Chapter 31 Surgery for Cochlear Implantation
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
There have been remarkable advances in cochlear implantation. Although the first attempt to stimulate the auditory system electrically occurred nearly 2 centuries ago, the development of a cochlear prosthesis to restore hearing to patients with sensorineural hearing loss has happened only over the past 5 decades. The early pioneering work of Simmons, Michaelson, and House provided the stimulus to encourage others, including Bonfai, Chouard, Clark, Eddington, and the Hochmairs.1 The initial acceptance of cochlear implants was slow; safety and efficacy were the concerns of the early investigators, and the greatest champions of the implant were the patients themselves. Time and technology have increased the benefits gained by most patients from their cochlear implants. As a result, cochlear implants have become the most successful prosthesis ever used to attempt to restore a sensory deficit.
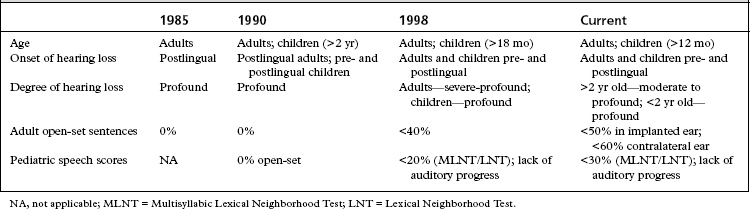
Incremental improvements in technology have resulted in the approval of multiple devices over the years. As performance with cochlear implants has improved over the years, the criteria for cochlear implantation have expanded (Table 31-1). In more challenging situations, bilateral cochlear implantation has been shown to provide additional benefit beyond a single cochlear implant, and is now considered an accepted medical practice outside of research protocols.2 Prospective studies continue to examine the benefits of bilateral cochlear implantation in adults and children.
MEDICAL EVALUATION
Two crucial factors influencing auditory performance after cochlear implantation include age of onset of deafness and duration of profound hearing loss. The ideal adult candidate has profound acquired sensorineural hearing loss. A period of auditory experience adequate for development of normal speech, speech perception, and language offers a significant advantage in learning to use the implant. These postlingually deafened patients represent most adults undergoing cochlear implantation. In these patients, there is a significant correlation between duration of profound hearing loss and performance.3 Patients with prolonged auditory deprivation receive similar auditory information as do other implant patients, but are unable to use the information as effectively; this is thought to be due to the loss of central auditory processing. A few adult implant recipients are congenitally or prelingually deafened, with prolonged auditory deprivation and little to no experience with sound. These patients typically have greater difficulty assimilating the new auditory information, and generally have performed less well than patients with some degree of auditory memory.
Physical Examination
It is important to identify preoperatively any external or middle ear diseases, including perforations of the tympanic membrane, that must be treated before cochlear implantation. For young children, the size of the implant in relation to the size of the child’s skull must be evaluated, and issues involved with skull maturation must be considered. The distance between the cochlear promontory and the mastoid cortex, the approximate sites of the electrode array, and the receiver-stimulator increases about 1.7 cm from birth to adulthood, with one half of the increase occurring during the first 2 years of life.4 The electrodes must be long enough to tolerate the increase in height and width of the skull that occurs with the child’s growth. The accommodation occurs through the gradual straightening of the excess electrode length within the air-containing mastoid cavity.5
Imaging
Preoperative imaging completes the candidacy evaluation process and assists in surgical planning. Choice of imaging modality varies at individual implant centers. High-resolution computed tomography (CT) scanning of the temporal bone and magnetic resonance imaging (MRI) are currently used. CT scanning provides excellent detail of inner ear morphology, the course of the intratemporal facial nerve, and aeration of the mastoid. Limitations of CT include the inability to evaluate retrocochlear pathology and cochlear patency in patients with fibrosis of the cochlea as a precursor to cochlear ossification. The ability to detect an absent cochlear nerve also is limited. MRI addresses these limitations,6 but this imaging modality incurs additional expense and may require general anesthesia in young patients.
Complete agenesis of the cochlea and an abnormal acoustic nerve resulting from congenital malformation, trauma, or surgery are contraindications for cochlear implant placement.7 Cochlear hypoplasia (present in Mondini’s deformity) is not a contraindication for cochlear implantation. Adults and children with incomplete congenital cochlear malformations have received implants successfully.8 Ossification or fibrous occlusion of the cochlea or the round window does not exclude a patient from implantation, but it may influence outcome. Occlusion of the cochlea may lead to partial insertion of the electrode carrier. MRI has become more useful than CT in the evaluation of the membranous inner ear in detecting cochlear fibrosis.
Promontory Evaluation
A few implant teams perform an electric stimulation test at either the promontory or the round window membrane.9 A positive response is a perception of sound on stimulation. Some investigators do not believe that such testing is crucial in the selection of candidates because patients with a negative response, particularly at the promontory, may respond to intracochlear stimulation with an implant. Promontory stimulation may be helpful in cases of suspected cochlear nerve agenesis.
SURGICAL TECHNIQUE
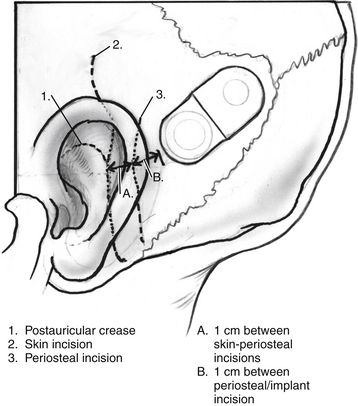
Surgery is performed with the patient under general anesthesia with the use of continuous intraoperative facial nerve monitoring. Perioperative antibiotics are routinely administered before making the initial incision. Many different incisions have been designed to allow placement of the receiver-stimulator (Fig. 31-1). Generally, the skin flap must be large enough to cover the receiver-stimulator completely. The length of the incision and size of the skin flap have been reduced over the years. By reducing incision and flap size, there is less interruption of the vascular supply to the operative field; this seems to correlate with fewer wound and flap complications. Skin and periosteal incisions should overlap by at least 1 cm; the skin incision should be at least 1 cm anterior to the front edge of the receiver-stimulator (Fig. 31-5).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


