and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
Superior oblique tenotomySuperior oblique tenectomyBrown’s syndromeSilicone tendon expanderWright procedure for superior oblique overactionSplit tendon elongationPosterior tenectomy of the superior oblique tendonSuperior oblique tendon weakening procedures are used in the management of various types of strabismus, including superior oblique overaction, inferior oblique palsy, and Brown’s syndrome (see Chap. 7). Most procedures weaken the superior oblique muscle by slackening the tendon. Uncontrolled procedures include tenotomy and tenectomy, in which the tendon is cut and the cut ends are free to widely separate or scar back together. These uncontrolled procedures should not be used in patients with binocular fusion, as the incidence of consecutive superior oblique palsy is more than 50 %.
Controlled lengthening of the tendon grades the induced slack. The two most effective controlled lengthening procedures are the Wright silicone tendon expander [1–3] and the split tendon elongation procedure. These procedures have significantly reduced the complication of consecutive superior oblique palsy and have had excellent outcomes. The superior oblique silicone tendon expander and the split tendon elongation procedures keep the tendon ends apart at a fixed distance and thus are preferred by the authors.
The superior oblique recession has been described as a controlled weakening procedure, but it has the disadvantage of changing the characteristics of the superior oblique insertion. Normally the superior oblique insertion spans from the superior rectus insertion to 6 mm from the optic nerve. After recessing the superior oblique, the surgeon creates a new insertion site. The broad insertion is now collapsed and is nasal and anterior to the original insertion. This new insertion position dramatically changes the superior oblique muscle functions, from a depressor and abductor to an elevator and adductor. The complication of limited depression has been well described following the superior oblique recession procedure.
Another controlled elongation procedure is the suture bridge, also called the “chicken stitch.” A suture is placed between the cut tendon ends to provide a graded separation. The problem with the suture bridge is the suture provides a scaffolding for fibrosis that can reunite the tendon ends. Reuniting of the tendon ends can result in postoperative undercorrection.
Another type of superior oblique weakening procedure is based on selectively removing the posterior tendon fibers (see Fig. 19.15). The idea is to reduce the depression and abduction functions but prevent postoperative extorsion by leaving the anterior fibers intact. This procedure has relatively little effect because it is performed on the temporal side of the superior rectus muscle. When the temporal fibers are removed from the sclera, they do not retract; rather, they scar down to the sclera under the superior rectus muscle. The posterior tenectomy procedure may be useful for mild superior oblique overaction, but a full tendon lengthening procedure is required for more significant overaction and Brown’s syndrome.
19.1 Surgical Exposure for Superior Oblique Tendon Weakening
Superior oblique tendon weakening procedures like tenotomy, Wright’s silicone tendon expander, and split tendon elongation should be performed nasal to the superior rectus muscle. Temporal tenotomies usually have minimal effect, as the superior oblique tendon is sandwiched between the superior rectus and the sclera. Another disadvantage of the temporal approach is that the tendon is extremely splayed out at its insertion, making it difficult to hook and isolate all of the posterior superior oblique tendon fibers. Finally, the nasal approach leaves the normally broad insertion intact, maintaining its three important functions of abduction, depression, and intorsion.
The preferred procedure for exposure of the tendon, developed by Dr. Marshall Parks, is to perform the superior oblique surgery nasal to the superior rectus muscle through a temporal conjunctival incision. By placing the conjunctival incision temporal to the superior rectus muscle and then reflecting the incision nasally, the surgeon can keep the nasal intermuscular septum intact, minimizing scleral-tendon scarring. Additionally, intact nasal intermuscular septum is important to maintain the anatomical relationships of the superior oblique tendon, and it helps to reduce the incidence of postoperative superior oblique palsy or limited depression.
19.1.1 Operative Procedure: Temporal Incision–Nasal Tendon Surgery
Figures 19.1, 19.2, 19.3, 19.4, 19.5, and 19.6 illustrate the procedure for exposure of the superior oblique tendon prior to tenotomy, Wright’s silicone tendon expander, or split tendon elongation.
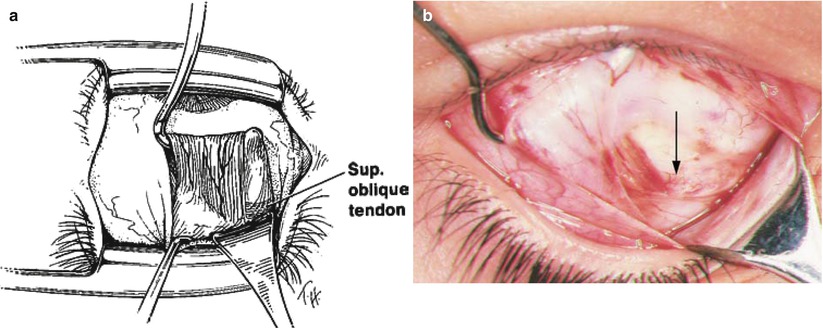
Fig. 19.1
A left eye with a superior temporal fornix incision through conjunctiva, and a separate incision through Tenon’s capsule. The conjunctival incision abuts the temporal aspect of the superior rectus (SR) muscle
Fig. 19.2
A Jameson hook is placed underneath the superior rectus muscle, and the eye is retracted down. Hook right next to the superior rectus muscle insertion to avoid pulling up on the superior oblique tendon. A small Stevens hook is used to pull the incision nasally over the tip of the Jameson hook
Fig. 19.3
The conjunctival incision is reflected nasally over the superior rectus insertion. Notice that the bulb tip of the Jameson hook is covered with intermuscular septum. Do not bare the tip of the Jameson hook; instead, leave intermuscular septum intact
Fig. 19.4




(a) A Desmarres retractor is inserted along the nasal border of the superior rectus muscle, and the lid speculum is removed in order to gain posterior exposure. The superior oblique tendon can be seen (through its fascial covering) as pearly white fibers that run perpendicular to the course of the superior rectus muscle. (b) The nasal aspect of the superior rectus muscle is shown. The superior oblique tendon is located nasal to the superior rectus muscle, approximately 12 mm posterior to the superior rectus insertion. Because the superior oblique tendon (arrow) is surrounded by fascia, it is somewhat difficult to see
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
