Category
Subtypes
Vascular tumors
Pyogenic granuloma
Racemose malformation
Capillary hemangioma
Hemangiopericytoma
Cavernous hemangioma
Kaposi’s sarcoma
Acquired sessile hemangioma
Lymphangiectasia
Varix
Lymphangioma
Malignant hemangioendothelioma
Fibrous tumors
Fibroma
Nodular fasciitis
Benign fibrous histiocytoma
Malignant fibrous histiocytoma
Neural tumors
Neurofibroma (localized)
Neurofibroma (diffuse)
Schwannoma (neurilemoma)
Granular cell tumor
Histiocytic tumors
Xanthoma
Juvenile xanthogranuloma
Reticulohistiocytoma
Myxoid tumors
Myxoma
Myogenic tumors
Rhabdomyosarcoma
Lipomatous tumors
Lipoma
Herniated orbital fat
Liposarcoma
Lymphoproliferative tumors
Benign reactive lymphoid hyperplasia
Lymphoma
Leukemic infiltrates
Choristomas
Dermoid
Dermolipoma
Osseous choristoma
Lacrimal gland choristoma
Complex choristoma
Metastatic tumors
Secondary tumors
19.2 Vascular Tumors
Vascular tumors of the conjunctiva are uncommon, and with the exception of Kaposi’s sarcoma, most are benign lesions that have no malignant potential. According to one large series [1], the most common conjunctival vascular lesions are lymphangioma/lymphangiectasia and pyogenic granuloma.
19.2.1 Pyogenic Granuloma
The term “pyogenic granuloma” is a misnomer, since it is neither pyogenic nor granulomatous. It is granulation tissue, although some consider it as a polypoid form of acquired capillary hemangioma [2]. Pyogenic granuloma is a fibrovascular response to tissue insult such as surgical or nonsurgical trauma or inflammation, although spontaneous pyogenic granulomas have also been reported. Pyogenic granuloma is commonly observed in the conjunctiva after chalazion surgery, strabismus surgery, excision of conjunctival lesions, and in the anophthalmic socket following enucleation, considered as an aberrant wound-healing response.
19.2.1.1 Clinical Features
Pyogenic granuloma has been reported in every part of the conjunctiva and even in the limbus and the cornea, mostly following corneal epithelial defect [3]. Pyogenic granuloma appears as a fleshy, elevated, red, often pedunculated, richly vascularized mass (Fig. 19.1a).
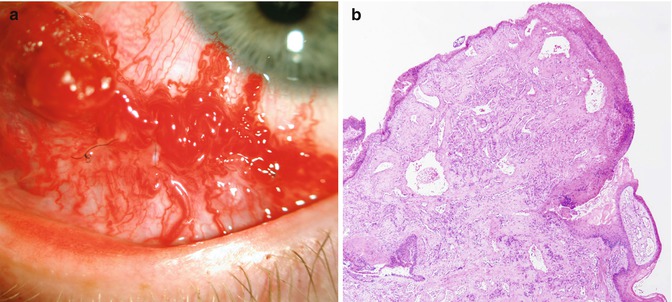
Fig. 19.1
Pyogenic granuloma. A 31-year-old man with a 3-week history of a rapidly growing recurrent conjunctival vascular growth in the inferonasal conjunctival fornix. Note prominent vascularity (a). Polypoid lesion with lobular pattern of capillary proliferation. The vessels are variably dilated (b) (Original magnification ×4)
19.2.1.2 Histopathologic Features
Pyogenic granuloma is composed of granulation tissue with marked chronic inflammation with lymphocytes, plasma cells, neutrophils, and proliferation of small, mostly capillary-sized blood vessels (Fig. 19.1b).
19.2.1.3 Treatment
Pyogenic granuloma often responds to topical corticosteroids when diagnosed early, but many cases require surgical excision.
19.2.2 Capillary Hemangioma
Capillary hemangioma appears during early infancy, and like its counterpart in the skin, may grow over several months and then regress spontaneously within several years.
19.2.2.1 Clinical Features
Capillary hemangioma is a distinct or diffuse red, elevated conjunctival lesion that can occur anywhere in the conjunctiva. It can be an isolated lesion or in association with an eyelid or orbital capillary hemangioma.
19.2.2.2 Histopathologic Features
Similar to capillary hemangiomas in other locations, it shows numerous capillary channels and proliferation of endothelial cells.
19.2.2.3 Treatment
Usually no treatment is needed and the child should only be observed. There are rare cases, especially when the lesion is large and potentially amblyogenic, in which surgical excision or local or systemic corticosteroids are employed [1, 4]. There is no experience yet in treating conjunctival capillary hemangioma by beta-blockers.
19.2.3 Cavernous Hemangioma
Cavernous hemangioma presents as a red or blue multiloculated lesion in the deep conjunctival stroma in children [4]. This lesion is usually isolated but may be associated with syndromes [1]. It may cause recurrent subconjunctival hemorrhage [5]. Histologically, similar to such lesions in other locations, it is composed of large blood-filled spaces, lined by endothelial cells and separated by fibrous septa. It can be managed by surgical excision.
19.2.4 Acquired Sessile Hemangioma
Shields et al. [6] described vascular lesions that consist of a sessile network of convoluted blood vessels immediately beneath the conjunctival epithelium.
19.2.5 Varix and Racemose Hemangioma
19.2.5.1 Conjunctival Varix
Varix and racemose hemangioma are rare vascular malformations of the conjunctiva. Varix is a mass of dilated venous channels that may range from a single channel to complex venous channels. Many of them are anterior extensions of orbital varix. The color ranges from blue-red to black [1]. It is usually movable and not fixed to the sclera. Thrombosis is frequent. Some consider it to be in the spectrum of lymphangioma. Management should be conservative, by observation and symptomatic treatment. When it is symptomatic, surgical excision should be considered, although the surgeon should bear in mind the risk of prolonged bleeding [1, 3].
19.2.5.2 Conjunctival Racemose Hemangioma
Conjunctival racemose hemangioma is a lesion of dilated arteries and veins communicating directly without a capillary bed between them. It appears as a loop of dilated vessels in the conjunctival stroma. It should be managed conservatively by observation. Wyburn-Mason syndrome should be ruled out in such cases [4].
19.2.6 Hemangiopericytoma
Hemangiopericytoma is very rare in the conjunctiva. It appears as an elevated pedunculated red mass. Histologically, it is a solid tumor composed of spindle-shaped pericytes and small blood vessels [7]. Treatment is by complete surgical excision with tumor-free margins and close follow-up.
19.2.7 Kaposi’s Sarcoma
Prior to the AIDS era, Kaposi’s sarcoma in general, and in the conjunctiva in particular, was a rare tumor that mainly affected elderly and immunosuppressed patients. Since the eruption of the AIDS epidemic, this malignant tumor is diagnosed much more frequently in AIDS patients. Sometimes conjunctival Kaposi’s sarcoma is the first sign of AIDS [8]. However, in recent years, it has been diagnosed less frequently because of the more effective treatment of AIDS in developed countries.
19.2.7.1 Clinical Features
Kaposi’s sarcoma appears as a single isolated or multiple confluent red painless conjunctival mass.
19.2.7.2 Histopathologic Features
The tumors are composed of malignant spindle-shaped cells with elongated oval nuclei, well-formed capillary channels, and vascular slits containing blood but no definite endothelial lining.
19.2.7.3 Treatment
Localized tumors can be excised surgically, with or without the addition of cryotherapy. However, Kaposi’s sarcoma is responsive to chemotherapy and low-dose radiation therapy [9]. Treatment using intralesional interferon alpha-2b or intralesional mitomycin C has been reported.
19.3 Lymphangiectasia and Lymphangioma
19.3.1 Lymphangiectasia
When lymphatic channels in the conjunctiva are dilated and prominent, the condition is called “lymphangiectasia.”
19.3.1.1 Clinical Features
Conjunctival lymphangiectasia can either be unilateral or bilateral with focal or diffuse bulbar chemosis [10]. As a result of the communication with conjunctiva veins, these dilated channels may be filled with blood and if so are termed “hemorrhagic lymphangiectasia” (lymphangiectasia hemorrhagica conjunctivae of Leber) [11]. The surrounding conjunctiva appears edematous, and occasionally associated subconjunctival hemorrhage is present. This phenomenon can occur spontaneously or after trauma or inflammation. Congenital cases have been reported.
19.3.1.2 Histopathologic Features
The lesion shows markedly dilated lymphatics, which may be filled with blood, partially surrounded by scattered inflammatory cells. The phenomenon is intermittent, with resolution between episodes.
19.3.1.3 Treatment
Usually no treatment is required, although surgical excision without or with amniotic membrane transplant or conjunctival autograft has been described [10]. Recently, treatment of symptomatic conjunctival lymphangiectasia by liquid nitrogen chemotherapy [12] and high-frequency radio wave electrosurgery has been reported [13].
19.3.2 Conjunctival Lymphangioma
Conjunctival lymphangioma is a benign tumor of the lymphatic vessels that usually appears in the first decade of life. It can occur as an isolated conjunctival lesion but more often represents a superficial component of orbital lymphangioma.
19.3.2.1 Clinical Features
Conjunctival lymphangioma appears as a multiloculated lesion composed of dilated cystic spaces. These spaces may contain clear fluid, but often part of them contain blood and are called “chocolate cysts.”
19.3.2.2 Histopathologic Features
Conjunctival lymphangioma shows dilated lymphatic channels filled with lymph and/or blood, lined by endothelium, and separated by thin walls.
19.4 Fibrous Tumors
19.4.1 Fibroma
19.4.1.1 Clinical Features
19.4.1.2 Histopathologic Features
The tumor is composed of compact fibroblasts and collagen. Rare variants such as elastofibroma oculi, giant cell angiofibroma, and solitary fibrous tumor have been described [18].
19.4.1.3 Treatment
Conjunctival fibroma is treated by complete surgical excision.
19.4.2 Benign and Malignant Fibrous Histiocytoma
Fibrous histiocytoma (FH) of the conjunctiva can be benign, locally aggressive, or malignant [19]. FH generally occurs in adults, but a case of FH in a child with xeroderma pigmentosum has also been reported [20].
19.4.2.1 Clinical Features
Conjunctival FH appears as an amelanotic mass that can range from a well-circumscribed mass to a diffuse one. It often presents in the limbus (Fig. 19.2) [21].
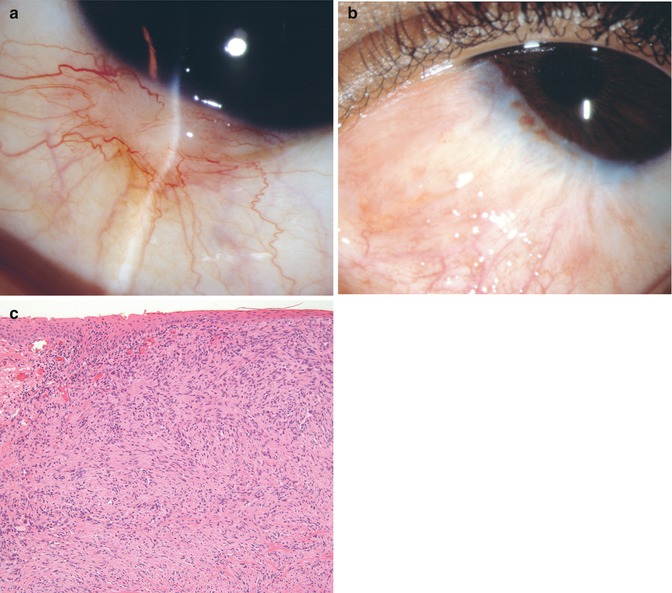
Fig. 19.2
A 10-year-old black boy presented with a limbal lesion that was excised about 2 months previously. The lesion recurred (a). Further excision with cryotherapy was performed. For yet another recurrence, excision was repeated. Histopathology revealed a moderately cellular spindle cell lesion composed of bland spindle cells arranged in a vaguely storiform configuration. Entrapped collagen bundles are witnessed at the periphery of the lesion, and there are scattered inflammatory cells, mostly lymphocytes (b, Hematoxylin and eosin-stain ×40). A final diagnosis of benign fibrous histiocytoma (extension to margin) was made. Repeat cryotherapy was performed to the surgical site. Over a 6-year follow-up, there was no recurrence and the patient maintained normal visual acuity (c) (Courtesy of David Meisler, MD and Thomas Plesec, MD, Cleveland Clinic, Ohio)
19.4.2.2 Histopathologic Features
FH shows a mixture of spindle-shaped fibroblasts, often arranged in storiform pattern, and lipid-laden histiocytes. Conjunctival FH with benign histological appearance may show a malignant clinical course. Malignant FH of the conjunctiva is extremely rare and shows marked pleomorphism, many mitotic figures, and multinucleated giant cells. Malignant FH is accepted as originating from primitive mesenchymal cells with the capacity to differentiate along either or both histiocytes and fibroblasts [22]. Malignant FH can metastasize to regional lymph nodes and hematogenously to distant organs, causing death.
19.4.2.3 Treatment
While benign FH can be treated by complete surgical excision, malignant FH should be treated by radical surgery that may include exenteration and radical dissection of regional lymph nodes.
19.4.3 Nodular Fasciitis
Nodular fasciitis is a benign rare nodular tumor of unknown cause that can occur at any age.
19.4.3.1 Clinical Features
Nodular fasciitis appears as a solitary white episcleral enlarging nodule at the limbus or over the sclera anterior to the insertion of one of the rectus muscles and can cause discomfort or pain. The nodule may grow quickly and show signs of inflammation. It is thought to originate from the Tenon’s capsule [23].
19.4.3.2 Histopathologic Features
The lesion tends to be round or oval and is not encapsulated. It is composed of bundles of fibroblasts that vary in configuration from spindle to stellate. There is a variable amount of intercellular myxoid ground substance interspersed with slit-like vascular spaces or capillaries and scanty infiltration of chronic inflammatory cells. Numerous mitotic figures can lead to its being misdiagnosed as a sarcoma.
19.4.3.3 Treatment
The prognosis is excellent and complete excision is usually sufficient therapy, although recurrence can occur.
19.5 Neural Tumors
19.5.1 Neurofibroma
Neurofibroma is a peripheral nerve sheath tumor that can occur in the conjunctival stroma as a solitary circumscribed, or as a diffuse or plexiform, tumor [24]. The solitary type usually is not associated with systemic disease, while the latter is generally associated with neurofibromatosis type 1 (von Recklinghausen’s disease).
19.5.1.1 Clinical Features
The solitary neurofibroma is a pink-yellow growing mass, while the plexiform neurofibroma is diffuse.
19.5.1.2 Histopathologic Features
Neurofibroma demonstrates benign proliferation of Schwann cells, axons, and endoneural fibroblasts, which may be difficult to differentiate from other spindle cell tumors.
19.5.1.3 Treatment
Solitary tumors are usually treated by complete surgical excision. Plexiform neurofibroma may be difficult to excise completely. In such cases, debulking of the tumor is performed.
19.5.2 Neurilemmoma (Schwannoma)
Neurilemmoma (Schwannoma) of the conjunctiva is a benign rare ocular tumor that can arise from any part of the conjunctiva – bulbar, forniceal, or palpebral [25].
19.5.2.1 Clinical Features
Neurilemmoma (Schwannoma) appears as a pink-yellow elevated mass in the conjunctival stroma.
19.5.2.2 Histopathologic Features
The tumor is the result of proliferation of Schwann cells of a peripheral nerve sheath and is composed of spindle cells that may be arranged in Antoni A pattern or Antoni B pattern.
19.5.2.3 Treatment
Conjunctival neurilemmoma is treated by complete excision within the tumor capsule. Incomplete excision may lead to recurrence. Malignant Schwannoma has not been recorded in the conjunctiva.
19.5.3 Granular Cell Tumor
Conjunctival granular cell tumor, known also as myoblastoma, is a very rare benign tumor of disputed origin [26]. After being thought of striated muscle origin, the recent suggestion is that it is of neural derivation, probably from Schwann cells.
19.5.3.1 Clinical Features
The tumor appears as a pink, elevated smooth mass of the conjunctival stroma, indistinguishable from other well-circumscribed tumors.
19.5.3.2 Histopathologic Features
The tumor is composed of groups and cords of cells with small round to oval nuclei and voluminous cytoplasm containing fine eosinophilic granules.
19.5.3.3 Treatment
The tumor should be completely excised.
19.6 Histiocytic Tumors
19.6.1 Xanthoma
Conjunctival xanthoma appears as a yellow subepithelial mass on epibulbar surface. In a case of xanthoma disseminatum, in which multiple lesions are found, lesions have been described in the limbus of both eyes [27]. Histopathologically, the lesion shows subepithelial infiltrate of lipid-laden histiocytes, eosinophils, and Touton giant cells.
19.6.2 Xanthogranuloma
19.6.2.1 Clinical Features
Conjunctival involvement in juvenile xanthogranuloma usually occurs as a solitary orange-pink stromal mass, usually near the limbus (Fig. 19.3) [28]. Sometimes associated systemic findings may not be present [28]. Bilateral conjunctival xanthogranuloma in adults has also been recorded [29].

Fig. 19.3
Juvenile xanthogranuloma in a 5-year-old child, presenting as a congested elevated pink mass in the limbal area growing over the cornea
19.6.2.2 Histopathologic Features
The lesions show typical findings of histiocytes and Touton giant cells; in addition, lymphocytes, plasma cells, and eosinophils can be found.
19.6.2.3 Treatment
Most lesions are treated by excision. When xanthogranuloma is suspected clinically, it may be observed for spontaneous resolution or can be treated by topical or systemic corticosteroids. In resistant cases, brachytherapy has been successfully applied.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


