Fig. 5.1
Squamous cell carcinoma of the upper lid (a) and lower eyelid (b) presenting as an irregular, elevated lesion with masses of keratin
Patients with SCC tend to have other tumors of the skin, including intraepidermal carcinoma (Bowen’s disease), senile keratosis, and basal cell carcinoma [1]. Squamous intraepidermal carcinoma (Bowen’s disease) represents full-thickness involvement of the epidermis by neoplastic cells (carcinoma in situ) with a relatively high risk of progression to invasive SCC [10]. Its clinical manifestation is of a persistent and slowly enlarging erythematous, scaly, or crusted lesion with a sharp, irregular outline [1, 12].
5.6 Histopathologic Features
5.6.1 Pathogenesis
5.6.2 Evolution
SCC of the eyelid usually begins with an early epithelial phase referred to as actinic keratosis (senile keratosis, solar keratosis), with subtotal replacement of the epidermis by atypical cells (intraepithelial squamous dysplasia). Intraepithelial squamous cell carcinoma or squamous cell carcinoma in situ is diagnosed when there is complete disorganization of the epidermis, with numerous atypical cells that are rounded, large, and with homogeneous, eosinophilic cytoplasm. Invasion of the dermis is the hallmark for the histopathologic diagnosis of invasive SCC (Fig. 5.2) [1].
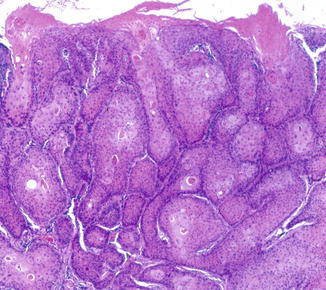
Fig. 5.2
Invasive well-differentiated squamous cell carcinoma showing invasion of the dermis by tumor polygonal cells that vary in size and staining properties
5.6.3 Light Microscopic Features
The invading cells show different degrees of differentiation leading to variable histologic features. In well-differentiated tumors the cells are polygonal, with abundant acidophilic cytoplasm and prominent hyperchromatic nuclei that vary in size and staining properties. Characteristic findings are of abnormal keratinization with dyskeratotic cells and keratin pearls and intercellular bridges. Poorly differentiated lesions show an increased degree of cellular anaplasia, with irregularly shaped and sized cells, enlarged nuclei, abnormal mitoses, little or no evidence of keratinization, and loss of intercellular bridges (Fig. 5.3).
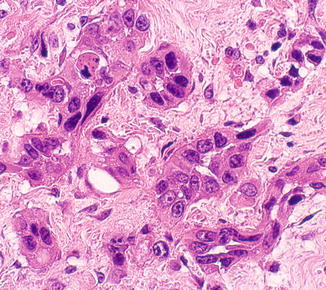
Fig. 5.3
Poorly differentiated squamous cell carcinoma showing cellular anaplasia with irregularly shaped and sized cells, enlarged nuclei, and no evidence of keratinization
5.7 Diagnostic Evaluation
Because of its variable clinical presentation, biopsy and histological examination are required for an accurate diagnosis [1]. Examination of the face or extremities for other types of premalignant lesions may aid in the diagnosis [1, 11]. The diagnosis of perineural spread and orbital invasion may be confirmed with appropriate imaging techniques.
5.8 Differential Diagnosis
5.9 Treatment
5.9.1 Preventive
Prevention by minimizing sun exposure, especially in childhood and adolescence, remains of prime importance in minimizing the morbidity and mortality associated with SCC.
5.9.2 Therapeutic
The main treatment modality used for eyelid SCC is surgical excision, with microscopic monitoring of the margins or Mohs’ microsurgery. A variety of other forms of therapy were suggested, such as radiation therapy, cryotherapy, chemotherapy, curettage with carbon dioxide laser, photodynamic therapy, and treatment with retinoids or
α-interferon. When used alone, these therapies have high recurrence rates, which are not acceptable for SCC of the eyelid, where recurrent tumors can be more aggressive and invasive. However, they may be appropriate for patients who cannot tolerate or who decline surgery [11].
5.9.2.1 Surgery
Only surgical excision with monitoring of the margins, using either a frozen-section, or a paraffin-section control, or Mohs’ micrographic surgery is an acceptable treatment option for periocular SCC [1, 2, 11, 12]. The treatment of choice for secondary orbital invasion of SCC is orbital exenteration [1, 10].
5.9.2.2 Sentinel Lymph Node Biopsy
The presence of regional lymph node metastases is the single most important prognostic factor for most solid neoplasms, and complete lymph node dissection with pathologic examination of a cross section of a lymph node is considered the gold standard in staging patients for adjuvant therapy. However, its therapeutic value is questionable, and it may be associated with considerable morbidity [11]. The sentinel lymph node biopsy has been suggested as a potentially useful technique to stage periocular SCC, especially in patients with recurrent, large, or highly invasive lesions or those with perineural invasion (Chap. 11) [11, 13].
5.9.2.3 Radiation Therapy
Radiation therapy has been used in the treatment of eyelid malignancies since the beginning of the twentieth century. SCC is relatively radioresistant and responds even less than BCC to radiation [1]. However, postoperative radiotherapy has been recommended in all patients with microscopic perineural invasion [14], as the role of surgery in the treatment of perineural spread seems to be only palliative [15].
Three-dimensional conformal planning or intensity-modulated radiation therapy is needed to minimize damage to adjacent structures, and synchronous chemotherapy should be considered to potentiate the effectiveness of radiation. Recent study suggested that primary radiotherapy for SCC of the eyelid provides high control rates with good function and cosmesis and should be considered an alternative to surgery in selected patients [16].
5.9.2.4 Chemotherapy
Chemotherapy may be used for patients with systemic disease and for those who cannot tolerate surgical excision or who decline surgery [17]. It is usually used as an adjuvant to surgery and radiotherapy in aggressive infiltrating SCC.
5.9.2.5 Topical Therapy
Topical treatments such as with fluorouracil (5-FU) cream and imiquimod cream (IMQ) were found to be effective treatments for SCC of the eyelids in only very small series of patients. Topical 5 % 5-FU cream was found to be useful in the treatment of squamous cell carcinoma in situ involving the eyelid, including the eyelid margin [18]. Topical 5 % IQ treatment was reported as successful in cases with intraepidermal as well as invasive SCC of the eyelids [19].
5.9.2.6 Photodynamic Therapy
Photodynamic therapy (PDT) is emerging as a promising treatment for patients with multiple or large SCC or in whom surgery is not appropriate. In such cases PDT is associated with reasonable efficacy, good cosmesis, and limited morbidity. However, until prospective controlled trials are performed, the precise role of PDT in relation to more conventional surgical approaches remains to be defined [20, 21].
5.10 Prognosis
5.10.1 Prognostic Factors
High-risk eyelid SCC lesions are those larger than 2 cm, with poor histological differentiation, deep invasion, and the presence of perineural invasion [22]. Recurrent tumors and tumors developing in scars or in immunocompromised patients also imply a poor prognosis [23, 24]. The histologic variant of adenoid SCC is associated with a better prognosis [1].
5.10.2 Staging
According to the applied practical review of the American Joint Committee on Cancer (AJCC) 7th edition [25], primary SCC is classified into stages I, II, III, and IV stages according to size, adjacent invasion, complete resection that requires enucleation, exenteration or bone resection, involvement of regional lymph nodes, extensive invasion making the tumor not resectable, and evidence of distant metastasis. This classification was found to be a practical tool for staging of carcinoma of the eyelids [26].
Box 5.1: Salient Diagnostic Features of Squamous Cell Carcinoma
Painless nodular, plaque-like, or ulcerated lesions with scaling and fissuring of the skin and irregular, rolled, pearly borders
Microscopic findings of infiltrative neoplasm arising from the epidermis and composed of polygonal cells with abundant acidophilic cytoplasm and prominent, hyperchromatic, pleomorphic nuclei
The presence of dyskeratotic cells with the formation of keratin pearls and intercellular bridges
5.10.3 Local Spread
Eyelid SCC is potentially fatal and responsible for considerable morbidity [9]. Aggressive or neglected cases of eyelid SCC may spread into the lacrimal passages, the orbit, and the intracranial cavity. SCC is by far the most frequent of the secondary epithelial neoplasms in the orbit [1]. However, orbital invasion is a rare complication that has been reported to occur in 2.5 % of all eyelid BCC and SCC [27]. Orbital invasion of eyelid SCC may take years to occur, often preceded by several surgical interventions, irradiations, and recurrences of the tumor. If left unattended, the entire orbital region and a major portion of the face are destroyed in an ulcerating fungating crater [1]. Orbital spread is usually associated with complete ptosis, ophthalmoplegia, and proptosis. Eventually, involvement of the orbital nerves and bones causes severe and constant pain [1, 10].
5.10.4 Perineural Spread
Perineural spread of SCC occurs in up to 14 % of facial lesions [28]. The perineural infiltration of SCC of the eyelids along branches of the trigeminal nerve, the extraocular motor nerves, and the facial nerve facilitates its spread into the orbit, periorbital structures, and intracranial cavity [29]. Once clinical signs or symptoms of perineural spread have developed, the prognosis is poor, with around 50 % recurrence after simple excision [28].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


