Surface Ablation: Photorefractive Keratectomy, LASEK, Epi-LASIK, and Epi-LASEK
Sumit (Sam) Garg
Ann Z. McColgin
Roger F. Steinert
The development of excimer laser ablation represented a breakthrough in the correction of ametropia. Photorefractive keratectomy (PRK) uses a 193-nm argon fluoride excimer laser to ablate the anterior corneal stroma to a new radius of curvature to decrease refractive error. In the early 1990s, PRK became a common technique worldwide for treating low to moderate myopia because it offers a wider treatment range and more predictable and stable results than incisional keratotomy,1,2,3 PRK has been the subject of extensive investigations, with ongoing improvements in hardware and technique. Laser in situ keratomileusis (LASIK) uses PRK technology but performs the procedure under a lamellar flap formed with a microkeratome or femtosecond laser. LASIK is discussed in detail in the next chapter. In this section we review the background, preoperative evaluation, surgical technique, clinical results, and complications of PRK and its more recent variants, LASEK, Epi-LASIK, and Epi-LASEK. The current techniques for these surface treatments are sometimes collectively termed advanced surface ablation (ASA).
BACKGROUND
Trokel et al4 and Srinivasan5 demonstrated a new form of laser–tissue interaction, termed photoablation, in 1983. Srinivasan, an IBM engineer, was studying the far-ultraviolet (UV; 193 nm) argon fluoride excimer (a contraction of “excited dimer,” the photochemical process that emits the laser photons) laser for photoetching of computer chips when Trokel, an ophthalmologist, postulated and subsequently proved that a similar process could also remove corneal tissue discretely and precisely with minimal damage to the adjacent cornea. The original observation of the effect of ultrashort UV light on the cornea is attributed to a civilian contractor, John Taboada, who was studying potential laser toxicity for the military. Trokel rapidly recognized the potential of the excimer laser for refractive and therapeutic corneal surgery.
Photoablation occurs because the cornea has an extremely high absorption coefficient at 193 nm. A single 193-nm photon has sufficient energy to directly break the carbon–carbon and carbon–nitrogen bonds that form the peptide backbone of the corneal collagen molecules. Consequently, excimer laser radiation ruptures the collagen polymer into small fragments, and a discrete volume of corneal tissue is expelled from the surface with each pulse of the laser.6,7,8
Initially, investigators studied whether the excimer laser could be used as a “laser scalpel” for corneal surgery in procedures such as astigmatic and radial keratotomy (Fig. 48-1).9,10 However, the excimer laser is a poor replacement for a cutting scalpel because the laser removes tissue, creating a “kerf”—it does not incise the tissue.11
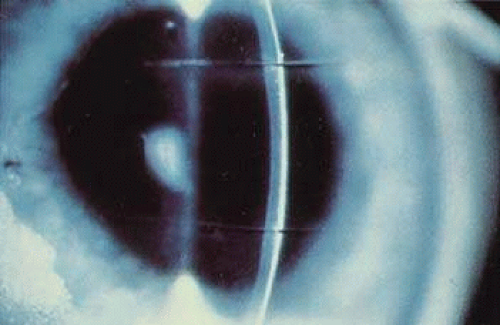 Figure 48-1. Two linear deep incisions created by the excimer laser in an ex vivo human cornea. |
The more successful application of the excimer laser for correcting ametropia is the sculpting or reshaping of the outer de-epithelialized surface of the cornea to alter its refractive power. This surgical procedure, termed photorefractive keratectomy (PRK) by Marshall and Trokel, was the focus of extensive preclinical investigations before it was applied to sighted human eyes.12,13,14,15,16 The results of early animal studies provided evidence for normal wound healing in laser-ablated corneas,17,18,19,20,21,22 and as the laser and delivery system technology matured,23,24,25,26 confidence grew that sighted ametropic human eyes could successfully undergo PRK. McDonald et al27 treated the first sighted human eye in 1988, and now millions of PRK procedures have been performed worldwide. The popularity of PRK faded rapidly when LASIK was popularized in the late 1990s, primarily because LASIK offered a faster visual recovery and less postoperative discomfort. Although more LASIK procedures continue to be performed than PRK and its variants, surface ablation has returned as an attractive alternative in specific indications such as very low corrections and thin corneas. Previously, LASIK flaps were thought to be associated with increased postoperative higher-order optical aberrations than PRK, and the postoperative quality of vision possibly better with wavefront-guided PRK compared to LASIK. This led some surgeons to advocate a complete return to surface ablation and to recommend that LASIK should be avoided altogether for standard corneal refractive surgery.28 Studies have shown an increase in aberration levels after LASIK.29 However, recent data suggest that both techniques are effective with equal vision and equal higher-order aberrations at a 6-month postoperative time point.30 Depending on patient and surgeon factors, either PRK or LASIK can provide successful refractive outcomes.31,32
PREOPERATIVE EVALUATION
When a patient is considering refractive surgery, several issues must be evaluated preoperatively. First, it is important to determine pre-existing ocular or systemic conditions that could interfere with healing or the predictability of the procedure. In addition, the patient’s refractive status, including stability, degree of refractive error, and astigmatism, must be determined. Finally, and perhaps most importantly, the patient’s goals and expectations must be evaluated.
It is important to obtain the patient’s full medical history, review the systems, and perform a complete ocular examination to rule out the presence of any conditions in which refractive surgery is contraindicated. A history of collagen-vascular and autoimmune diseases, such as rheumatoid arthritis, systemic lupus erythematosus, and Sjögren syndrome, are considered contraindications to PRK due to unpredictable corneal wound healing with the potential for corneal melting.33,34,35 A history of keloid scar formation and prior herpes simplex keratitis are relative contraindications. However, systemic antiviral prophylaxis begun preoperatively and continued for several months postoperatively may make PRK safe in patients with a history of herpes simplex keratitis. Diabetes must be well controlled preoperatively because it involves instability of refraction and potentially poor wound healing. Dense amblyopia is a relative contraindication because the refractive procedure puts the patient’s better eye at risk. Patients with this disorder should wear protective spectacles rather than undergo surgery to reduce spectacle use.
A full ocular examination is mandatory. An external examination should consider the orbital anatomy. A deep-set globe, high brow, and/or a narrow palpebral fissure are features that may favor PRK and LASEK over LASIK, Epi-LASIK, or Epi-LASEK, because with the latter techniques it may be difficult or impossible to access the microkeratome and apply the suction ring or patient interface. A thorough examination of extraocular movements is important because the presence of a phoria or tropia could result in postoperative diplopia. Pupil size should be measured because a large pupil may contribute to glare and haloes postoperatively, although recent improvements in our understanding of dim light vision symptoms suggests that corneal aberrations (not the pupil size itself) are the principal issue.36 A commercial pupillometer can more accurately assess pupil size under mesopic or scotopic conditions. Eye dominance is tested in case the patient desires monovision (in monovision corrections, typically the dominant eye is corrected for distance vision). The eyelids and tear film should be evaluated for blepharitis or dry eyes that should be treated preoperatively. Cyclosporin-A has been found to be effective in treating dry eye resulting from refractive surgery in some studies.37 A careful examination of the cornea should reveal the presence of any corneal scars, vessels, or evidence of previous inflammation. Patients with epithelial basement membrane dystrophy (EBMD, often termed map-dot-fingerprint dystrophy) are better candidates for PRK than for LASIK because PRK may be therapeutic by enhancing epithelial adhesion, whereas the microkeratome friction in LASIK may cause a frank epithelial defect.
Preoperative corneal pachymetry is mandatory for all patients.38 The central corneal thickness is determined by ultrasonic pachymetry or with a Scheimpflug or scanning slit topographer. In addition to being a screening test for possible pre-existing keratoconus or other types of corneal ectasia (see later), corneal pachymetry can determine the amount of corneal tissue that will be available for excimer tissue ablation without risking weakening the cornea to the point where postoperative ectasia and irregular astigmatism become significant risks. The current generally used standard is that the cornea must have at least 250 μ or 50% of the original thickness (whichever is greater) of the residual stromal bed under a LASIK flap. If the flap thickness plus tissue ablation depth are calculated to leave inadequate residual stromal thickness, LASIK is contraindicated and surface ablation is preferable.
The lens must be examined closely to rule out the presence of an early cataract, and a dilated-fundus examination should be performed to rule out pre-existing peripheral retinal degeneration or peripheral holes that should be treated preoperatively.
Computed corneal topography is vital in the preoperative evaluation of refractive surgery patients. Corneal topography is particularly useful in the evaluation of irregular astigmatism. Corneal warpage can occur with the use of contact lenses, and its presence will interfere with the accuracy of preoperative refractive measurements. For this reason, soft contacts should not be worn for a minimum of 3 days, and hard contacts should be avoided for at least 2 weeks prior to the preoperative evaluation. If corneal warpage is suspected, the patient should not wear contact lenses until the topography is stabilized (Fig. 48-2).
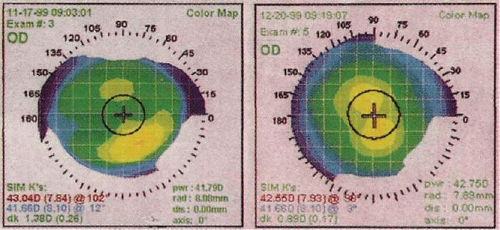 Figure 48-2. Left. Corneal topography of a patient with corneal warpage from hard contact lens wear. Right. One month after the contact lenses were discontinued, the warpage has resolved. |
The presence of frank or subclinical (forme fruste) keratoconus can also be detected by corneal topography (Fig. 48-3). Some series have reported successful PRK in keratoconus suspects.39,40 However, the presence of keratoconus is generally considered a contraindication to PRK because the removal of additional tissue from an already ectatic cornea may lead to further ectasia and unpredictable results. When keratoconus is suspected on topography but is not visible on examination, two tests are helpful. First, the topography should be repeated with the patient looking slightly superiorly (one or two rings on the placido disc). If the patient has true keratoconus, the abnormality of eccentric inferior steepening will persist. If the patient has a slightly inferiorly shifted corneal apex rather than a true keratoconus, the pattern will become symmetric with a slight upgaze. The second test is corneal pachymetry. In true keratoconus, the central cornea will be thinner than average and will thin slightly more when the pachymetry is repeated 1 to 2 mm inferior to the corneal center. Alternatively, anterior segment optical coherence tomography allows for a pachymetry map of the entire cornea, which can be useful in evaluating relative corneal thickness. Current topography devices often include a readout of the posterior corneal topography. An abnormal amount of anterior curvature of the posterior cornea lends further support to a suspicion of corneal ectasia. The clinician should also use a retinoscope to determine whether a “scissoring” light reflex is present, which would increase the likelihood of the presence of keratoconus.
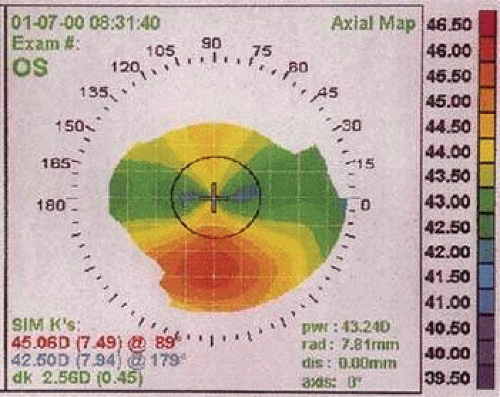 Figure 48-3. Corneal topography of a forme fruste keratoconus. Note the inferior corneal steepening. |
Careful evaluation of the patient’s refractive status is critical. In general, patients should be 18 years of age or older, and the refraction should be stable to within ±0.5 diopter (D) over the previous year. Visual acuity should be checked without correction, as well as with the patient’s current spectacles. Both manifest refraction and cycloplegic refraction must be performed. Corneal topography is a useful adjunct in evaluating astigmatism. In addition, the surgeon must evaluate any clinically significant disparity between the manifest and cycloplegic refractions. Most patients will have a cycloplegic refraction between 0.25 and 1.0 D shifted in the hyperopic direction. Because some or all of this disparity can be attributed to the optics of the peripheral cornea and a small posterior shift of the crystalline lens with cycloplegia, many surgeons will plan their laser input based on the manifest refraction if it has been performed with a careful defogging technique. A disparity between the manifest and cycloplegic refractions of more than 1 D of sphere warrants re-evaluation, often including a postcycloplegic manifest refraction “pushing plus” to overcome accommodative spasm. Accommodative spasm is common in both those with myopia who have become “over-minused” in their contact lenses or spectacles (extra minus causes a slight minification of the image, which causes a perception of higher contrast) and in those with hyperopia who have a lifelong habit of accommodation to improve distance vision. In middle-aged patients, a cycloplegic refraction is still mandatory because surprising amounts of accommodative spasm may remain. Tropicamide 1% is usually strong enough to relax accommodation in patients older than 40 years of age, but Cyclogyl 1% may be advisable in younger patients, especially those with hyperopia. Several clinical tests are helpful for resolving disparities between the manifest and cycloplegic refractions. In addition to a defogging technique that “pushes plus,” a time-honored technique is the duochrome chart (one half of the chart is green, and the other half is red). Because of chromatic aberration, the longer red wavelengths are focused slightly behind the shorter green wavelengths. An over-minused refraction will cause the focal point to be behind the retina. Red wavelengths will be farther retrofocused and therefore letters on the red half of the chart will appear more blurred than the letters on the green half of the chart. Other helpful clinical strategies include placing a 4-mm aperture in the trial frame during the cycloplegic refraction to restrict vision to the more central cornea and then comparing the refraction to the readings from an autorefractor with a defogging device system or a wavefront analyzer.
If there is a discrepancy between the patient’s refractive and corneal cylinders, the refraction should be re-evaluated. If possible, it is desirable to perform a wavefront analysis to identify patients with a high level of preoperative aberration that may become more symptomatic postoperatively, as well as to guide a customized ablation if indicated.
Finally, proper patient education is the key to a successful refractive surgery procedure. The goal of refractive surgery is to decrease the patient’s dependence on glasses and contact lenses. Achieving this goal depends on the patient’s daily visual needs. The patient must understand that the technique is still not as accurate or as predictable as correcting myopia with contact lenses or spectacles, which has a virtually 100% chance of achieving 20/20 or better vision in a healthy eye. The extra time taken with patients to ensure that they fully understand the goal of the procedure can save much frustration for both surgeons and patients postoperatively.
Informed consent should include a discussion of other surgical as well as nonsurgical options for the patient. Likely outcomes, the potential need for enhancements, and potential complications must also be discussed. In addition, presbyopia should be explained, and monovision (in which one eye is intentionally left mildly myopic for near vision) should be offered as an option to middle-aged patients. If the patient is interested, a monovision simulation with contact lenses should be performed prior to the procedure.
SURGICAL TECHNIQUE
Laser Calibration
On the day of surgery, the laser should be checked for an adequate homogenous beam profile, alignment, and power output, following the manufacturer’s guidelines.
Preoperative Planning
Many surgeons use a nomogram adjustment of the correction that is to be programmed into the laser. If possible, it is preferable to perform these calculations in advance of the moment of surgery to avoid time pressure or distractions that may lead to calculation errors. Most nomograms are individualized to the surgeon, laser, and specific technique used, as well as patient factors, which may include the amount of correction, patient age, gender, and other variables. These factors may all influence the outcome of the ablation.
Often the manifest and cycloplegic refractions differ, or the amount and axis of the topographic and refractive astigmatism differ. Consequently, it may be unclear which refraction should be entered into the laser. If it is confirmed that the refractive cylinder differs from the topographic cylinder, it is assumed that lenticular astigmatism or posterior corneal curvature is the cause. In this case, the laser is usually still programmed with the axis and amount of cylinder noted on refraction. The surgeon should take particular care to check the consistency of the axis on the refraction and topography with the value programmed into the laser. This is a common source of error, particularly when there is a conversion between plus and minus cylinder formats.
In many laser models the surgeon also must enter the size of the optic zone, and whether or not a blend of the ablation zone should be performed. If there is sufficient corneal tissue, an ablation zone larger than the scotopic pupil size is usually selected. A “blend zone” is an area of peripheral asphericity that is designed to reduce the possibly undesirable effects of an abrupt transition from the optical zone to an untreated cornea. A common approach to creating a blend zone is to have, for example, a -6 D correction consist of a -5 D correction at a 6-mm optical zone and a -1 D correction at an 8-mm optical zone. The larger the treatment area, the deeper the ablation.
In wavefront-guided custom and wavefront-optimized ablations, these parameters are usually fixed by the wavefront optical measurement and the laser model.
The surgeon must calculate whether an adequate stromal bed will remain. This is rarely an issue for surface ablation, but in thinner corneas and higher dioptric treatments, there may be inadequate tissue for LASIK, prompting the surgeon to select surface ablation. In simple spherical corrections of myopia, the approximate depth of ablation can be calculated by the Munnerlyn formula:
t = S2D/3
where t is the thickness of the tissue ablated in microns, S is the diameter of the optical zone in millimeters, and D is the dioptric correction. For example, in a 6-mm optical zone, the formula is simply 12 × D. A 4-D myopic correction would remove about 48 μ centrally. Note, however, that aspheric peripheral blend zones and wavefront corrections remove more tissue than the simple spherical correction in the Munnerlyn formula, and the surgeon is advised to program the correction into the laser to have the laser software calculate the ablation depth. In addition, the surgeon must remember to input the intended total correction value, not the nomogram-reduced value, to obtain the true amount of tissue removal.
Patient Preparation
Before the laser treatment is performed, the patient should be instructed about the sounds and smell of the laser. Anxious patients may receive an oral sedative, such as diazepam, and the operative eye (in unilateral treatments) should be indicated with an adhesive label or some other temporary mark on the forehead.
Before or after the patient reclines under the head of the laser, the patient’s skin is typically prepped with povidone iodine (Betadine) or alcohol wipes. Some surgeons also use a sterile drape over the skin and lashes. Topical tetracaine and/or proparacaine anesthetic drops are placed in the eye. A lid speculum is placed in the operative eye, and a patch is placed over the fellow eye to avoid cross-fixation. A gauze pad may be taped over the temple between the operative eye and the ear to absorb any fluid run-off. The amount of desired correction, accounting for the vertex distance, is entered into the laser and checked by the surgeon. The patient is asked to fixate on the laser centration light while the surgeon focuses and centers the laser. For most patients, line-of-sight fixation by the patient during PRK produces more accurate centration than globe immobilization by the surgeon.41,42
Surgical Technique
In most original techniques and in U.S. phase III investigations, the epithelium is removed by a sharp blade or a blunt spatula (Fig. 48-4). In this technique, the surgeon defines the outer limit of de-epithelialization with an optical zone marker and then débrides the periphery followed by the center. To avoid desiccation and resultant variability in ablation rates, the surgeon must perform this procedure efficiently. Skill is required to avoid nicking the Bowman layer. An ophthalmic surgical cellulose sponge lightly moistened with an artificial tear lubricant, such as carboxymethylcellulose 0.5%, is brushed over the surface of the cornea to remove any residual epithelium and provide a smooth surface (Fig. 48-5). Subsequently developed alternative methods for removing the epithelium include the use of a rotating corneal brush,43 application of diluted absolute alcohol (typically around 20% concentration) to the corneal surface to loosen the epithelium,44,45,46 and transepithelial ablation by the excimer laser itself.47 The epithelium should be removed efficiently and consistently to prevent hydration changes in the stroma, because the rate of excimer laser ablation may be increased by excessive corneal stromal dehydration, resulting in an overcorrection.48
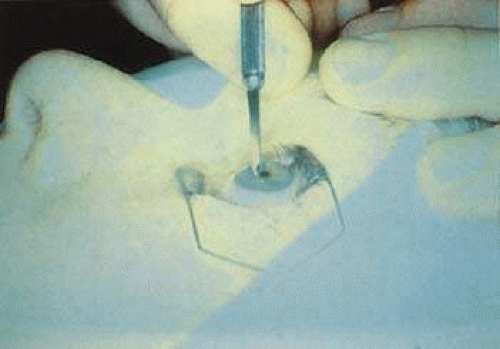 Figure 48-4. De-epithelialization with a blade before PRK. |
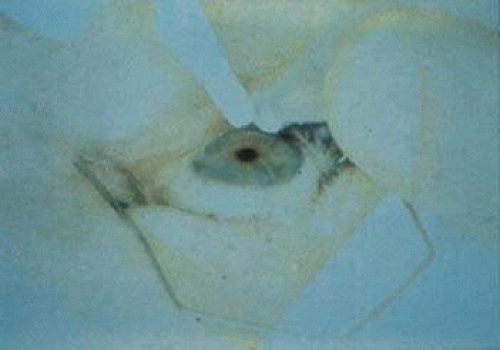 Figure 48-5. Final cleaning of the surface before beginning the laser exposure. |
In the LASEK variant of PRK, which was first described by Camellin,49 the goal is to preserve the patient’s epithelium. Instead of debriding and discarding the epithelium, or ablating the epithelium with the excimer laser, the surgeon uses a technique to remove an intact sheet of epithelium. First, the surgeon can place a radial mark of gentian violet ink to assist in later realignment of the epithelial flap. Most commonly, a solution of approximately 20% diluted absolute alcohol is applied for 20 to 30 seconds. The alcohol is restricted to the area to be de-epithelialized with a ring (usually an optical zone marker) pressed onto the corneal surface, or by means of a round surgical sponge soaked with the alcohol solution. After the desired exposure time has passed, the alcohol is removed from the “well” of the optical zone marker by absorption into a microsurgical spear sponge. After the alcohol is fully absorbed and the optical zone marker is removed, the ocular surface is copiously irrigated with balanced salt solution (BSS) to minimize toxicity to the limbal germinal epithelium. The surgeon then uses an instrument, which often has a hoe or spatula configuration, to carefully separate a flap of full-thickness epithelium from the underlying Bowman layer. The epithelium is delicately folded back on itself until all of the epithelium has been removed except for a small “hinge,” which is usually located superiorly. Figure 48-6 shows the key steps involved in performing LASEK.
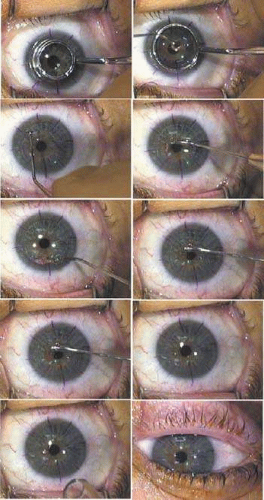 Figure 48-6. Technique for LASEK. A. After the gentian violet radial orientation marks are placed, the epithelial flap is delineated with an optical zone marker or similar instrument. B. Alcohol to loosen the epithelial flap is carefully contained within a trephine-shaped well pressed on the cornea. C. The separation of the flap edge is begun with a “microhoe.” D. The separation of the epithelial flap continues as a “micro hockey stick” strokes the epithelium back, with care taken to not perforate the epithelium. E. The epithelium is fully retracted off the area to be ablated by the laser, leaving a “hinge” of epithelium for about one clock hour in the superior periphery. F&G. After the laser exposure is completed, the epithelial sheet is gently replaced by floating it and stroking it with a BSS cannula. H. The epithelial flap is realigned using the radial marks. I. The epithelial sheet is briefly dried with filtered air through a microtip to begin adhesion to the stroma. J. After a BSCL is placed, the procedure is complete. (All photographs courtesy of Daniel Durrie, M.D.) |
The goal of LASEK is to reduce postoperative pain and achieve a speedier return of vision compared to PRK, and perhaps to reduce postoperative haze formation.50 A recent meta-analysis comparing LASEK and PRK showed comparable refractive efficacy and accuracy between the two groups at 1 and 12 months. Additionally, compared with PRK, LASEK did not relieve discomfort on day 1 posttreatment or reduce corneal haze intensity at 6 and 12 months posttreatment.51
Efforts have also been made to develop a variant of the microkeratome used in LASIK. The microkeratome is modified with a dull blade and thin applanation plate to mechanically remove the epithelial flap without the use of toxic agents, such as alcohol, that are used in LASEK. The goal is to create an epithelial flap that may remain viable and more likely to successfully re-adhere postoperatively. These techniques are most commonly termed epi-LASIK. Hondur et al52 compared epi-LASIK to LASEK and found similar results at 1 year. Epi-LASIK did have a slightly longer mean time to epithelial healing initially, but a similar amount of haze clinically and by confocal microscopy gray-scale quantification at all time points.
Due to incomplete epithelial flaps and occasional stromal incursions with some of the epikeratomes, the volume of epi-LASIK procedures has decreased.53 A newer variation of advanced surface ablation is epi-LASEK. Epi-LASEK is similar to epi-LASIK except that alcohol is added with the goal of facilitating creation of the epithelial flap. Camellin and Wyler54 have shown that the addition of alcohol did allow for a better flap and hinge creation without the addition of pain or haze when comparing epi-LASEK to epi-LASIK.
Last, the excimer laser itself may be used to remove the epithelium in transepithelial photorefractive keratectomy (T-PRK). In this variant, the epithelium is removed with the excimer laser by monitoring the disappearance of blue fluorescence during the ablation.55 Ghadhfan et al56 reported T-PRK visual outcomes to be equivalent to traditional PRK and superior to LASIK or LASEK for low to moderate myopia, and T-PRK visual outcomes to be superior to LASIK, LASEK, and traditional PRK for high myopia.
Laser Ablation
After the epithelium is out of the treatment zone and the stroma has been exposed with one of these techniques, the laser is centered and focused according to the manufacturer’s recommendations. Improved PRK centration occurs when the aiming beams or reticule are centered on the entrance pupil instead of the corneal apical light reflex.57,58 The patient is instructed to maintain good fixation during the stromal ablation. Small microsaccades should not adversely affect the outcome of the procedure. If the patient begins to lose fixation, however, the surgeon should immediately stop the treatment until adequate refixation is achieved. If the laser includes a tracking mechanism, it is still important for the surgeon to monitor for excessive eye roll, which can result in decentration despite the tracking device. Additionally, some current excimer lasers offer iris registration to improve toric accuracy. If the treatment involves a large amount of astigmatism correction, this should be used. If iris registration is not present, the eye should be marked at 3 and 9 o’clock (prior to removal of the epithelium) to account for any cyclotorsion.
To correct myopia, the surgeon flattens the cornea by placing the largest number of laser pulses centrally and progressively fewer pulses toward the periphery of the optical zone (Fig. 48-7). To correct hyperopia, the cornea must be steepened. No pulses are placed in the precise center, the maximum number of pulses are placed in the peripheral optical zone, and then a blend zone creates a smooth transition from the edge of the optical zone back to the peripheral corneal surface (Fig. 48-8). Although the excimer laser beam at 193 nm is invisible to the human eye, a faint fluorescence of deep blue light is sometimes visible during stromal ablation. The sound of the laser firing is the main feedback signal to the surgeon, along with an alteration in the light reflex as the stromal ablation progresses. If topical mitomycin C (MMC, usually 0.2 mg/mL) is to be used (usually in cases of high myopic correction) when the PRK is applied to a LASIK flap, or to enhance a previous PRK hazy scar, most surgeons will apply it as a soaked pledget placed on the ablated surface for 1 minute or less at the end of the laser exposure.59 Several studies have shown MMC to be a safe adjunct in PRK. In highly myopic (>–8 D), MMC 0.2 mg/mL for 45 seconds did not delay epithelialization nor cause any adverse effects at 12 months. It did, however, induce an approximately 6% overcorrection.60 It has also been shown to effectively prevent primary or recurrent haze in primary or retreatment PRK or PTK eyes at 6 months.61 Confocal microscopy has shown no significant side effects on keratocytes after PTK with MMC compared to PTK alone.62 Thornton et al63 studied the effect of low-dose MMC (0.02 mg/mL) on PRK and found that the traditional dose of 0.2 mg/mL was more effective for myopia greater than or equal to -6 D and deeper ablation depths of 75 microns or more. However, for lower amounts of myopia or shallow ablations, the lower dose of MMC (0.02 mg/mL) appears to be as effective as the traditional dose (0.2 mg/mL). Despite the reported safety of MMC, vision-threatening complications, including glaucoma and corneal perforation, have been reported. The search continues for the ideal topical wound-healing modulator that has a high specificity for collagen synthesis without toxic side effects.
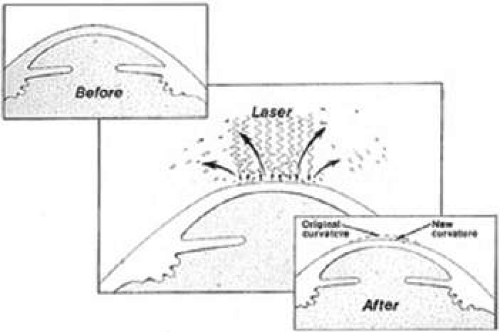 Figure 48-7. Schematic representation of the excimer laser flattening the central cornea for the treatment of myopia. |
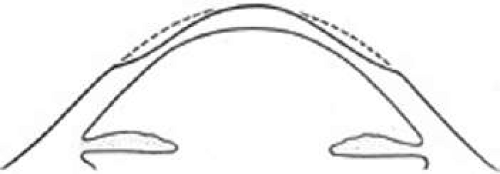 Figure 48-8. Schematic representation of the pattern of corneal ablation necessary to correct hyperopia with the excimer laser. The greatest amount of tissue is removed from the periphery of the optical zone with a gradual transition toward the anterior corneal surface. |
Immediate Postoperative Treatment
After the procedure is completed, antibiotic, steroid, and nonsteroidal anti-inflammatory (NSAID) drops are usually placed in the eye, followed by a bandage soft contact lens (BSCL). If the LASEK, epi-LASIK, or epi-LASEK variants have been performed, the surgeon carefully floats and repositions the epithelial sheet back into position with BSS before he or she applies the medications and the BSCL. Some surgeons also apply chilled BSS before and/or after the PRK procedure in the belief that cooling reduces pain and haze formation, although the advantage of this practice has not been substantiated in a controlled study. If the patient cannot tolerate a BSCL, a pressure patch may be used.
POSTOPERATIVE CARE
During the first 24 hours, the patient may experience a large amount of pain, which may be relieved by an oral narcotic pain medication. Topical NSAID drops have been shown to significantly reduce postoperative pain,(64–68) although they may also slow the rate of re-epithelialization and promote sterile infiltrates. Studies have also demonstrated a reduction in pain with the use of topical anesthetic drops.69,70,71 Topical anesthetic drops must be used cautiously because they may cause severe corneal complications when used excessively over a prolonged period. However, topical tetracaine used ad libitum in conjunction with a BSCL for 1 or 2 days after PRK does not appear to delay re-epithelialization or cause keratopathy. Oral analgesics are sometimes necessary. These include oral NSAIDs, oral prednisone, gabapentin or pregabalin, and opiate pain medicaitions.53 The patient should be followed closely until the epithelium is intact, usually within 72 hours. At this point, the BSCL, antibiotic, and NSAID drops (if used) may be discontinued. If they have been used at all, the topical anesthetic drops must be confiscated from the patient to prevent prolonged use. Following re-epithelialization, a decision is made to continue or discontinue the topical steroid drops. The administration of topical steroids to modulate postoperative wound healing and reduce anterior stromal haze and regression of the refractive effect remains a controversial subject. Some investigators have demonstrated that corticosteroids have no significant long-term effect on corneal haze or visual outcome after PRK.72,73,74,75 Other studies demonstrated that steroids were effective in limiting haze and myopic regression after PRK, particularly after higher myopic corrections.76,77 Currently, surgeons who advocate the use of topical steroids after removal of the BSCL generally believe that only patients with higher levels of myopia (e.g., greater than about 4.0 D) require long-term topical steroids. If they are used, steroid drops are usually tapered over a 3- to 4-month period, depending on the patient’s corneal haze and refractive outcome. Keratocyte healing activity is maximal at 1 to 2 months. Abrupt termination of steroid drops at this time may trigger an excess healing reaction with haze formation and regression of the correction.
CLINICAL RESULTS
Impact of Evolving Technology
The effectiveness of PRK improved markedly during the pre–market-approval clinical trials conducted in the United States from 1990 to 1994 because the broad-beam excimer laser systems were updated several times and the surgeons became more familiar with the PRK technique. Also, the size of the ablation zone increased as experience revealed that small ablation zones, which were originally believed to be desirable to limit the depth of tissue removal, produced more haze and regression, as well as subjective glare and haloes. Larger treatment zones, including larger true optical zones and aspheric peripheral blend zones, are now commonly used to improve both optical quality and refractive stability in both myopic and hyperopic treatments.
Subsequent improvements in beam quality and the development of scanning slit and spot lasers have been associated with better outcomes, including less postoperative haze and less irregularities (especially fewer central island elevations).
Many surgeons now use outcome analysis programs that refine the success rates. Scanning spot laser technology necessitated the development of tracking technology to ensure proper registration of the shot pattern. The potential for pupil tracking technology to improve centration led all of the manufacturers of such devices to introduce pupil tracker technology.
The most common types of tracker technology use one of two strategies. In so-called closed-loop trackers, high-speed oscillating infrared beams scan across the edge of a fixed dilated pupil. These beams detect the abrupt change in reflected light at the edge of the pupil. This signal then directs rapidly responding mirrors to create a space-stabilized image, and the laser treatment is located on the cornea based on that image.
The second type of tracker is based on an infrared image of the pupil and uses video technology to monitor the location of the pupil image and shift the laser beam accordingly, in a so-called open-loop system.
Other improvements in excimer laser technology include tracking positionally induced cyclotorsion either by detection of limbal marks (placed by the surgeon) or iris registration. Iris registration essentially maps the iris and creates landmarks during wavefront acquisition when the patient is seated and detects these landmarks when the patient is supine. This allows for accurate tracking of cyclotorsion. However, this technology has not translated into improved outcomes in wavefront-guided treatments.78,79
One of the most significant improvements in refractive surgery has been the development and implementation of wavefront-guided and wavefront-optimized treatments. Conventional treatments are spherocylindrical only. A wavefront-guided excimer laser uses an evaluation unique to each eye to determine the best laser treatment plan for an individual patient. Wavefront-guided treatments are based on aberrometry measurements and are designed to treat both spherocylinder and higher-order aberrations. Currently, wavefront-guided lasers approved in the United States include the Alcon LADARVision CustomCornea, AMO VISX S4 CustomVue, and the Bausch & Lomb Technolas 217z Zyoptix. A wavefront-optimized laser uses theoretical wavefront data to determine the best overall tissue ablation plan rather than measurements specific to the patient. Wavefron-optimized treatments are designed to treat spherocylinder errors while reducing induced spherical aberration. The Alcon Allegretto Wave Light offers both wavefront-optimized and wavefront-guided treatments.
Trials of wavefront analysis-guided and optimized treatments generally report improvements in both visual acuity and quality of vision compared to conventional excimer treatments.
Most recently, evaluation of topography-guided treatments are being evaluated. Topography-guided treatments may be beneficial in patients with highly aberrated corneal topographies and irregular astigmatism. Topography-guided treatments evaluate many more data points compared to wavefront-guided treatments.
Clinical Outcomes
In a study of the first laser to gain FDA approval in the United States (the Summit Phase III PRK study80), 701 eyes with myopia ranging between -1.5 and -6.0 D were enrolled, with 2-year follow-up data available on 612 of the eyes. In that trial, 92.5% of the eyes had an uncorrected visual acuity (UCVA) of 20/40 or better, and 66.5% had a UCVA of 20/20 or better. In addition, 77.8% of the eyes had a spherical equivalent manifest refraction within 1.0 D from emmetropia, and 6.9% had lost two lines of best corrected visual acuity (BCVA). In the VISX Phase III Study for low myopia,81 691 eyes with myopia ranging from -1.0 to -6.0 D were followed for 24 months. In that study, 85% of the eyes had a UCVA of 20/40 or better, with 79% of the eyes within 1.0 D of emmetropia, and 1% of the eyes lost two lines of BCVA.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


