Chapter 115 Surgery for Pediatric Vitreoretinal Disorders
General aspects
Development of the child’s eye and surgical consequences
The development of spatial vision and binocular fusion (sensitive period) starts in the human infant at the age of 3–4 months.1 A reduction in the visual acuity of one or both eyes with morphologic intactness is called amblyopia. The child’s age at exposure to an amblyopia-inducing condition is the most important determinant for its development. Children up to 8 years can develop an amblyopia; development at later age is rare. The therapy of choice for all forms of amblyopia is an appropriate occlusion therapy which sometimes must be continued until the child is 12 or 13 years old in order to avoid a recurrence.
Untreated anisometropia resulting from vitreoretinal operations induces amblyopia, especially in small children (Table 115.1). Whereas a refractive error averaging −2.75 diopters (D) is induced by a cerclage in the adult,3 the anisomyopia resulting from a cerclage may be greater in pediatric eyes. Myopia occurs as a result of the axial elongation induced by the encircling band which has a more pronounced effect on refraction due to the very short axial length of the infant eye. Furthermore, buckling surgery with a cerclage induces forward displacement of the lens, which causes severe myopia in the infant lens with its relatively high refractivity.4 The refractive change is generally less than 6 D and amblyopia is rarely manifest, since patients still have sharp near vision.5 These patients can generally be fitted with spectacles. High axial myopia of −11 to −15 D following buckling surgery in infants with retinopathy of prematurity (ROP) is more difficult to treat. Therefore, once successful reattachment of the retina has been achieved, the cerclage can be severed thus reducing the refractive error to values around −5 D.4
Table 115.1 Deprivation caused by vitreoretinal disease2
| Stimulus deprivation | Stimulus deprivation and suppression | |
|---|---|---|
| Bilateral deprivation: amblyopia due to media opacity of the same severity, e.g., bilateral congenital cataract or bilateral vitreous hemorrhage | 1. | All predominantly unilateral stimulus deprivations or bilaterally differing stimulus deprivations |
| 2. | Relative amblyopia: congenital or early manifestation of defects in the foveal region | |
| 3. | Uncorrected anisometropia because of blurred image and aniseikonia (e.g., anisomyopia due to cerclage anisohyperopia in silicone oil tamponade, cycloplegic eye drops) | |
| 4. | Acquired medium opacity | |
The most obvious and important anatomic consideration in pediatric retinal surgery is the relatively smaller size of the child’s globe and orbit compared with that of the adult (Table 115.2). At birth, the average axial eye length is 17.5 mm; which is 70% of the axial length of an adult eye. In the first year, the eyeball length increases by nearly 3.5 mm. From age 3–14, the eye grows very slowly; an average of 0.1 mm/year.6 The average horizontal and vertical corneal diameters are 9.8 ± 0.33/10.4 ± 0.35 mm (newborn boys) and 10.1 ± 0.33/10.7 ± 0.29 mm (newborn girls). By age 7, the cornea has an average diameter of 11.7 mm.7 In the newborn, the anterior segment already comprises 80% of its final area, while the surface of the posterior segment comprises only 20% of an adult eye; in the first 6 months of life, the posterior segment surface increases by 50%. The lens of the newborn is spherical and is relatively thicker than the adult lens. As the lens flattens, the power of the lens is reduced by approximately 8 D; in the first 2 years, it is reduced by approximately 11.5 D and it reaches adult values between 7 and 10 years.8 Since the cornea flattens, its power is also reduced: in the first 6 weeks of life, the power is reduced from 51 D to 44 D.9
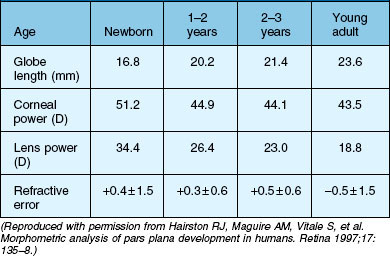
A vision-dependent feedback mechanism is necessary for the development of emmetropia.10 It is assumed that various forms of stimulus deprivation induces a myopic shift during development.11 Dense hemorrhages persisting in the neonatal vitreous for 4 weeks or longer appear to cause axial myopia and severe amblyopia. Surgical intervention before this time should be considered to avert deprivation amblyopia and to retard axial myopia.12
The ciliary body of the eye is divided into the pars plicata ciliaris and the pars plana ciliaris. The pars plicata of the mature newborn is nearly adult in size, whilst the pars plana is relatively small (Table 115.3).13,14 The pars plana of mature newborns measures 1.6–2.0 mm.6
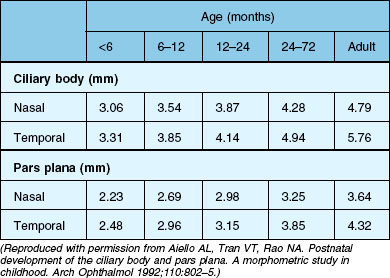
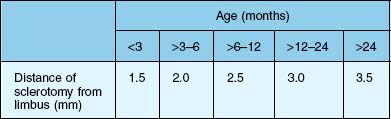
The anterior–posterior extension of the pars plana begins in the postnatal phase (Fig. 115.1). In a 6-month-old infant, the pars plana is >3.0 mm6,14 this means that in infants younger than 6 months, the pars plana width is <3.0 mm. However, the extension of the entire ciliary body is quite variable in individual eyes, its total extension in the age group 24–72 months ranges from 3.75 mm to 5.5 mm. A total of 75% of the final length of the ciliary body at adulthood is reached by 24 months.14 A positive correlation between the anteroposterior diameter of the eye and the distance from the sclerocorneal limbus to the ora serrata was demonstrated in the four meridians.13
The results of the morphometric investigations are of great importance for the choice of the vitreoretinal–surgical entrance. The anterior–posterior expansion of the ciliary body corresponds approximately to the distance from the corneoscleral limbus measured externally (in millimeters). For an accurate external determination of the location of the ora serrata, 0.3–0.4 mm must be added to the measured distance starting from the corneoscleral limbus for the values of the ciliary body extension.14 Accordingly, in infants, one must select a pars plicata entrance for a vitrectomy. Only then is it ensured that the retina is not artificially damaged. The disadvantage of this entrance is the direct proximity of the lens and therefore manipulations and lens-saving operations are often not possible. Because of the relatively larger size of the lens in relation to the anterior segment in children compared with adults, special care is required if the eye is operated on without removing the lens. For a standard three-port vitrectomy, the width of the pars plana should be at least 3 mm,6 so that at the earliest a pars plan a approach can be selected for a 1-year-old child. The measurements mentioned here are based exclusively on histological slides, i.e., after appropriate fixation of the material. The real dimensions are therefore larger.
Scleral thickness is clearly age-dependent. During the first half-year of life the average scleral thickness is approximately 0.4 mm, by age two, the thickness has doubled. After that age, the scleral thickness increases very slowly and becomes stiffer with age.15
The vitreous body is avascular, transparent, and gel-like in consistency, and comprises 80% of the eyeball volume. The vitreous body is attached to the surrounding structures; a firm attachment exists within the area of the vitreous base and Wieger’s ligament forms the firm attachment between the soft lens and anterior vitreous. One differentiates between the anterior and posterior vitreous body. The posterior vitreous cortex (posterior vitreous hyaloid) is 100–110 µm thick and consists of closely packed collagen fibrils. In pediatric eyes the posterior vitreous cortex lies adjacent to the retinal surface. This structure is known as the vitreoretinal border region, the vitreoretinal junction, or the vitreoretinal interface. The vitreoretinal interface consists of the internal limiting membrane (ILM) and the posterior hyaloid. In the newborn, the vitreous body appears homogeneous with a fine radial stripe pattern. It is interspersed with so-called transvitreal channels. With increasing age vitreous strands develop, which in the adult eye form typical concentrically arranged diaphragm-like condensations.16 The secondary vitreous in the term infant without ocular disease consists of a very dense collagenous gel. Some authors believe that in term infants, there is no hyaluronic acid present until 4 years of age. There are, however, many diseases that are associated with a lack of densely formed vitreous (e.g., myopia, retinitis pigmentosa, ROP, familial exudative vitreoretinopathy (FEVR), Goldmann–Favre disease, and congenital retinoschisis). In pediatric eyes, the attachment between the vitreous cortex and retina is very firm. Formed vitreous and increased scarring seem to be correlated. It is believed that children develop proliferative vitreoretinopathy (PVR) more frequently than adults.
Surgical considerations and techniques
Cornea and keratoprosthesis
The placement of a temporary keratoprosthesis (e.g. Eckhardt keratoprosthesis (DORC) or Landers keratoprosthesis (Ocular instruments) allows a clear view for vitreoretinal surgery, which is then followed by a corneal transplant. Several retrospective studies have documented acceptable outcomes with combined surgery in adults, but only a few cases with children have been well documented.17–19 The best outcome was of a 7-year-old boy whose operation included usage of a keratoprosthesis followed by lentectomy, scleral buckling, vitrectomy, C3F8-fluid/gas-exchange, and penetrating keratoplasty. At 10 months postoperatively, the best corrected visual acuity was 20/30.17 In summary, 10 of 17 corneal grafts in children remained clear in the follow-up period, but in 16 eyes, visual acuity did not exceed finger counting. Phthisis occurred in about 40%.17–19
In general, the prognosis of keratoplasty in children is poorer than in adults. There is a greater risk of an immune reaction with development of neovascularization. Perforating keratoplasties in children following trauma have a poorer general prognosis, especially in cases of aphakia and after injuries involving the posterior segment of the eye as opposed to phakic eyes and after isolated injuries to the anterior segment. In a meta analysis,20 55–100% of transplants were not opaque 1 year after keratoplasty in children.
The corneal sutures in children can be removed much sooner than in adults. Removal should be performed within the time intervals specified in Table 115.4, in order to enable immediate provision of contact lenses, especially in aphakic eyes.21
Table 115.4 Recommendation for removal of corneal suture by age
| Age | Removal of corneal suture |
|---|---|
| 1–6 months | 4–6 weeks |
| 6–12 months | 6–8 weeks |
| 12–24 months | 8–12 weeks |
| 24–48 months | 12–16 weeks |
| 5–15 years | 4–6 months |
(Reproduced with permission from Reidy JJ. Penetrating keratoplasty in infancy and early childhood. Curr Opin Ophthalmol 2001;12:258–61.)
Lens management
In some cases, especially in eyes with a high risk of developing proliferative vitreoretinopathy, such as after severe open globe injury and in uveitis, an intraocular lens (IOL) should not be implanted. Opacity of the remaining capsule fragments with optically disadvantageous postcataract membranes is inevitable. In addition, remnants of the lens capsule and the zonular fibers lead to development of synechiae with distortion of the pupil which is associated with a reduction in the visibility of the peripheral retina. Surgical treatment of retinal detachment is impeded. For this reason, complete removal of the entire lens, including the complete capsule should be aimed for in eyes with a high risk of developing PVR. In addition, a current study shows a significantly increased endophthalmitis risk if an intraocular lens implanted placed in eye immediately after open globe injury.22
The risk of a severe intraocular fibrin reaction is one of the further drawbacks of intraocular lens implantation in children. Even after operation of a nontraumatic cataract in a pediatric eye, a significantly less pronounced fibrin reaction is observed after pars plana lentectomy than with a limbal approach, as necessary for implantation of an intraocular lens.23,24 In darkly pigmented eyes, an even more intense fibrin reaction is observed. Further disadvantages of primary intraocular lens implantation are the imprecise biometry and unclear prognosis concerning eye growth.
Posterior-segment surgical techniques
The smaller size of infant eyes results in differences in surgical landmarks, relative instrument size, and fluid dynamics of vitreous surgery (Fig. 115.2) in addition to increased vitreous adhesion. We will address these specific issues below.
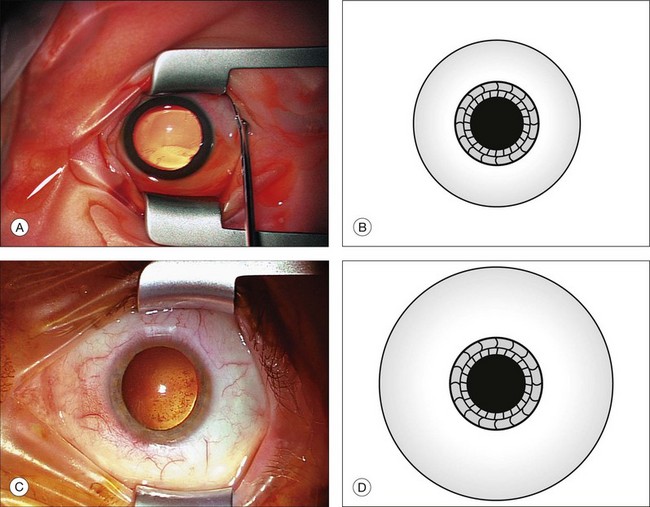
Fig. 115.2 Comparison of a globe from a neonate (A,B) with that of an adult (C,D) shows different proportions.
Buckling surgery (see also Chapter 100, Techniques of scleral buckling): after a peritomy, traction sutures (silk 5/0) are placed beneath the insertion of two to four rectus muscles. Then the retinal holes are located, marked, and a transscleral cryoretinopexy is performed under ophthalmoscopic control. Depending on location of the hole, appropriate radial or circumferential scleral buckles are placed and fixed, if necessary with an additional segmental silicone-rubber sponge. For a cerclage, one suture per quadrant is placed, and the ends are secured with a sleeve. Due to spatial considerations, the sleeve is preferably placed in the lower temporal quadrant. The perfusion of the central retinal artery must be checked. Rarely, a paracentesis is necessary. The scleral thickness is thinner than in adult eyes, therefore thinner (6/0) suture (polyester fiber, polyamide fiber) should be used for partial-thickness scleral sutures in babies. We also recommend the use of flat spatula needles (0.28 mm diameter).
A child’s eyes are more prone to vigorous reproliferation than those of adult. This can be attributed to biochemistry of this age group which support cell growth more actively, or to a longer delay between the time of detachment and the establishing of diagnosis and therapy. For primary detachments, we use a sculpted 3 × 5 mm sponge with an encircling 2.5 mm solid silicone band. It is often assumed that the children’s orbits cannot accommodate a large sponge, but this type of exoplant is well tolerated. Drainage of subretinal fluid is controversial. Postoperative complications of scleral buckling in children range from refractive amblyopia to alteration of eye growth. To avoid these complications, the band is cut in all children younger than 3 years, approximately 3 months after the scleral buckling operation, once a stable reattachment has been achieved.4 We choose to cut rather than to remove the element because we believe that continued support is given to the retina by the encapsulated exoplant. To reduce amblyopia development in the postoperative period, we prescribe 1% atropine drops for 5 days; if both eyes have good visual potential, we prescribe the drops for both eyes. In addition to amblyopia therapy, a refractive error needs to be treated with adequate prescriptions.
Usually a three-port vitrectomy is performed in children. The infusion is preferably placed temporally. The sclerotomies are placed 3.5 mm behind the limbus in infants older than 2 years. In children younger than 2 years, the sclerotomies are performed within the range of the pars plicata and/or pars plana, in accordance with Table 115.5. In the infant eye, especially in babies, the scleral incisions are made posterior to the limbus with incisions through the pars plicata. Displacement of the conjunctiva for adequate coverage of the sclerotomies necessary for transconjunctival sutureless surgery is not possible.25 Therefore, conjunctival dissection is thus preferred before the sclerotomy incisions are made. Because of the very thin sclera in babies and infants, we recommend using trocars beginning at age two. In preschool children, we recommend placing the trocars perpendicular through the sclera. In young eyes, oblique placement of the trocars is associated with an increased risk of accidental dislocation, since the trocars have only a short path through the pediatric sclera compared to the longer path through an adult sclera. A young patient age is a risk factor for intraoperative sclerotomy leakage: in a study of 322 eyes, 61% of patients aged <40 years needed intraoperative suture placement for leaking sclerotomies at the end of 23G transscleral vitrectomy.26 Due to the decreased scleral stiffness and the increased elasticity of young sclera, suturing of sclerotomies in children is necessary to ensure a leakproof closure. For the closure of the conjunctiva, absorbable Vicryl 10/0 can be used.
A complete range of small incision instruments which permit a complete vitrectomy through small (23G and 25G) incisions has been developed. Performing surgical maneuvers with smaller instruments allows the surgeon to work more precisely and increases the potential for minimizing surgical trauma. We prefer the use of 23G instruments, but case selection remains important. In case of very dense cellular membranes, the 23G or 25G cutter cannot adequately address this tissue and additional instrumentation may be necessary. In more complicated cases, such as traction retinal detachments, eyes with extensive fibrovascular proliferation, complex retinal detachments requiring scleral buckles for proliferative vitreoretinopathy, and giant retinal tears, surgical maneuvers can be performed with small gauge instruments, but are often more easily performed using 20G instrumentation.27 For cases requiring enhanced panoramic illumination, it is possible to use the 20G shielded bullet light pipe instead of the 23G illumination light pipe. The sclerotomies are made with a 23-MVR blade. In babies, we use a 23G disposable Tornambe infusion cannula (DORC 1272). Larger sclerotomies may allow for better manipulation of the 23G or 25G cutter within the sclerotomy, avoiding unintentional bending of the instrument and potential damage to the lens or retina.25
Vitrectomies are always performed with wide-angle observation systems. In addition, wide-field vitrectomy contact lenses are specifically designed to facilitate pediatric vitreoretinal surgery.28
The wide-angle observation systems for vitreous surgery (binocular indirect ophthalmomicroscope, vitreopanfundoscope, and stereoscopic diagonal inverter have many advantages: (1) wide angle of view; (2) large depth of field; (3) stereopsis; (4) good visualization in hazy media, even with narrow pupil; (5) upright, tru-to-side image; (6) magnification with the microscope zoom; (7) beam splitter for the assistant; (8) good visualization in gas-filled or silicone-filled eyes; (9) free mobility of the eye for peripheral surgery. With these systems, surgery is possible from the posterior pole to the vitreous base and the anterior loop traction, regardless of whether the eye is phakic, pseudophakic, or aphakic. The vitreous body can be removed with a 23G high-speed cutter with a cutting rate of 5000 revolutions/minute and a suction power of 400 mmHg. With the cutter near the peripapillary retina, suction should be applied to separate the posterior hyaloid from the retina in slow circular movements. Special attention is necessary to create a posterior vitreous detachment; “tenting of the retina” is a sign of very strong vitreoretinal adherence and poses a high risk for development of iatrogenic retinal holes. A compromise is a judicious core vitrectomy, leaving as thin a layer of cortical vitreous on the retina as possible. If it is not possible to remove vitreous in the periphery, a thorough shaving is necessary. This can be performed by a small gauge high-speed cutter; if 20G instruments are used, special 20G shaver-cutters are available. Creation of a posterior vitreous detachment with suction alone to lift the vitreous off of the optic nerve is more difficult with small gauge vitrectomy probes. The smaller port opening decreases the ability to engage and hold the vitreous. Creating a posterior vitreous detachment in a child with adherent posterior hyaloid remains substantially easier with 20G instruments because of larger port sizes and greater flow rates.27 For small-gauge vitrectomies, higher infusion rate in the range of 35–50 mmHg are necessary to ensure adequate intraocular fluid dynamics. Due to the lower systolic blood pressure of babies and infants, iatrogenic occlusion of the central retinal artery can be induced, and the surgeon has to observe the optic nerve.29 Retinal breaks should be avoided because they are often difficult to treat. Posterior drainage retinotomies are associated with profound postoperative proliferation. Iatrogenic breaks are best avoided by abandoning peeling in favor of bimanual dissection with forceps and scissors. If a retinotomy is unavoidable, it must be performed as close as possible to the ora serrata and following diathermy coagulation. Retinopexy of retinotomy edges is done with argon laser coagulation. If the extension of the retinotomy is larger than 2 clock-hours, a silicone oil tamponade is used. Diagnostic vitrectomy can be used to evaluate conditions such as inflammatory conditions, and amyloidosis. The cytopathologic analysis of ocular fluids obtained for diagnostic purposes has proven to be effective for establishing and confirming diagnosis.
It is hoped that pharmacologic agents will become available to assist in separating the youthful posterior cortical vitreous from the retina. The goals of enzymatic vitrectomy (dispase, plasmin, tissue plasminogen activator, or chondroitinase) are either to disinsert the posterior hyaloid from the retinal surface in an atraumatic, precise, cleavage plane or to try to disinsert the peripheral vitreous from the neurosensory retina. Enzymatic (collagenase or hyaluronidase) manipulation of the central vitreous in terms of liquefaction has been evaluated. At present microplasmin is used in clinical studies.30–32 This is certainly only the beginning of this type of vitreal surgery, whether adjuvant or alternative.
Silicone oil and gas tamponade
The physical properties of silicone oil include a combination of specific gravity, refractive index, and surface tension. Heavy silicone oil may be of interest for inferior traumatic retinal detachments. Use of 1000 cs or 5000 cs silicone oil can be considered in the management of pediatric complex retinal detachments associated with multiple etiologies.33 The choice of viscosity offers an optimal balance between easy injection and a longtime tamponade. Indications and the long-term results of pars plana vitrectomy in children are comparable with those in the adult. Retinal reattachment and preserved visual acuity can be achieved in the majority of eyes using silicone oil retinal tamponade. In complicated retinal detachments, especially after injuries, a radical approach with primary silicone oil injection and later silicone oil removal has proved useful. In children, with their long life expectancy, timely removal of silicone oil vital for maintaining the function of the eye.
Biostaining of the ILM and intraocular membranes is a technique that is still evolving, and despite good results in adults, it should be used in children with utmost care. We recommend Trypan blue and Brilliant blue as “safe” dyes for staining, assuming they have nontoxic or at least minimal toxic effects.34 Visualization of the stained posterior hyaloid greatly facilitates complete removal and reduces surgical time. Control staining following membrane removal is possible, preferable by the use of triamcinolone to check if all membranes have been successfully removed.
Indications for surgery
Injuries
(See also Chapter 98, Pathophysiology of ocular trauma, and Chapter 100, Techniques of scleral buckling.)
Direct injury
Open globe injury
Some 29–47% of pediatric open globe injuries involve both the anterior and posterior segments of the eye.35–37 Whereas the primary surgery includes external reconstruction of the globe, internal reconstruction can be performed simultaneously with the primary wound closure or, in most cases, in a second step.
The timing of secondary comprehensive anatomical internal reconstruction is crucial. Various authors have recommended a secondary vitreoretinal operation for internal reconstruction in the period between the 7th and 10th post-traumatic day in adults38–40; others recommend 3–10 days after trauma.39,41 The general rule is to delay comprehensive anatomical reconstruction of the seriously injured eye for approximately 1 week, when the risk of intraoperative hemorrhage is dramatically reduced and a separation of the posterior vitreous begins to develop.38,39 Kuhn et al. recommend early vitrectomy within 3 days to prevent development of vitreoretinal proliferation.39
The value of a prophylactic encircling band in severe globe-opening injuries is controversial. There are no prospective studies documenting the advantage in children. In adults, the frequency of retinal detachment is less on the whole after applying an encircling band. An encircling buckle procedure is recommended in the presence of a corneoscleral or scleral wound >5 mm with ciliary body involvement with marked vitreous loss and vitreous hemorrhage.42–44 Despite optimal follow-up, the functional results after combined pediatric anterior and posterior segment injuries are limited: about 12%33 to 69%37 of the children attain a visual acuity of 0.1 or better after primary wound closure and secondary surgery for reconstruction of the anterior and posterior segments.
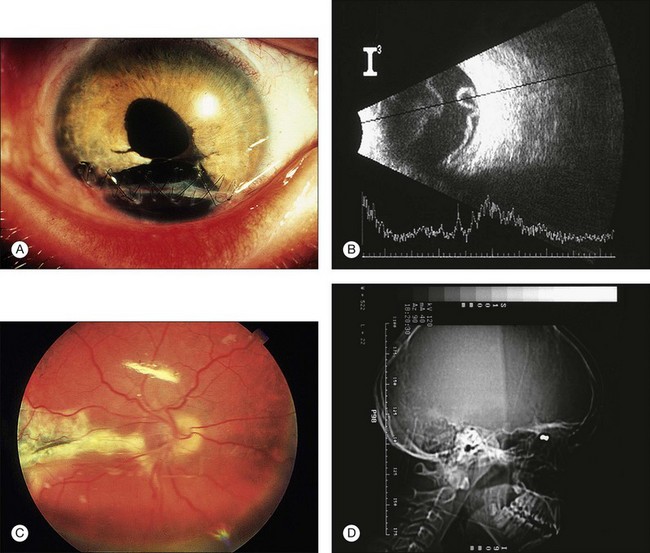
In addition, children may develop more extensive postoperative inflammation, scarring, and severe proliferative vitreoretinopathy than adults, which may also affect the anatomical and functional outcomes.45 The results after pediatric vitreoretinal surgery depend greatly on the extent and severity of the primary damage (Fig. 115.3). A wound size exceeding 10 mm, a lens lesion, and a patient age under 4 years are factors with unfavorable prognoses. Further negative influential factors include: severe intravitreal bleeding, poor initial vision, and gunshot injuries. Retinal detachment always correlates with significantly poorer results. Preoperative macular attachment is a crucial prognostic factor for attaining a postoperative vision better than 0.1.46,47
Closed globe injury
Oradialysis
A common finding in closed injuries is an oradialysis. An oradialysis is located most often inferotemporally, which may only become symptomatic years after the trauma. In the absence of cataract, minimal vitreous haemorrhage or haze, treatment consists of a circumferential segmental buckle. The edge of the segmental buckle should exceed the edge of the dialysis by twice.48 Anatomical reattachment was achieved in 67–88% of cases, whereas the rate of PVR was low.49,50
Traumatic macular hole
Most traumatic macular holes result from closed-globe contusion injuries. Furthermore, the formation of a macular hole secondary to a penetrating injury has been documented in an 8-year-old boy.51
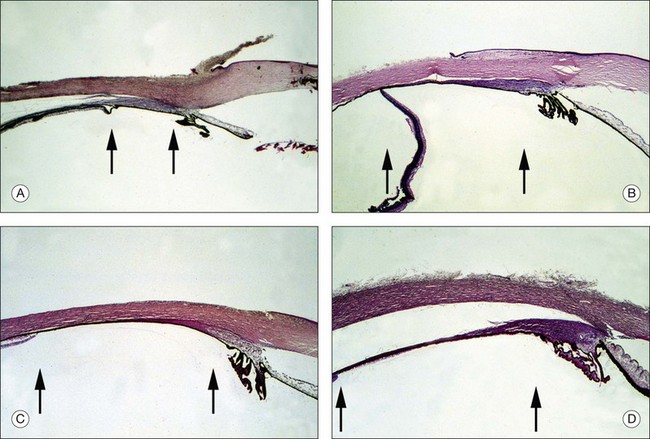
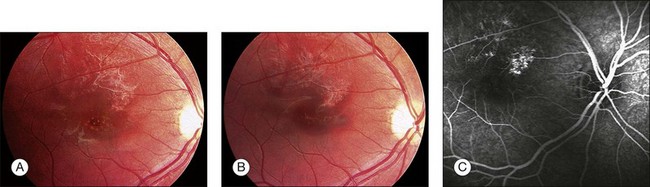
Traumatic macular holes may result from blunt trauma when it causes separation of the vitreous from the retina, contusion necrosis, or subfoveal hemorrhage. The cause of visual deterioration is necrosis resulting from contrecoup forces or tearing of the retina by a sudden separation of the posterior vitreous face.52 But others found that the posterior vitreous was detached from the macula in only 5% of eyes with traumatic macular holes.53 They supported the theory that rupture of the macula caused by retinal stretching occurs as a result of either ocular deformity in the equatorial region or from the strong force of impact on the macula.53 Small, full-thickness traumatic macular holes with a size of 0.1–0.2 disc diameter (DD), can resolve spontaneously in 64–100% of pediatric cases, 3–4 months following trauma, and this may be associated with good visual recovery, in most cases even 20/20.54–56 In contrast to spontaneous closure of small macular holes (100–200 µm) closure of large holes (400–600 µm) has been rarely described (Fig. 115.4).57
In preschool children, the timing of surgery should be based on the fact that traumatic macular holes may be amblyogenic. We therefore recommend vitreous surgery for the treatment of traumatic macular hole after 4 weeks. In elderly children, a period of observation of 3–4 months before vitreoretinal surgery is recommended.55
Common features of patients with spontaneous closure of traumatic macular hole are young age (<25 years), small size of the macular hole (0.1–0.2 DD), no posterior vitreous detachment, and no epiretinal membrane.55
Vitreous surgery for traumatic macular holes can lead to anatomic success in 92–100% and visual acuity improvement in 92–100% of pediatric patients.51,55,58 Recent studies recommend surgical procedures including removal of the posterior hyaloid, the epiretinal membrane, and internal limiting membrane and expanding gas/air mixture tamponade.55,58,59 Studies with adjunctive treatments have been published and describe the successful use of platelet concentrate,60 and plasmin (0.4 IU of autologous plasmin) for enzyme-assisted pars plana vitrectomy.58 In young patients, poor compliance with face-down positioning may be a factor in surgical failure. It is difficult for a child to maintain a face-down position postoperatively, therefore the use of silicone oil is advocated in children who need long-term intraocular tamponade after vitreoretinal surgery. However, additional surgery for silicone oil removal is necessary.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


