Purpose
To evaluate the safety and efficacy of a supraciliary micro-stent (CyPass Micro-Stent; Transcend Medical, Menlo Park, California, USA) for surgical treatment of glaucoma in patients refractory to topical medications.
Design
Multicenter, single-arm interventional study.
Methods
Patients with open-angle glaucoma (Shaffer Grade 3 and 4) and uncontrolled medicated intraocular pressure (IOP) >21 mm Hg at baseline and candidates for conventional glaucoma surgery were enrolled. Glaucoma medications were discontinued at surgery and resumed at investigator discretion. CyPass Micro-Stent implantation was completed in all patients using a standard clear corneal approach. Adverse events, postoperative IOP changes, and need for IOP-lowering medications during the first 12 postoperative months (12M) were monitored.
Results
Sixty-five eyes were enrolled, and 55 were available at 12M, accounting for loss to follow-up and early termination. Baseline IOP was 24.5 ± 2.8 mm Hg, and the mean number of medications recorded was 2.2 ± 1.1. There were no serious intraoperative events or major adverse events (eg, retinal or choroidal detachment, persistent uveitis, persistent hyphema, hypotony maculopathy). The most common adverse events included IOP increases >30 mm Hg beyond 1 month (11%, 7/65), transient hyphema (6%, 4/65), and cataract progression (12%, 5/41 phakic eyes). Mean IOP was 16.4 ± 5.5 mm Hg at 12 months—a 34.7% reduction ( P < .0001). Mean medication usage also decreased from baseline to a mean of 1.4 ± 1.3 medications at 12M ( P = .002). In eyes originally indicated for conventional glaucoma surgery, no secondary surgery was performed in 83% (53/64).
Conclusion
Supraciliary stenting with the CyPass Micro-Stent effectively lowers IOP as a surgical treatment for glaucoma, precluding the need for more invasive glaucoma surgery in >80% of patients at 1 year, thereby reducing postoperative glaucoma surgical complications.
Glaucoma remains the second-leading cause of blindness in the world. Surgical therapies for glaucoma (eg, trabeculectomy, nonpenetrating glaucoma surgery, or shunt implantation) are well-established treatment options. It is well known, however, that the formation of a filtering bleb can potentially end in subconjunctival fibrosis, blebitis, hypotony, endophthalmitis, and filtration failure. Such complications commonly restrict the use of bleb-forming surgical therapies to only individuals who have failed medical and laser trabeculoplasty therapy and have experienced significant visual field deterioration.
One approach to a safer surgical treatment for glaucoma includes conjunctiva-sparing interventions that target the suprachoroidal space rather than the trabecular meshwork outflow pathway. Uveoscleral outflow is difficult to measure but may account for up to half of the aqueous humor drainage in normal human eyes. Experimental evidence suggests that a negative pressure gradient of 3–4 mm Hg exists between the suprachoroidal space and the anterior chamber and provides a potential driving force for aqueous outflow to the former space. Nontrabecular outflow can also be increased by prostaglandin analogues, which are the most frequently used topical intraocular pressure (IOP)-lowering agents. It has been suggested that the uveoscleral pathway has a higher capacity for a therapeutic effect than the conventional pathway via the trabecular meshwork. Further, clinical experience from traumatic or iatrogenic cyclodialysis demonstrates a significant hypotensive effect, generally correlating with the patency of the cleft. Thus, preventing cleft closure through controlled, permanent stenting is expected to allow continued aqueous outflow and lowered IOP.
Previous efforts to surgically increase suprachoroidal outflow have had limited success, owing to the difficulty of accessing the suprachoroidal space effectively without inducing significant surgical trauma and complications. It has also been challenging to maintain an open conduit over time in the absence of a permanent implant to maintain the outflow channel, without which cleft closure can be associated with substantial and sudden IOP elevation.
The CyPass Micro-Stent (Transcend Medical, Inc, Menlo Park, California, USA) is a polyimide implant intended to create a new permanent conduit for additional outflow of aqueous humor from the anterior chamber to the suprachoroidal space. The micro-stent can be placed into the supraciliary space using an application device via a clear corneal approach. The surgery is minimally invasive, spares the conjunctiva, and avoids the formation of a filtering bleb.
In recent studies, supraciliary micro-stenting in combination with phacoemulsification cataract surgery demonstrated significant IOP lowering through up to 24 months follow-up, without the major complications of conventional glaucoma surgery. This is the first report of the DUETTE clinical study (A Study of CyPass Implantation in Patients With Open Angle Glaucoma Refractory to Single or Multi-Agent Topical Therapy), which evaluated the clinical utility of supraciliary stenting as a treatment for glaucoma refractory to topical medications.
Methods
Study Design
The CyPass Micro-Stent is an investigational device that is currently undergoing United States Food and Drug Administration trials and has received the Conformité Européenne Mark, meaning it is available commercially in many European countries. DUETTE is an ongoing, multicenter, prospective, single-arm, interventional clinical trial evaluating the CyPass Micro-Stent implant. Patients with open-angle glaucoma (OAG) refractory to medical therapy and considered for conventional glaucoma surgery (trabeculectomy or shunt procedure) by the investigator were enrolled under a standardized treatment protocol ( ClinicalTrials.gov identifier NCT01166659 ). The DUETTE study protocol was approved by Freiburger Ethik-Komission International institutional review board (Freiburg, Germany), as well as by the ethics committee at each hospital, and adhered to the tenets of the Declaration of Helsinki. All subjects provided written informed consent before any study procedures were undertaken.
Study Subjects
All study subjects had a complete ophthalmic examination preoperatively, including medical history, slit-lamp examination, dilated funduscopic ophthalmoscopy, IOP measurement via Goldmann tonometry, and best-corrected distance visual acuity (BCDVA). Inclusion criteria were: presence of primary open-angle glaucoma with Shaffer Grade 3 or 4 as assessed by clinical gonioscopy, medicated IOP between 21 and 35 mm Hg, optic nerve vertical cup-to-disc ratio greater than 0.7, and visual field defect noted via the Humphrey Visual Field 24-2 Swedish Interactive Threshold Algorithm (SITA) Standard or equivalent, and failing to achieve or maintain target IOP control (per each investigator’s discretion) with use of 1–4 IOP-lowering medications, with consideration of conventional glaucoma surgery. Subjects could be either phakic or pseudophakic. Exclusion criteria included angle closure or Shaffer Grade 1 or 2 angles; diagnoses of traumatic, malignant, uveitic, or neovascular glaucoma; discernible congenital anomalies of the anterior chamber or iridocorneal angle; or known intolerance or hypersensitivity to topical anesthetics, miotics, mydriatics, or polyimide. Patients with previous incisional glaucoma surgery were also excluded, as well as patients with any clinically significant ocular pathology other than OAG.
Study Device
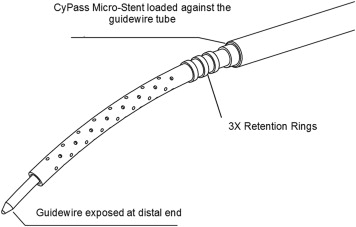
The CyPass Micro-Stent is a fenestrated micro-stent made of a biocompatible polyimide material ( Figure 1 ). It is 6.35 mm in length and 510 μm in external diameter. As the micro-stent is inserted, it assumes the curvature of the specialized applier guidewire to follow the scleral contour along the supraciliary space. When it is correctly inserted into the supraciliary space, the material stiffness, in conjunction with a series of retention rings at the proximal end, helps ensure the stability of the device in the angle and the supraciliary space. The micro-stent is designed to increase aqueous outflow via the uveoscleral pathway.
Surgical Implantation Technique
All glaucoma medications were stopped at the time of surgery except in circumstances where the principal investigator determined that it was in the subject’s best interest to continue some or all of these agents. Surgeons used their standard anesthesia regimen for anterior segment surgery. A shelved 1.5-mm corneal incision was performed at the limbus across from the target implantation site, acetylcholine was injected to achieve miosis, and then the anterior chamber was filled with a viscoelastic agent to maintain the chamber and expand the angle. The CyPass device was threaded onto the retractable guidewire of the applier, and implantation was carried out through the clear corneal incision.
The procedure was visualized using a goniolens (Ocular Instruments, Inc, Bellevue, Washington, USA), and insertion was initiated with the nonincisional tip of the guidewire, which allowed blunt dissection into the ciliary tissue to create a dissection plane between the ciliary body and the sclera. The micro-stent was inserted into the dissected area until it reached the supraciliary space and retention features were engaged. The guidewire was then retracted, leaving the micro-stent in place, and the applier withdrawn from the eye. Viscoelastic was evacuated using irrigation and aspiration. Each site used its standard course of postoperative antibiotics and steroids. Implant positioning was confirmed postoperatively with gonioscopy. In some cases, optical coherence tomography (Visante OCT; Carl Zeiss Meditec, Jena, Germany) or ultrasound biomicroscopy (Humphrey UBM 840, 50 MHz; Carl Zeiss Meditec) was used to assess the CyPass position.
Study Measures
Standard postoperative follow-up visits were at day 1, week 1, and months 3, 6, and 12. Reintroduction of IOP-lowering medications after surgery was left to the discretion of the investigator and dependent on the target IOP of each of the subjects. Ocular device–related adverse events as well as unanticipated adverse events were collected at each visit. Patient postoperative examinations included gonioscopic assessment of implant placement, slit-lamp examination, dilated fundus examination, and measurement of IOP and BCDVA. The primary outcome measure was paired IOP reduction at 12 months as compared to baseline. Paired IOP reduction is defined as the reduction in IOP for the study eye from baseline to the censored time point. Secondary endpoints included need for additional incisional glaucoma rescue surgery (trabeculectomy, tube shunt) and ocular hypotensive medication use at 12 months.
Statistical Methods
Postoperative IOP and medication use at 6 months and 12 months were compared to baseline in a paired, nonparametric analysis using the Wilcoxon signed rank test. Eyes that were reoperated were considered not evaluable and were therefore not included in the follow-up analysis, in order to reduce the confounding effect of additional glaucoma surgery.
Results
Demographic information for the 65 eyes of 65 subjects implanted is presented in Table 1 . Mean IOP at baseline was 24.5 ± 2.8 mm Hg and mean number of topical medications was 2.2 ± 1.1.
| Total subjects enrolled | 65 |
| Mean (SD) age, y | 68.3 (10.5) |
| Female, n (%) | 45 (69) |
| Phakic eyes, n (%) | 41 (63.1) |
| Mean (SD) baseline IOP, mm Hg | 24.5 (2.8) |
| Mean (SD) baseline number of IOP-lowering medications | 2.2 (1.1) |
| 0 medications, n (%) | 1 (1.5) |
| 1 medication, n (%) | 19 (29.2) |
| 2 medications, n (%) | 20 (30.8) |
| 3 medications, n (%) | 16 (24.6) |
| 4 medications, n (%) | 9 (13.8) |
| Mean (SD) BCDVA, letters | 74 (15) |
Safety analysis included all 65 implanted patients based on investigator-reported adverse events. Of the 65 subjects, 9 subsequently underwent trabeculectomy and 2 received an additional CyPass Micro-Stent. Of these 11 subjects receiving secondary glaucoma surgery, 3 were exited from the study early, 2 by the subjects’ decision and 1 by the investigator’s decision owing to glaucoma disease progression. Four additional subjects voluntarily withdrew from the study, and 3 subjects were lost to follow-up. This leads to a total of 10 subjects exiting the study early, leaving 55 eyes with IOP and medication data available at 12 months.
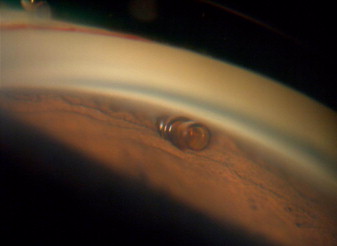
The micro-stent was successfully implanted in all eyes of all study subjects. There were no sight-threatening intraoperative complications. Proper implant positioning was confirmed via gonioscopic observation ( Figure 2 ) and, in some cases, postoperative UBM or OCT ( Figure 3 ). There were no serious device-related ocular adverse events during the postoperative follow-up period ( Table 2 ). There were also no significant differences between study centers overall with respect to the rate of adverse events ( Table 3 ).

| Adverse Events/Complications | n (%) |
|---|---|
| Inflammation/anterior chamber reaction persisting beyond first postoperative month | 0 (0) |
| Hypotony (<6 mm Hg) persisting beyond first postoperative month | 0 (0) |
| Hypotony maculopathy | 0 (0) |
| Shallow anterior chamber (no central touch) | 0 (0) |
| Transient IOP increase >30 mm Hg | 7 (10.8) |
| Transient hyphema a (lasting > 1 day) | 4 (6.2) |
| Corneal edema persisting beyond first postoperative month | 0 (0) |
| Suprachoroidal hemorrhage | 0 (0) |
| Retinal detachment | 0 (0) |
| Explanted device | 0 (0) |
| Device repositioning | 0 (0) |
| BCDVA reduced from baseline by ≥2 lines | 2 (3.1) |
| Iris atrophy | 0 (0) |
| Cataract progression | 5 (7.7) |
| Endophthalmitis | 0 (0) |
| Secondary glaucoma surgical intervention | 12 (18.5) |
| Trabeculectomy | 9 (13.8) |
| Additional CyPass implantation | 2 (3.1) |
| Laser trabeculoplasty | 1 (1.6) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


