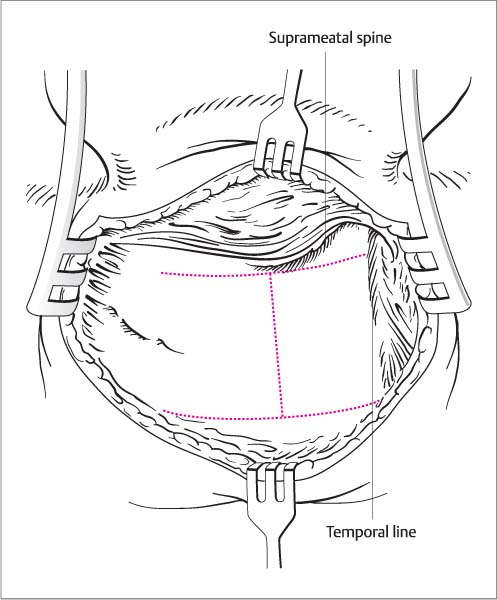
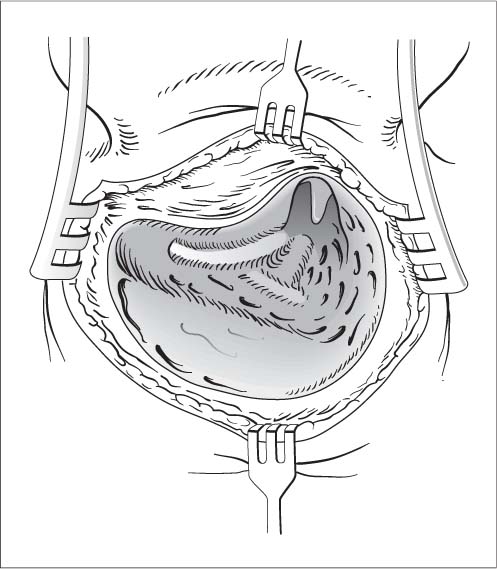
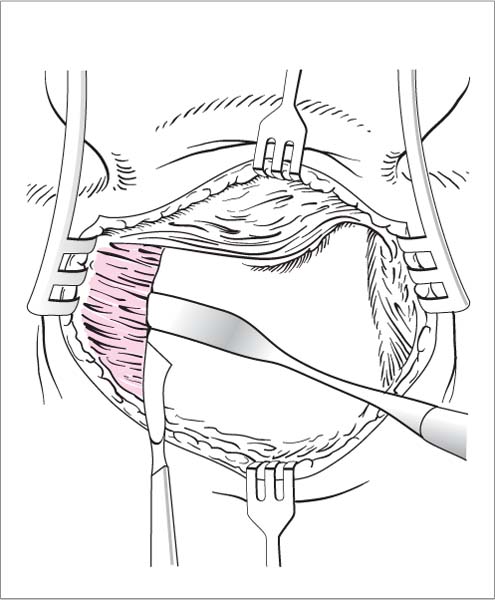
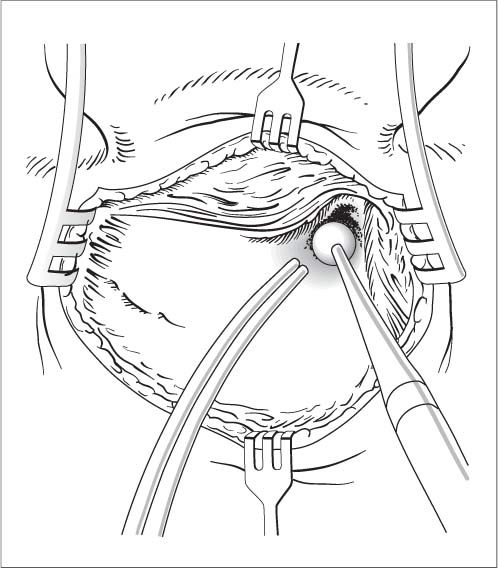
19 Surgery of the Mastoid Process Schüller radiograph, blood count, ESR; high-resolution CT if required. Suction irrigator or combined drilling and irrigation system, antrum hook, House curette. General anesthesia. Local anesthesia is also an option. Positioning. The patient is positioned supine on the operating table with the head turned to the side and immobilized on a headrest or ring. Approach. Postauricular skin incision (see Chapter 17, Fig. 17.4). The incision is extended to the mastoid tip. The entire mastoid process is exposed, and the self-retaining retractors are inserted. Exposure. The periosteum is opened with an H-shaped incision (Fig. 19.1). It is widely reflected from the mastoid cortex with a periosteal elevator from the temporal line to the mastoid tip and from the suprameatal spine to the posterior border of the mastoid. The sternocleidomastoid muscle is released from its insertion with a periosteal knife (Fig. 19.2). Opening the bone. The mastoid cortex is initially opened between the suprameatal spine and temporal line with a large cutting burr, which is applied to the bone in long strokes directed parallel to the temporal line (Fig. 19.3). The boundary of the middle cranial fossa is exposed. The opening is saucerized and deepened with a conical burr. Locating the antrum. The antrum is approached obliquely upward along the base of the middle cranial fossa and the posterosuperior wall of the ear canal using a burr and a curette. The latter instrument is particularly useful in well-pneumatized bone. Identification. The antrum presents as a cavity of variable size and is identified by the bright, shiny, hard bone of the horizontal semicircular canal, which lies behind the short crus of the incus. The antrum must be differentiated from the large surrounding air cells. Orientation is aided by probing with an antrum hook. If a Körner septum (hard, thick bony plate lateral to the antrum) is blocking direct access and limits the depth of the exposure, it should be burred down from the posterior side. Fig. 19.1 Mastoidectomy. The periosteum over the mastoid cortex is opened with an H-shaped incision. Fig. 19.2 Mastoidectomy. The mastoid cortex is exposed. The sternocleidomastoid muscle is released with a periosteal knife. Fig. 19.3 Mastoidectomy. The cortex between the suprameatal spine and temporal line is opened with a large cutting burr. Enlarging the aditus. The aditus ad antrum is enlarged with the House curette and, if necessary, small diamond burrs while scrupulously avoiding any contact between the drill and the ossicular chain. The aditus is enlarged until the incudomalleolar joint is visible in the epitympanum. Mastoidectomy. Next, the air cells are exenterated with a large cutting burr, first working posteriorly into the sinodural angle and Citelli cell and then widely skeletonizing the sinus plate with a large diamond burr while also removing the retrosinus cells (Fig. 19.4). It may also be necessary to drill anteriorly into the zygomatic cells, depending on the indication. The Trautmann triangle located behind the posterior semicircular canal should be exposed as well. The perifacial air cells are opened after removing the cells on the posterior canal wall. This is done only with the diamond burr and curette, working strictly parallel to the course of the facial nerve. When this step has been completed, the mastoid tip is also drilled out. Dura and sinus exposure. If it is suspected that inflammatory changes have spread to the sinus and dura, both structures should be exposed and inspected even in the absence of a visible breach. After the sinus and dura have been skeletonized, the bone covering these structures is thinned further at a circumscribed site, and the thin bony plate is gently broken inward and elevated with a round incision knife. If the dura or sinus has already been exposed spontaneously, granulations will generally be found on the exposed area. The eroded bony margins are extended—thinned with a diamond burr and the remaining shell elevated with an angled round incision knife—until normal dura or sinus wall is encountered. From there the granulations are elevated in the proper plane with the angled round knife and removed with a cup forceps. Additional steps (sinus aspiration, dissection of the dura) may be necessary and are described below under Treatment of Otogenic Complications. Fig. 19.4 Mastoidectomy. The semicircular canal and body of the incus are visible in the antrum and aditus ad antrum. The middle cranial fossa, sigmoid sinus, and facial canal are skeletonized. Concluding the operation. Remaining overhangs are smoothed with a large diamond burr, and all bone dust is carefully removed by irrigation. A drainage tube is inserted and brought out the lower end of the wound. The periosteum is reapproximated with sutures, and the meatal entrance is fixed posteriorly. The wound is closed in layers. The ear canal is packed if it has been opened or mobilized.
Mastoidectomy
Surgical Principle
 The air cells of the mastoid process are exenterated from the mastoid cortex while preserving the posterior wall of the ear canal.
The air cells of the mastoid process are exenterated from the mastoid cortex while preserving the posterior wall of the ear canal.
 The skull base is skeletonized to the middle and posterior cranial fossae, the sigmoid sinus is skeletonized, and sufficient antral patency is established.
The skull base is skeletonized to the middle and posterior cranial fossae, the sigmoid sinus is skeletonized, and sufficient antral patency is established.
Indications
 Mastoiditis and its complications.
Mastoiditis and its complications.
 Cholesteatoma.
Cholesteatoma.
 Cholesterol granuloma.
Cholesterol granuloma.
 Granulating mastoiditis in chronic mesotympanic otitis media.
Granulating mastoiditis in chronic mesotympanic otitis media.
 Chronic otitis media with effusion.
Chronic otitis media with effusion.
 Access for facial nerve decompression, translabyrinthine neurectomy or acoustic neuroma excision, saccotomy, cochlear implant, partially implantable hearing aids.
Access for facial nerve decompression, translabyrinthine neurectomy or acoustic neuroma excision, saccotomy, cochlear implant, partially implantable hearing aids.
Contraindications
 General medical condition (relative).
General medical condition (relative).
 Relative: absence of mastoid pneumatization, complete eburnation, extreme anterior position of the sigmoid sinus.
Relative: absence of mastoid pneumatization, complete eburnation, extreme anterior position of the sigmoid sinus.
Specific Points Regarding Informed Consent
 Deafness, hearing loss due to inner ear pathology or ossicular discontinuity.
Deafness, hearing loss due to inner ear pathology or ossicular discontinuity.
 Tinnitus.
Tinnitus.
 Vertigo.
Vertigo.
 Altered taste sensation (chorda tympani).
Altered taste sensation (chorda tympani).
 Facial nerve injury.
Facial nerve injury.
 Heavy scarring of the incision and auricle, keloid formation.
Heavy scarring of the incision and auricle, keloid formation.
 Neuralgiform pain.
Neuralgiform pain.
 Dural injury with meningitis, brain abscess.
Dural injury with meningitis, brain abscess.
 Sinus injury with hemorrhage.
Sinus injury with hemorrhage.
 Postauricular contraction or fistula formation.
Postauricular contraction or fistula formation.
 Stenosis of the ear canal.
Stenosis of the ear canal.
Surgical Principle
Special Instruments
Anesthesia
Surgical Technique
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 The extent of air-cell removal is variable, depending on the findings. The dura and sinus should always be evaluated, however, when dealing with mastoiditis and its complications. Clinical findings may require exposing the air cells at the root of the zygomatic arch.
The extent of air-cell removal is variable, depending on the findings. The dura and sinus should always be evaluated, however, when dealing with mastoiditis and its complications. Clinical findings may require exposing the air cells at the root of the zygomatic arch.
 Take tissue samples for histology and microbiology.
Take tissue samples for histology and microbiology.
 Establish sufficient antral patency.
Establish sufficient antral patency.
 Use curettes in the vicinity of the ossicular chain; never touch it with a rotating burr.
Use curettes in the vicinity of the ossicular chain; never touch it with a rotating burr.
 A myringotomy or tympanostomy tube may also be necessary, depending on the findings.
A myringotomy or tympanostomy tube may also be necessary, depending on the findings.
 Remove granulations and polyps only under vision and after identifying the malleus head and incus. If bleeding obscures vision, control it by local application of Privine drops or dilute suprarenin solution.
Remove granulations and polyps only under vision and after identifying the malleus head and incus. If bleeding obscures vision, control it by local application of Privine drops or dilute suprarenin solution.
 When skeletonizing the facial nerve with a diamond burr, work strictly parallel to the course of the nerve and only after identifying the horizontal semicircular canal as a landmark.
When skeletonizing the facial nerve with a diamond burr, work strictly parallel to the course of the nerve and only after identifying the horizontal semicircular canal as a landmark.![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine