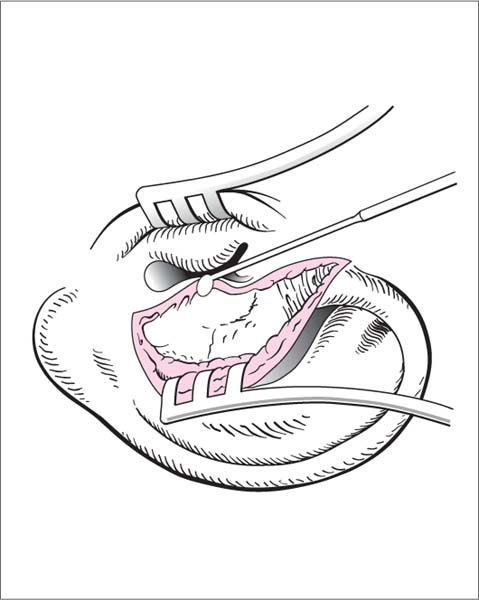
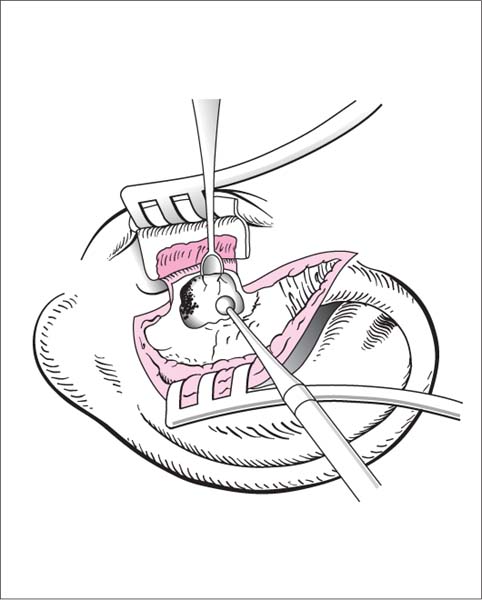
16 Surgery of the Bony Ear Canal and Tympanic Membrane The bony overgrowth is removed until the circumference of the tympanic membrane is fully visible. Auricular malformation (relative). Local or general anesthesia. Fig. 16.1 Removal of exostosis. An endaural incision is made, and the skin over the dome of the exostosis is incised. The incision is extended to form H-shaped flaps. The meatal skin is elevated superiorly and inferiorly with a round incision knife. Fig. 16.2 Removal of exostosis. A large exostosis can be hollowed out with a burr, and the remaining shell can then be fractured with a House curette. The meatal skin is approximated to the anterior wall with a Silastic strip. Perioperative antibiotics. Packing should remain in place for 2–3 weeks. Any granulations that form should be removed. Circumscribed tumors are excised with healthy margins, followed if necessary by coverage of the surgical defect. Superficial benign and malignant tumors of the external ear canal. Local excision is contraindicated for tumors that have infiltrated deeper tissues, invaded surrounding tissues, or cannot be clearly visualized. See Exostosis. Local or general anesthesia.
Exostosis
Surgical Principle
Indication
 Stenosing exostosis with recurrent otitis media.
Stenosing exostosis with recurrent otitis media.
 Direct bone contact with tympanic membrane causing impaired sound conduction.
Direct bone contact with tympanic membrane causing impaired sound conduction.
 Interference with hearing aid fitting.
Interference with hearing aid fitting.
 Restricted access for middle ear surgery or myringoplasty.
Restricted access for middle ear surgery or myringoplasty.
Contraindication
Specific Points Regarding Informed Consent
 Tympanic membrane perforation.
Tympanic membrane perforation.
 Hearing loss, tinnitus.
Hearing loss, tinnitus.
 Facial nerve injury.
Facial nerve injury.
 Stricture due to scarring.
Stricture due to scarring.
 Salivary fistula.
Salivary fistula.
 Temporomandibular joint injury.
Temporomandibular joint injury.
Anesthesia
Surgical Technique
 The patient is positioned supine with the head turned to the side and immobilized on a headrest or ring.
The patient is positioned supine with the head turned to the side and immobilized on a headrest or ring.
 An endaural incision is made and retractors are placed.
An endaural incision is made and retractors are placed.
 An H-shaped skin flap is created over the exostosis. It may be in continuity with the endaural incision if desired.
An H-shaped skin flap is created over the exostosis. It may be in continuity with the endaural incision if desired.
 The meatal skin is separated superiorly and inferiorly from the exostosis with an angled round incision knife (Fig. 16.1). With a very large, broad-based exostosis that almost completely obstructs the ear canal, the skin is mobilized in stages while exposed portions of the exostosis are progressively removed. The superior flap is reflected outward while the inferior flap is retracted away from the drilling site with the suction tip.
The meatal skin is separated superiorly and inferiorly from the exostosis with an angled round incision knife (Fig. 16.1). With a very large, broad-based exostosis that almost completely obstructs the ear canal, the skin is mobilized in stages while exposed portions of the exostosis are progressively removed. The superior flap is reflected outward while the inferior flap is retracted away from the drilling site with the suction tip.
 The bone is removed with a diamond burr using progressively smaller burr diameters. Alternatively, an exostosis with a narrow base can be removed with a gouge.
The bone is removed with a diamond burr using progressively smaller burr diameters. Alternatively, an exostosis with a narrow base can be removed with a gouge.
 Any remaining bony edges can be removed with a House curette (Fig. 16.2).
Any remaining bony edges can be removed with a House curette (Fig. 16.2).
 The meatal skin is reapproximated.
The meatal skin is reapproximated.
 Silicone film and packing are placed into the ear canal.
Silicone film and packing are placed into the ear canal.
 The wound is closed.
The wound is closed.
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 The entire circumference of the tympanic membrane must be visible.
The entire circumference of the tympanic membrane must be visible.
 Do not drill below the level of the tympanic membrane (mainly an issue when excising a posterior wall exostosis).
Do not drill below the level of the tympanic membrane (mainly an issue when excising a posterior wall exostosis).
 Do not drill through the anterior canal wall. The mastoid air cells may be opened but should be covered with meatal epidermis or fascia before closing.
Do not drill through the anterior canal wall. The mastoid air cells may be opened but should be covered with meatal epidermis or fascia before closing.
 With a very large exostosis, it is better to remove and reimplant meatal skin than damage the skin with a burr.
With a very large exostosis, it is better to remove and reimplant meatal skin than damage the skin with a burr.
 Elevated meatal skin can be kept away from the burr with adhesive strips (e. g., Silastic).
Elevated meatal skin can be kept away from the burr with adhesive strips (e. g., Silastic).
 A very large exostosis can be hollowed out and the remaining shell fractured with a House curette (Fig. 16.2).
A very large exostosis can be hollowed out and the remaining shell fractured with a House curette (Fig. 16.2).
 Bony edges projecting over the tympanic annulus can be removed with a House curette, working parallel to the annulus.
Bony edges projecting over the tympanic annulus can be removed with a House curette, working parallel to the annulus.
 Risks and Complications
Risks and Complications
 Wrapping of meatal skin around the spinning burr.
Wrapping of meatal skin around the spinning burr.
 Facial nerve injury (keep above the level of the tympanic membrane).
Facial nerve injury (keep above the level of the tympanic membrane).
 Inner ear damage caused by drilling, accidental contact with the short process of the malleus, ossicular dislocation, tympanic membrane perforation, salivary fistula in the ear canal caused by drilling through the bony anterior canal wall (may also damage the temporomandibular junction), meatal stricture due to extensive skin loss.
Inner ear damage caused by drilling, accidental contact with the short process of the malleus, ossicular dislocation, tympanic membrane perforation, salivary fistula in the ear canal caused by drilling through the bony anterior canal wall (may also damage the temporomandibular junction), meatal stricture due to extensive skin loss.
Postoperative Care
Removal of Small Tumors in the Ear Canal
Surgical Principle
Indications
Contraindications
Specific Points Regarding Informed Consent
Anesthesia
Surgical Technique
 The patient is positioned supine with the head turned to the side and immobilized on a headrest or ring.
The patient is positioned supine with the head turned to the side and immobilized on a headrest or ring.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


