needed during extubation: secure patent airways, suction pharynx well.
Care is also needed during extubation: secure patent airways, suction pharynx well.
 Risks and Complications
Risks and Complications
 Injury to the ascending palatine artery and ascending pharyngeal artery: if necessary the vascular stump should be ligated with a suture. If this is impossible, the carotid sheath can be exposed from an external approach.
Injury to the ascending palatine artery and ascending pharyngeal artery: if necessary the vascular stump should be ligated with a suture. If this is impossible, the carotid sheath can be exposed from an external approach.
 Aspiration pneumonia.
Aspiration pneumonia.
 Mediastinitis or jugular vein thrombosis.
Mediastinitis or jugular vein thrombosis.
Postoperative Care
Surgery for Deep Neck Infection Originating from the Tonsils and for Tonsillar Sepsis
Surgical Principle
 Risks and Complications
Risks and Complications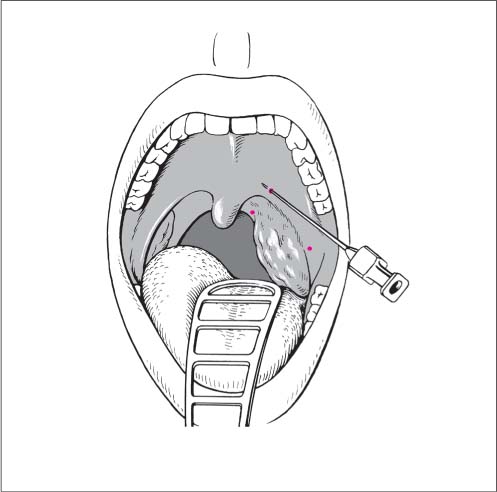
 Risks and Complications
Risks and Complications As for tonsillectomy (see
As for tonsillectomy (see Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


