Superior Oblique Muscle Surgery
Richard A. Saunders
Ronald G. W. Teed
Superior oblique muscle dysfunction manifests clinically as incomitant hypertropia, A-pattern strabismus, and torticollis, and may be accompanied by vertical or torsional diplopia. These abnormalities can be either congenital or acquired.1 Surgical intervention is usually aimed at correcting superior oblique muscle dysfunction, most often by weakening an “overacting” muscle or strengthening an “underacting” muscle. Superior oblique muscle surgery is occasionally performed to compensate for trochlear dysfunction (e.g., Brown syndrome) or as part of the management of strabismus problems not directly involving the superior oblique muscle (e.g., oculomotor nerve palsy).
In most cases, superior oblique muscle dysfunction is associated only with other strabismus disorders.2,3 Some cases may be part of recognized syndromes (Apert, Crouzon), craniocervical junction deformities (Chiari malformation), or neural tube defects (meningomyelocele).4,5 Familial transmission of superior oblique muscle palsy has been reported.6,7,8 Rarely, myasthenia gravis and thyroid eye disease may involve the superior oblique muscle.9,10
The Challenges of Superior Oblique Muscle Surgery
Superior oblique muscle contraction produces a vector of force directed anteriorly and medially with respect to the orbit. The relative proportion of vertical, torsional, and horizontal forces exerted on the eye depends on direction of gaze. In adduction, the primary action of the superior oblique muscle is depression, but this becomes intorsion when the eye is abducted. Any procedure that strengthens or weakens the action of the superior oblique muscle therefore has multiple, gaze-dependent effects on ocular alignment. These complex and sometimes confusing actions can be intimidating to the ophthalmic surgeon. It is this unusual anatomy, difficult exposure, and unpredictable surgical outcomes that undoubtedly led to von Graefe’s frequently quoted admonition (“Noli me tangere”) that surgery on the superior oblique muscle should not be attempted.11
It was not until 1935 that Wheeler12 showed that direct surgery on the superior oblique tendon could be performed to strengthen the action of an underacting superior oblique muscle. In 1942, Hughes and Bogart13 described a procedure to weaken the action of the superior oblique muscle by recessing the trochlea. Later that decade, Berke14 described and carefully illustrated superior oblique tendon tenotomy. His operation, with subsequent modifications, became the standard method of correcting superior oblique muscle overaction.15 Nevertheless, the reluctance of most ophthalmic surgeons to operate on the superior oblique muscle was reiterated by Fink16 as recently as 1947. Although superior oblique muscle surgery is now common, prior to 1970 about the only time an ophthalmologist saw the superior oblique muscle was during an enucleation (Eugene Helveston, personal communication, October 14, 2008).
As a result of better understanding of the anatomy and physiology of the superior oblique tendon and trochlea, improved surgical instruments and sutures, and innovative surgical techniques, superior oblique muscle surgery is now more commonly performed. Appropriate surgical indications include strabismus manifesting as clinical overaction or underaction of the superior oblique muscle(s), such as A-pattern esotropia and exotropia, superior oblique muscle palsy, Brown syndrome, and complex alignment defects requiring intervention on a “normal” superior oblique muscle, such as oculomotor nerve palsies, nystagmus with a cyclovertical null point, and dissociated vertical deviation. When properly performed, superior oblique muscle surgery is safe, effective, and yields results that cannot readily be achieved by other methods.
SURGICAL ANATOMY OF THE SUPERIOR OBLIQUE MUSCLE
Surgery to strengthen or weaken the action of the superior oblique muscle is almost always accomplished by operating on the reflected tendon. Although the muscle originates just above and medial to the optic foramen, its physiologic origin is the trochlea. After passing the trochlea, the superior oblique tendon inserts to the sclera underneath and posterolateral to the superior rectus muscle, forming an approximate 54° angle with its pretrochlear portion. Emerging from the trochlea, the tendon is cordlike and passes through the Tenon capsule. The sheath of the superior oblique tendon attaches to the fascial sheaths of the superior rectus and levator palpebrae superioris muscles. Fine connections between the tendon and the surrounding connecting tissue have implications for superior oblique surgery (e.g., these connections allow for residual superior oblique muscle function following superior oblique tenotomy).
As the superior oblique tendon approaches the medial border of the superior rectus muscle, the fibers fan out before attaching to the sclera. The anterior end of the insertion is usually located approximately 3 to 5 mm posterior to the lateral pole of the superior rectus muscle insertion, while the posterior end of the insertion lies 13 to 14 mm from the superior rectus muscle insertion. The width of the concave insertion is approximately 11 mm. These measurements, however, are highly variable.16 A superior vortex vein penetrates the globe near the posterolateral edge of the insertion, which needs to be identified and avoided if the tendon is disinserted
Connective tissue binds the superior oblique tendon to the overlying superior rectus muscle.17 This frenulum allows the superior oblique tendon to move with the superior rectus muscle and limits the amount that each muscle can be moved independently. Jampolsky18 suggested that large recessions and any resections of the superior rectus muscle should involve severing of this frenulum. Similarly, the frenulum should be transected during superior oblique recession or disinsertion to allow for maximal weakening.19
SUPERIOR OBLIQUE STRENGTHENING PROCEDURES
INDICATION: SUPERIOR OBLIQUE MUSCLE PALSY
The superior oblique muscle may need to be strengthened to correct cyclovertical strabismus in the setting of a clinically underacting muscle. The main indication for superior oblique muscle strengthening is congenital or acquired superior oblique muscle palsy. Less frequently, strengthening may be helpful to treat residual inferior oblique muscle overaction and V-pattern strabismus after inferior oblique muscle weakening in patients with persistent underaction of one or both superior oblique muscles.
Surgery to correct unilateral, congenital superior oblique muscle palsy is the single most common indication for superior oblique muscle strengthening. The underlying cause has traditionally been thought to be dysfunction of the fourth (trochlear) cranial nerve. Patients with unilateral superior oblique muscle palsy typically present with an incomitant hypertropia characterized by elevation of the affected eye in adduction and overaction of the ipsilateral inferior oblique muscle. This diagnosis is normally supported (but not diagnosed) using the Parks20 three-step test, usually with associated excyclotropia of the ocular fundus. Compensatory torticollis is present in approximately 75% of cases, with the face turn or head tilt directed toward the opposite shoulder.21,22 This is often first noted when the child begins to walk. However, the presence of a vertical deviation in primary gaze position may be overlooked if the physician fails to evaluate ocular alignment with the child’s head held erect. Chronic torticollis can result in asymmetric facial development and postural plagiocephaly (Fig. 86-1).23,24,25 This deformity manifests as hypoplasia of the face on the side toward which the head is tilted (contralateral to the palsied muscle).26 It is not known whether early strabismus surgery can prevent or reverse this deformity. The mechanisms that lead to plagiocephaly from superior oblique muscle palsy are uncertain; in fact, plagiocephaly from coronal suture synostosis can result in superior oblique palsy and a clinical picture of ocular torticollis.27 Some authors believe that proper head positioning during sleep is more important than performing early surgery in preventing the facial asymmetry.28 Bilateral superior oblique muscle palsy is much less common and occurs most frequently after head trauma, but occasionally occurs on a congenital basis associated with horizontal strabismus. In children, bilateral superior muscle palsy is much more common than unilateral palsy following trauma and may be occult.29,30,31 However, primary overaction of the inferior oblique muscles is common in strabismic children and may be a source of diagnostic confusion. This latter entity can usually be distinguished from bilateral superior oblique muscle palsy by its association with horizontal strabismus (usually esotropia) in primary gaze position, a large V-pattern (which is most pronounced between primary position and up gaze), and a negative result to the Bielschowsky head tilt test. Although bilateral superior oblique muscle palsy may also present with a V pattern, it is usually smaller in magnitude and characterized by an esotropia in down gaze rather than an exotropia in up gaze. These patients often adopt a compensatory chin-down position to facilitate fusion and/or avoid diplopia. The preoperative diagnosis of bilateral superior oblique muscle palsy can be confirmed with intraoperative traction testing or direct assessment of superior oblique tendon laxity after surgical retrieval.32,33
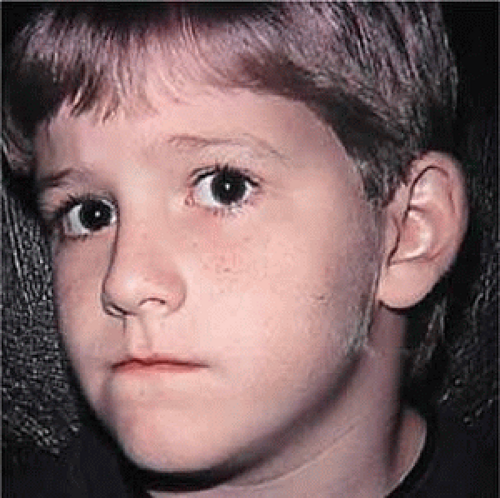 Figure 86.1. An 8-year-old boy with postural plagiocephaly associated with congenital left superior oblique muscle palsy. Note the right-sided atrophic facial development from chronic torticollis. |
Clinically subtle, bilateral superior oblique muscle palsy can usually be distinguished from a strictly unilateral palsy by a smaller than expected hyperdeviation in primary gaze position accompanied by reversal of the hypertropia in the field of action of the apparently normal superior oblique muscle or on the Bielschowsky head tilt test. Assessing the oblique fields of gaze for a reversal of the hypertropia is essential to detecting bilaterality in some cases.31
If closed head trauma can be excluded by history, the diagnosis of congenitally absent or hypoplastic superior oblique muscles or tendons (alone or combined) should be considered, especially in patients with other craniofacial anomalies.4 Computed imaging studies of the orbits may demonstrate attenuation or absence of the superior oblique muscle.34,35
Treatment for congenital superior oblique muscle palsy can generally be delayed until after age 1 year. This is fortunate, since detailed prism and cover measurements can be difficult or impossible to obtain in young children. Fusion is usually preserved in children who exhibit torticollis, and the risk of developing suppression and amblyopia is low.21 However, children with clinically apparent superior oblique palsy at a young age may have worse sensory outcomes.3 Acquired superior oblique palsy, usually a result of trochlear nerve injury associated with closed head trauma, should not be surgically treated for at least 6 months after onset or until spontaneous improvement has ceased.36
The main indications for corrective surgery are a manifest vertical strabismus in primary gaze or reading positions, compensatory torticollis, and diplopia. Large vertical vergence amplitudes to maintain fusion are typically present in patients with long-standing deviations of several years or more. However, motor fusional effort may cause asthenopic symptoms in these patients. Alternatively, patients may complain of loss of binocular vision, a cosmetically objectionable hypertropia, or cyclovertical diplopia when the deviation is manifest. Compensatory torticollis, to reduce or eliminate the hypertropia,37 is common and often the primary reason for ophthalmologic consultation in children. Older children and adults with acquired, bilateral superior oblique muscle palsy may complain of torsional diplopia in the absence of vertical strabismus when forced to look down or use bifocal glasses.38 Adaptations to tilting of the visual environment can occur in patients with acquired cyclotropia but are more deeply rooted in patients with congenital cyclotropia.39
To choose an appropriate operation in older children and adults, it is desirable to quantitate the vertical and horizontal alignment defects using prism and cover measurements or Maddox rod testing. When possible, these measurements should be obtained in the diagnostic gaze positions at distance and the near reading position. This task is time consuming but worthwhile, given that these measurements will influence the type and amount of surgery performed. In addition, important ancillary information can be obtained, such as the strength of vertical vergence amplitudes, a clinically significant horizontal deviation, or the presence of occult bilateral involvement. Assessment of subjective ocular torsion using the double Maddox rod or objective excyclotropia by fundus examination is often useful and helps confirm the diagnosis.
Successful management of superior oblique palsy can be achieved with various surgical approaches (Fig. 86-2).40,41,42,43,44,45,46,47 Superior oblique muscle-strengthening procedures are often performed in conjunction with surgery on other cyclovertical muscles. Their most common uses are (i) to augment ipsilateral inferior oblique muscle weakening in patients with at least 25 prism diopters (PD) of hypertropia in lateral gaze or 20 D of hypertropia in primary gaze; (ii) to augment ipsilateral superior rectus or contralateral inferior rectus muscle recession or posterior fixation in patients with increased hypertropia in down gaze; (iii) to correct excyclotropia in the presence of a small hypertropia in primary gaze position; and (iv) to improve the function of a congenitally lax or redundant tendon.48 In fact, torticollis may be difficult or impossible to eliminate in some children without a superior oblique tendon tuck or similar strengthening procedure.49
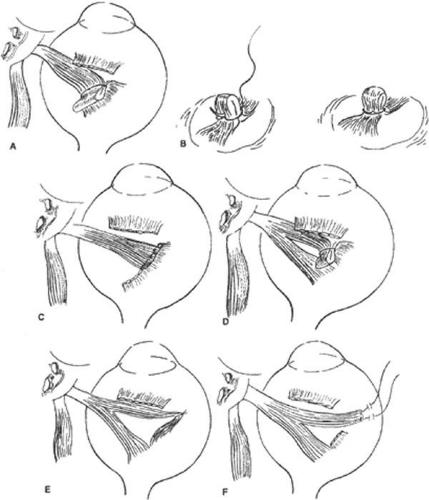 Figure 86.2. Some useful superior oblique strengthening procedures. A and B. Superior oblique tendon tuck. C. Superior oblique tendon resection. D. Anterior fiber tuck. E. Harada-Ito procedure. F. Adjustable Harada-Ito procedure. |
The Harada-Ito procedure, discussed later in this chapter, and its modifications enhance intorsion and are used to correct excyclotropia when little or no vertical misalignment in primary gaze position exists.50,51,52,53,54 Its use, therefore, is limited primarily to correcting torsional diplopia in patients with bilateral superior oblique muscle palsy.
Small horizontal deviations associated with superior oblique muscle palsy tend to resolve spontaneously after vertical realignment of the eyes. In our experience, concurrent horizontal rectus muscle surgery often (and for unknown reasons) leads to overcorrection and is usually unnecessary, unless the deviation is large.
Superior oblique muscle strengthening is occasionally performed as an isolated procedure, either as the primary procedure or, more often, after surgical undercorrection following inferior oblique muscle weakening. Indications for this approach are persistent torticollis associated with a small residual hypertropia, excyclotropia, and clinical underaction of the paretic superior oblique muscle. A superior oblique tendon tuck is an appropriate primary procedure in patients with <10 PD of hypertropia in primary gaze position, at least 5° of subjective extorsion, and little or no overaction of the ipsilateral inferior oblique muscle. This situation is normally found in unilateral or bilateral posttraumatic superior oblique muscle palsy. Congenital superior oblique muscle palsy may require both strengthening of the paretic muscle and weakening of the antagonist inferior oblique muscle.55 Perhaps the most reliable indication to operate on both muscles is a hypertropia >25 PD in the diagnostic position of gaze with the largest hypertropia, rather than primary gaze position.56
Finally, patients with direct trauma to the superior oblique tendon after penetrating injuries of the upper eyelid and orbit or eyelid surgery may have a repairable injury and should have the superior portion of the globe carefully explored and severed portions of the tendon reapproximated if technically feasible.57,58
CONTRAINDICATIONS
Contraindications to superior oblique muscle strengthening are few but important. Patients with small-angle, vertical deviations of <10 PD in the fields of action of both the ipsilateral superior oblique and inferior oblique muscles and no torsional symptoms are generally not good candidates for superior oblique muscle strengthening procedures, but can sometimes be managed successfully with inferior oblique muscle weakening or prism-fitted glasses. However, prisms are rarely appropriate in children. Patients with preoperative underaction of the ipsilateral inferior oblique muscle or concurrent Brown syndrome following trochlear injury should not undergo any procedure that could further compromise elevation of the eye. Similarly, the presence of a taut superior oblique tendon identified at the time of surgery, either by traction testing or direct inspection, should be a cause for concern. Such patients can develop symptomatic postoperative Brown syndrome following minimal shortening of the superior oblique tendon.32,48,56,59,60,61 (Our only tuck takedown over 3 decades of clinical practice was required in a patient with posttraumatic superior oblique muscle palsy who had only 4 mm of tendon tuck performed!) Finally, the absence of excyclotropia or vertical incomitance in lateral gaze should prompt the surgeon to consider operating on alternative muscles. This is because superior oblique muscle strengthening typically produces between 5° and 10° of intorsion in primary gaze position and has its greatest vertical effect in adduction. Although clinically important postoperative Brown syndrome is uncommon, many patients have a mild, long-term elevation deficiency in the operated eye, particularly if the ipsilateral inferior oblique muscle has also been weakened. They often report vertical diplopia in extreme up gaze, which might pose problems in certain occupations (e.g., pilot, auto mechanic, electrician) or athletic activities requiring a full field of single binocular vision.
SURGICAL PROCEDURES
The superior oblique tendon tuck is a type of folding, or plication62 (from Latin plicare, to fold), the most frequently performed superior oblique muscle strengthening procedure. It is almost always performed unilaterally in patients with congenital superior oblique muscle palsy or acquired paresis in which tendon laxity is demonstrated by intraoperative traction testing.32,33 Superior oblique tendon advancement or resection may be used in lieu of a tendon tuck, although these procedures are technically more difficult and less reversible. The Harada-Ito procedure is usually performed bilaterally and is generally reserved for patients with acquired, bilateral superior oblique palsy to correct torsional diplopia.60
Tendon Tuck
To perform the procedure, either general anesthesia or local anesthesia with intravenous sedation may be selected. Following anesthesia, it is often helpful to assess tendon laxity by performing an exaggerated traction test.32,33,63 A normal superior oblique tendon can be differentiated from a lax tendon when the globe is rotated upward, inward, and retropulsed into the orbit (Fig. 86-3).32
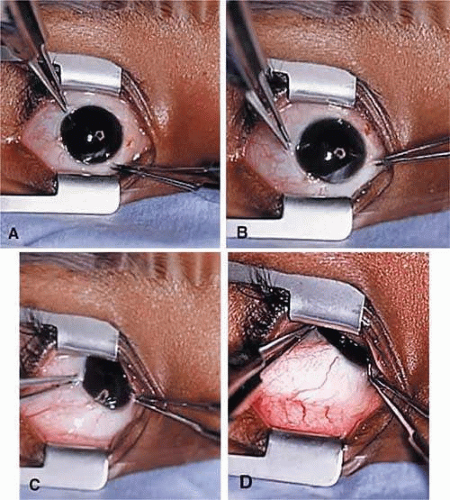 Figure 86.3. A through C. Exaggerated torsional traction test performed in a patient with congenital right superior oblique muscle palsy. D. The right superior oblique tendon could not be felt as the right eye was elevated, adducted, and retropulsed into the orbit. |
The superior oblique tendon tuck is best performed near the tendon’s insertion as described by McLean.64 The surgical procedure is performed through a superior temporal cul-de-sac approach (Fig. 86-4). With the globe depressed, an incision is made through the conjunctiva and Tenon fascia just temporal to the lateral border of the superior rectus muscle and parallel to the corneoscleral limbus. The superior rectus muscle is engaged on a muscle hook and the globe adducted and positioned in maximal depression. The lateral rectus muscle may also be used to assist positioning the globe. Using two small muscle hooks, the conjunctival incision is opened posteriorly in a triangular fashion. The lateral border of the superior rectus muscle is elevated and displaced medially. The globe is then examined for the glistening white fibers of the superior oblique tendon running flush against the sclera and directed anteromedially. The anterior portion of the reflected tendon typically inserts under the lateral border of the superior rectus muscle, 3 to 5 mm posterior to its insertion. However, this location may vary, and anatomic anomalies are common (Fig. 86-5).16,48,63,64,65 Inexperienced surgeons have mistaken the lateral portion of the tendinous insertion of the superior rectus muscle for the superior oblique tendon (Fig. 86-6).66 However, the superior rectus muscle travels toward the orbital apex and contains prominent anterior ciliary blood vessels, whereas the superior oblique tendon is directed toward the trochlea and is usually avascular. In addition, direct traction on the superior oblique tendon can easily be palpated at the trochlea by pressing a finger over the eyelid in the superior nasal quadrant of the orbit.14 This is a reliable sign that the tendon (and not some other structure) has been engaged on the muscle hook.
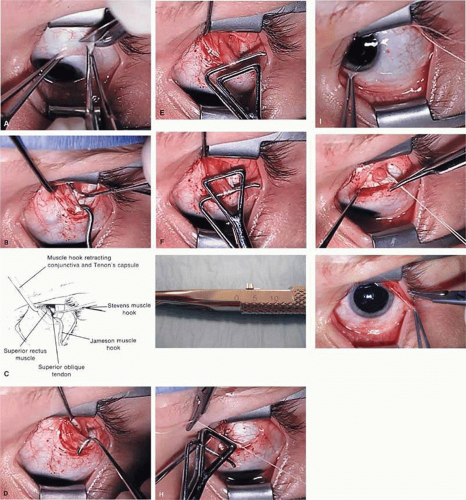 Figure 86.4. Superior oblique tendon tuck procedure in the left eye. A. A conjunctival incision is made temporal to the insertion of the superior rectus muscle. B and C. With the superior rectus muscle engaged on a Jameson muscle hook, the globe is held in maximal depression and a Stevens tenotomy hook is passed under the superior oblique tendon near its scleral insertion. D. The superior oblique tendon is retrieved from the orbit, and tendon laxity is assessed. E. The tendon is removed from the muscle hook and placed on a Bishop tendon tucker. F. The tucker is tightened until snug. G. The amount of tendon shortening (in mm) can be read directly on the shaft of the tucker. H. Redundant tendon is sewn to itself with a 5-0 braided Dacron suture forming a provisional tuck. I. The tendon is released into the orbit and the amount of tendon tuck evaluated using forced duction testing. J. If satisfactory, the sutures are cut and the tendon is allowed to retract. K. The conjunctival incision is closed at the surgeon’s option. |
 Figure 86.5. Anomalies of the superior oblique muscle. A. Superior oblique tendon (on Stevens tenotomy hook) inserting anomalously on the surface of the superior rectus muscle (in Green muscle hook). B. Absent superior oblique tendon in a patient with apparent congenital right superior oblique muscle palsy. The superior rectus muscle has been detached from the globe. |
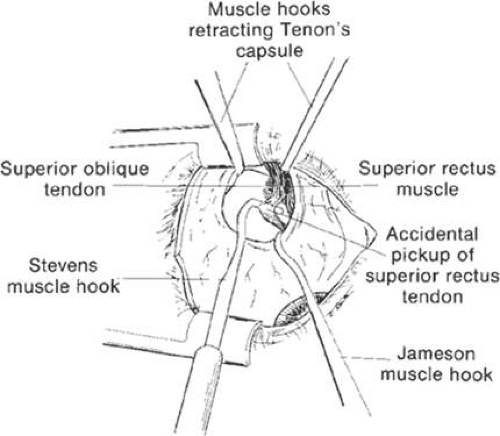 Figure 86.6. During a temporal conjunctival approach, the lateral portion of the superior rectus muscle tendon can be confused with the superior oblique tendon. |
After the superior oblique tendon has been positively identified, it is gathered on a Stevens tenotomy or other muscle hook with a small tip. This maneuver is most readily accomplished by passing the hook over the tendon with its tip parallel to the sclera and pointed medially. Direct visualization of the tendon is essential, in that blind sweeping can be hazardous. A superior temporal vortex vein usually exists near the posterior insertion of the superior oblique tendon, and the optic nerve is within reach. In addition, it is important to avoid passing the muscle hook into orbital fat because its release into the sub-Tenon space predisposes the eye to develop an adherence syndrome postoperatively.67
The superior oblique tendon is drawn forward through the surgical wound, and attachments to the Tenon fascia and the superior rectus muscle are cut. A second pass of the muscle hook helps ensure that no fibers have been missed. Gross assessment of tendon laxity is then performed. A lax tendon requires a greater amount of tuck, whereas a normal tendon should be approached with caution, and a taut tendon should not be shortened at all.56 A Bishop tendon tucker is helpful to control the isolated tendon and permits the surgeon to quantitate the amount of tendon shortening conveniently. The tendon is drawn in the tucker until snug but not tight. The loop of tendon is then sewn to itself using a nonabsorbable suture such as 5-0 braided Dacron. After this provisional tuck has been completed, the tendon is released into the orbit and a traction test is performed with the eye positioned in maximum adduction. It has been our experience that the ideal tuck results when the amount of tendon shortening produces its first resistance to elevation as the inferior limbus crosses an imaginary line between the medial and lateral canthus (Fig. 86-7).45,55,56 Care must be taken not to retropulse the globe into the orbit, because this exaggerates the duction limitation. An average tendon shortening of approximately 11 mm is required in congenital superior oblique muscle palsy (lax tendon) and 8 mm in acquired palsy (normal tendon).56 However, the optimum amount of tuck does not necessarily correlate with the size of the hypertropia in primary gaze position, and intraoperative titration is essential. If the initial tuck is too tight or too loose based on results of traction testing, the tendon is retrieved from the orbit and the tuck is adjusted (Fig. 86-8). The final tie-off is performed by passing the suture through and around the superior oblique tendon a second time, after which it is tied securely. This minimizes the potential for tendon slippage through the tuck and provides additional security should a suture loop fail postoperatively. It is not necessary to sew the redundant tendon to the sclera. Conjunctival closure is performed at the surgeon’s discretion. One or two interrupted sutures of 6-0 plain catgut is well tolerated and prevents the conjunctiva from gaping open postoperatively.
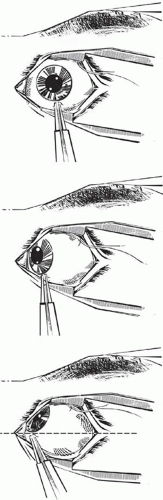 Figure 86.7. Drawing of the intraoperative traction test for titrating a superior oblique tendon tuck (left eye shown). A. The eye is grasped near the limbus at approximately 5:30 o’clock with a toothed forceps. B. The globe is positioned in 30°–40° adduction. C. The globe is then elevated against the superior oblique tendon without retropulsion. The first resistance to elevation should be felt as the inferior limbus crosses an imaginary line (dashed line) between the medial and lateral canthus. |
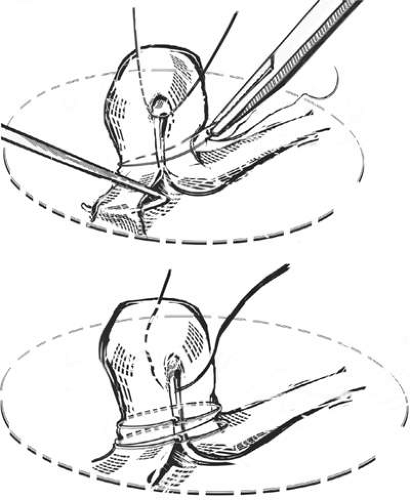 Figure 86.8. Simple technique of adjusting a tuck judged too loose or too tight. A. An excessive tuck can be loosened by pulling the looped tendon apart with a muscle hook while simultaneously working the provisionally tied nonabsorbable (e.g., 5-0 braided Dacron) suture away from the sclera with a needle driver. Once adjusted, the tendon is then secured tightly with a second wrap of suture around and through the tendon. A silk traction suture is shown through the tendon loop and allows easy release and recovery from the orbit. B. An inadequate tuck is tightened by placing a second wrap of suture around and through the tendon closer to the sclera. The original suture is not removed. |
Tendon Imbrication
This procedure is similar to the superior oblique tendon tuck, except that a nonabsorbable suture is secured to the tendon 6 to 9 mm from its insertion and then passed through the sclera just beyond the insertion.68 Pulling these sutures tight folds the tendon over onto itself (imbrication, from Latin imbricare, to cover with tiles) and advances the midportion of the tendon.62 Plication shares reversibility with the superior oblique tendon tuck, although it alters the normal anatomic insertion of the tendon and is more difficult to adjust intraoperatively.
Tendon Resection/Advancement
The superior oblique tendon can be resected or advanced in a manner similar to that used for rectus muscles (Fig. 86-2C). However, the long and fanlike tendinous insertion makes this technique more challenging, even with optimal exposure, and typically results in narrowing and some anterior transposition of the scleral insertion. Furthermore, this procedure is less easily reversible than superior oblique tendon tuck and other procedures that do not involve tendon disinsertion. Therefore, superior oblique tendon resection is rarely, if ever, selected by most surgeons.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


