Fig. 10.1
Mohs’ micrographic surgery. Frozen sections are obtained from the undersurface and skin edges of the excised lesion. Locations of residual tumor are marked on a map for subsequent second stage excision
10.2.3 Sentinel Lymph Node Biopsy
In a patient with a biopsy-proven malignant eyelid lesion with demonstrated biological behavior for regional lymph node metastasis, careful evaluation of preauricular and submandibular lymph nodes is essential. An additional consideration is the use of lymphatic mapping and sentinel lymph node biopsy for early accurate staging of solid tumors exhibiting a propensity for regional nodal metastasis [6] (Chap. 11).
10.2.4 Eyelid Reconstruction
Optimum functional and cosmetic outcomes are possible if the following general principles of eyelid reconstruction are taken into consideration:
The eyelid is a bilamellar structure; the anterior lamella consists of the skin and orbicularis oculi muscle, and the posterior lamella of the tarsal plate and conjunctiva.
The anterior or posterior lamella must have its own inherent blood supply.
Provision must be made for maximal horizontal stabilization with minimal vertical tension, proper canthal fixation, and an epithelialized internal surface to face the globe [8].
Undermining should be sufficient to allow for tension-free closure.
Identification of the transverse edge of the levator aponeurosis and a knowledge of facial nerve anatomy are essential in maintaining the opening and closing functions of the eyelid.
10.3 Lower Eyelid Defects (Fig. 10.2)
Fig. 10.2
Algorithm for the repair of lower eyelid defects
10.3.1 Anterior Lamellar Deficit, Lid Margin Intact
10.3.1.1 Primary Closure
In general, anterior lamellar defects without lid margin involvement may be closed primarily if this does not induce distortion. The wound is closed in two layers using deep, interrupted 6/0 Vicryl sutures and interrupted, superficial 6/0 or 7/0 nylon or silk sutures in the skin. If insufficient anterior lamella remains, a full-thickness pentagonal wedge, including the anterior lamellar defect, may be excised with Westcott scissors. The tarsal borders should be sharp and perpendicular to the lid margin. The resulting full-thickness defect may then be closed primarily as described below.
10.3.1.2 Skin Graft
For defects that are too large to close primarily, full-thickness skin grafts from hairless areas may be employed. Possible donor sites include the ipsilateral or contralateral upper eyelid, the preauricular or retroauricular skin, and less commonly the supraclavicular fossa and the upper inner arm. In general, split-thickness skin grafts are not recommended in eyelid reconstruction [1]. If a skin graft is obtained from the upper eyelid or retroauricular area, it must be thinned of subcutaneous fat and connective tissue. The graft is then trimmed to size and sutured to the edges of the defect with interrupted 7/0 nylon or silk sutures [7].
10.3.1.3 Ellipse Sliding Flap
An elliptical sliding flap may also be used to close some anterior lamellar defects [9]. This flap, however, should not be used to reconstruct anterior lamellar defects near the lid margin because ectropion or retraction may be induced by excessive perpendicular tension. The ellipse should be oriented parallel to the relaxed skin tension lines. The long axis should be four times longer than the short axis, with the ellipse angle at approximately 30°. The flap is secured in two layers.
10.3.1.4 Myocutaneous Advancement Flap
An ideal method to address a large anterior lamellar deficit is the myocutaneous advancement flap because it provides the best tissue match with an independent blood supply (Fig. 10.3). Incision lines should be oriented horizontally and blend within naturally occurring skin creases. Planes of dissection should be determined before the undermining is advanced past the lateral orbital rim [7, 8]. The flap consists of skin and muscle and is designed to advance medially to fill an anterior lamellar defect. The creation of a myocutaneous advancement flap begins with an infralash incision that extends laterally to the canthus and arches superiorly. The key component is a tension-bearing permanent suture (4/0 Prolene) at the zygoma or the lateral orbital rim; the flap is then closed in two layers. This technique provides an anterior lamella replacement with an inherent vascular supply.
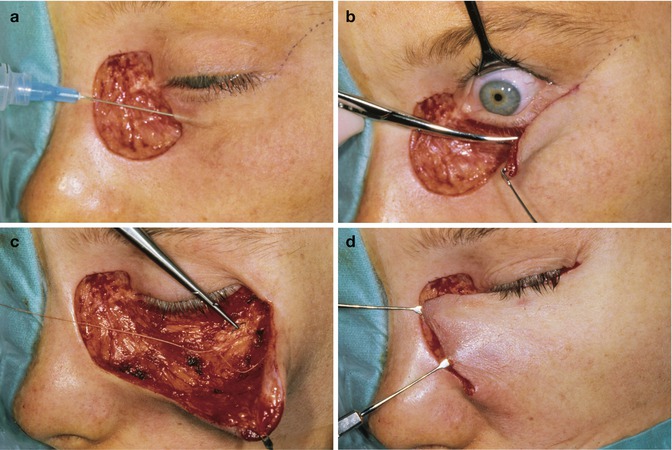

Fig. 10.3
Myocutaneous advancement flap. A large anterior lamella deficit may be repaired with a myocutaneous advancement flap because it provides the best tissue match with an independent blood supply (a). A flap of sufficient size that allows for tension-free closure is dissected from the underlying tissue (b). Proper placement of a tension-bearing permanent suture (4-0 Prolene) at the zygoma or the lateral orbital rim is important in securing the flap into position (c). Closure at the tip of the flap should be devoid of tension (d). The myocutaneous advancement flap with its inherent vascular supply now covers the anterior lamella defect (e)
10.3.2 Full-Thickness Eyelid Defect
10.3.2.1 Primary Closure
For small defects involving less than one-third of the lower eyelid margin, primary closure without lateral cantholysis is the best option. Primary layered closure provides the best tissue match, a smooth lid margin, and a continuous eyelash line. If tension is present and precludes proper lid margin reapproximation, a lateral canthotomy with inferior cantholysis may be performed to yield 5–6 mm of medial advancement of the temporal eyelid margin [7, 9].
The first step requires trimming of the eyelid defect edges. The tarsal borders should be sharp and perpendicular to the lid margin. The tissue inferior to the tarsus is cut into a wedge, forming a pentagonal-shaped defect. Direct closure may be utilized if the borders of this defect can be reapproximated without excess tension; otherwise a lateral cantholysis is needed.
To perform a cantholysis, a 4–5-mm horizontal incision through skin and orbicularis muscle is made from the lateral canthal angle toward the orbital rim. The tip of the Westcott scissors should be used to identify the lateral attachment of the lower lid, and the inferior crus of the lateral canthal tendon is cut by making a vertical incision. The most important step in primary closure of the pentagonal lid margin defect is precise approximation of the tarsal edges. Accurate vertical alignment provides most of the tension-bearing support of the wound. Following lid margin reapproximation and repair of the tarsal defect as outlined in Fig. 10.4, the anterior lamella is closed in two layers.
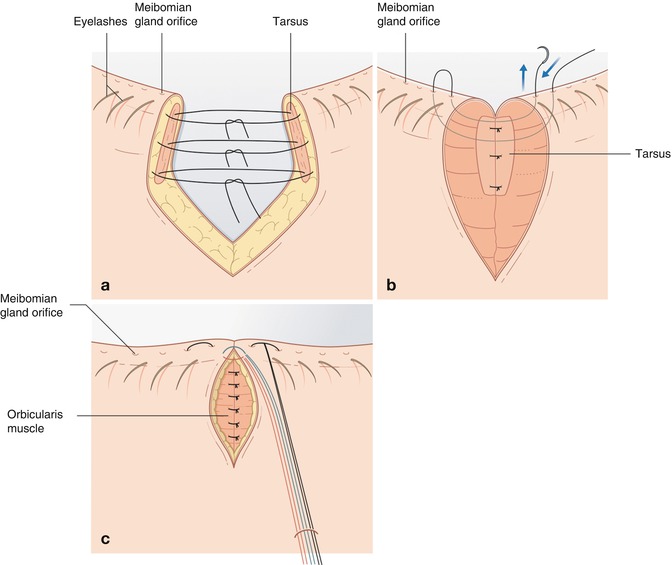
Fig. 10.4
Lid margin repair, full-thickness defect. The eyelid margin defect may be closed primarily if less than one-third of the margin is involved. An important step in primary closure of a full-thickness lid margin defect is precise approximation of the tarsal edges. Accurate vertical alignment provides the tension-bearing support of the wound. Three interrupted 5-0 Vicryl sutures are placed at partial thickness through the tarsal plate (a). The lid margin is closed with a vertical mattress suture using 6-0 silk suture which provides proper anteroposterior alignment. A vertical lid margin suture induces puckering of the wound edges to avoid notching after healing (b). Two additional sutures, one posterior and another inferior to the lashes, are placed to align the lid margin. The three 6-0 silk sutures should be left long and secured away from the wound onto the lower lid skin with a suture (c)
10.3.2.2 Semicircular Rotational Flap
A lateral semicircular rotational flap may be used to reconstruct up to two-thirds of a central lower lid defect if there is a sufficient temporal tarsal remnant. The temporal tarsal remnant and a myocutaneous flap are moved as a unit [7]. The first step is to outline a semicircle, approximately 20 mm in diameter, starting at the lateral canthal angle. The outline should arc superiorly and temporally, but not pass the lateral extent of the brow. In addition, a lateral canthotomy of the inferior crus is performed with the scissors extending to the inside of the orbital rim. The lateral lower lid and flap are moved medially until the lid margin defect may be covered and closed without tension. Once the defect is closed, the lateral canthus is reformed. Fixation of the lateral edge of the flap is needed to provide posterior and lateral vector forces so that the reconstructed lower eyelid lies in apposition with the globe. The deep edge of the flap is sutured to the inner aspect of the lateral orbital rim inferior to the superior crus using 4/0 Vicryl sutures. Finally, the conjunctival edge previously cut during the canthotomy is advanced superiorly and attached to the skin edge of the lateral lid margin with a running 7/0 Vicryl suture.
10.3.2.3 Free Tarsal Graft and Myocutaneous Advancement Flap
For larger defects where primary closure is not possible, a free tarsal graft from the ipsilateral or contralateral upper eyelid can be used for posterior lamella replacement [9]. The graft provides posterior lamellar support and a mucous membrane lining for the reconstructed lower lid. A myocutaneous advancement flap is then fashioned to provide blood supply to the free graft (Fig. 10.5). This option is most appropriate for patients whose involved eyelid is on the side of the only seeing eye or who would not be able to tolerate closure of the eyelids with a Hughes flap (see below).
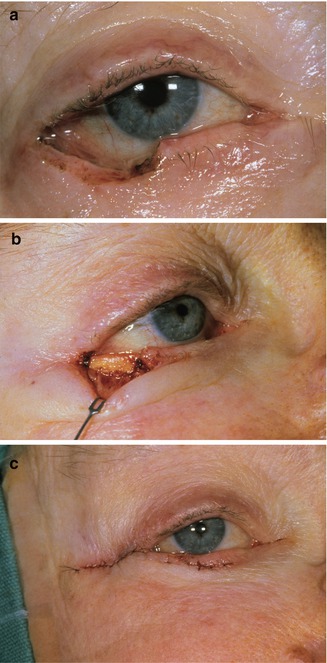
Fig. 10.5
Free tarsal graft plus myocutaneous advancement flap. A full-thickness lower eyelid defect may be repaired with a free tarsal graft for posterior lamella replacement and an overlying myocutaneous advancement flap to provide vascular support (a). The free tarsal graft harvested from either the ipsilateral or the contralateral upper eyelid provides posterior lamellar replacement (b). The myocutaneous advancement flap, fashioned in the manner of a lower eyelid blepharoplasty, provides an inherent blood supply to the underlying free tarsal graft. This figure demonstrates the key principle that either the reconstructed anterior or posterior lamella must have its own inherent vascular supply (pedicle flap), thus ensuring tissue survival and optimum surgical outcome for the patient (c)
The harvest of a free autogenous tarsal graft first involves the placement of a 4/0 silk traction suture through the central upper lid margin. The lid is everted to expose the tarsoconjunctival surface. The inferior edge of the graft is parallel to and 4 mm or more from the lid margin. The superior tarsal border determines the vertical height of the graft. The incision is made through the conjunctiva and full-thickness tarsus along the inferior and vertical edges. Dissection is used to separate the levator aponeurosis from the underlying tarsus. Mueller’s muscle and conjunctiva are cut from the superior tarsal border, leaving 2 mm of conjunctiva attached to the graft. The donor site is allowed to heal by secondary intention.
The graft is secured into the defect with the conjunctival surface in contact with the globe and the superior edge of the graft, with the conjunctival remnant along the new lid margin. The medial edges are secured with interrupted 5/0 Vicryl sutures passed at partial thickness to avoid ocular irritation. The superior edge is attached to the superior forniceal conjunctiva and the edges of Mueller’s muscle and levator aponeurosis using interrupted 6/0 Vicryl sutures. The graft may subsequently be covered with a vascularized myocutaneous advancement flap (similar to the previously described rotational flap).
10.3.2.4 Periosteal Strip and Myocutaneous Advancement Flap
The periosteal strip with myocutaneous advancement flap is an alternative to the free tarsal graft [7]. This method may be used to reconstruct the lower lid when the lateral third of the tarsus is not present. The periosteal strip may also be used in combination with other procedures for larger defects. When fashioning the periosteal strip, the skin overlying the flap is first outlined with a marking pen in a semicircle or as a cheek flap extended 1–2 cm past the lateral commissure. Once the skin–muscle flap is mobilized and reflected, the lateral orbital rim is exposed. A rectangular strip of periosteum based at the inner aspect of the rim is then formed. The strip should be 1 cm wide, angled at 45° to follow the lower lid contour. The distance from the lateral edge of the tarsal defect to the orbital rim determines the length. The fascia is dissected from the temporalis muscle and separated from the bony rim with a periosteal elevator. The strip is reflected nasally to fill the tarsal defect. The anterior periosteum lies against the globe, and the distal end is secured to the lateral border of the remaining tarsus with partial-thickness 5/0 Vicryl sutures. The strip thus provides posterior lamellar support for the reconstructed lower eyelid. The myocutaneous advancement flap is then rotated and secured to fill the anterior lamellar defect.
10.3.2.5 Free Tarsal Graft and Unipedicle Flap from the Upper Eyelid
A free tarsal graft with a unipedicle flap from the upper eyelid is another method used to close full-thickness lower eyelid defects. The free tarsal graft is first harvested. Next, a flap is harvested from excess upper lid skin and subcutaneous tissue, based at the lateral canthus (Fig. 10.6), rotated inferiorly to fill the lower anterior lamellar defect, and then closed in two layers. The unipedicle flap may leave the patient with a lump of tissue at the lateral canthus. If necessary, a second procedure may be undertaken 6–8 weeks later to thin the base of the flap and remove this excess tissue.
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
