Stridor, Aspiration, and Cough
Joseph E. Dohar
Samantha Anne
INTRODUCTION
Love and a Cough Cannot be Hid
No truer words than these by George Hebert. Few signs and symptoms are perceived as being as distressing to parents as cough, aspiration, and stridor. At a glance, one may consider “stridor,” “aspiration,” and “cough” as each constituting chapters unto themselves. What unifies these three entities is their anatomic and functional interrelatedness that often results in the concomitant concurrence of all three. Although this chapter discusses each independently, the clinical reality is that any disruption of the complex structure and function of the upper aerodigestive tract often adversely alters the delicate coordination between swallowing and respiration. Hence, it is not uncommon for any combination of these three signs and symptoms to coexist. Even in clinical presentations where only one of these signs dominates, the astute clinician will always search for the other two. This is especially true for aspiration that is not uncommonly “silent” in children. Not only is such an assessment diagnostically imperative but also therapeutically significant as management is vastly altered by the relative proportionate degree to which each of these is playing a role. It is no wonder then that pediatric aerodigestive centers of excellence have emerged in tertiary children’s hospitals as representative of the “gold standard” of such care. Such environments are predicated upon the dynamic overlap between stridor, aspiration, and cough. They integrate an interdisciplinary and systematic means by which to assess all three by combining traditional and fundamental tools with more recently developed diagnostic evaluations such as functional endoscopic evaluations of swallowing (i.e., FEES) and breathing.
STRIDOR
Stridor is an abnormal sound due to turbulent airflow through a partially obstructed airway. The level of obstruction can often be clinically localized to the supraglottis, the glottis, or the subglottis and trachea based on the characteristics of the stridor. Specifically, the type of stridor, whether inspiratory, expiratory, or biphasic, helps to localize the site of obstruction. Supraglottic obstruction generally presents with inspiratory stridor while intrathoracic obstruction presents with expiratory stridor. Fixed anatomic obstructive lesions tend to cause biphasic stridor. Finally, the quality of stridor may also provide clues to location and etiology. For example, high-pitched inspiratory stridor is nearly always seen in neonates with laryngomalacia.
Evaluation
The evaluation of a child with stridor begins with a thorough history and physical examination from which most often a differential diagnosis is derived. The most important step in evaluating a child with stridor is determining acuity of the respiratory distress. For an actively stridorous child with severe retractions and impending obstruction, urgent airway stabilization is necessary. Once stabilized, a full evaluation can follow.
History and Physical Exam
The perinatal history specifically determining whether or not endotracheal intubation or airway intervention was required is paramount. The onset, triggers, progression, and presence of exacerbating and/or alleviating factors must also be ascertained. Associated symptoms including presence of aspiration or difficulty with feedings, hoarseness, and signs of reflux must be identified. Positional
changes that worsen or lessen stridor should be noted as well as recurrent or persistent croup episodes. Noting cyanotic spells or apneas helps to quantify the severity of the obstruction. Lastly, comorbidities such as neurologic abnormalities and past surgeries such as those to correct congenital cardiac anomalies must be recorded.
changes that worsen or lessen stridor should be noted as well as recurrent or persistent croup episodes. Noting cyanotic spells or apneas helps to quantify the severity of the obstruction. Lastly, comorbidities such as neurologic abnormalities and past surgeries such as those to correct congenital cardiac anomalies must be recorded.
The physical examination begins with an overall impression of the child without invoking excitement. Vital signs must be reviewed for the presence of fever suggestive of an acute infectious etiology, tachypnea, oxygen desaturations, and tachycardia. Dysmorphic features may suggest a syndrome. Observe the child for audible stridor at rest, signs of increased respiratory work including subcostal, intercostal, and suprasternal retractions. Some clinicians may confuse stertor with stridor, and this distinction must be ascertained as early as possible since the subsequent evaluation differs for each. Voice and/or cry quality should be perceptually assessed. Dysphagia may be immediately evident as drooling. A thorough head and neck examination must follow with careful attention to palpation and visualization of any masses within oropharynx and neck. Auscultation of the upper airway and chest qualifies the type of stridor and identifies its phase of occurrence as inspiratory, expiratory, or biphasic.
Radiology
Useful imaging may include chest and neck radiographs. Chest radiographs, in anterior-posterior, lateral upright, and lateral decubitus projections can aid in the diagnosis of several causes of stridor. Inspiratory/expiratory films can reveal foreign bodies in the central airway as well as in the bronchi. Biphasic radiographs may also reveal hyperinflation from obstructing lesions or lower airway disease such as infiltrates or pneumonias. Lateral neck films can reveal key findings such as the “thumbprint” sign of inflamed epiglottis in epiglottitis or thickened retropharyngeal soft tissue in phlegmon- and/or abscess-related airway obstruction.
Computed tomography (CT) and magnetic resonance imaging (MRI) can be used for airway evaluation but do not replace a thorough endoscopic evaluation of airway stenosis or malacia. CT with contrast identifies extrinsic masses or vascular lesions that compress the airway. Both CT and MRI can be used to evaluate vascular malformations in general.
Endoscopy
Following a careful selection of radiologic imaging and after a thorough examination of the child, endoscopy is crucial to complete the evaluation of a child with stridor.
Flexible nasopharyngolaryngoscopy (NPL) is an invaluable tool in evaluation of a stridorous child when possible. The presence of obstructive lesions, dynamic collapse of supraglottic structures, and dysfunction of vocal cord mobility are ascertained. Caution must be used when considering awake flexible endoscopy in a child with impending airway obstruction as the potential agitation may precipitate an emergent situation. Starting with evaluation of the nasal cavities and nasopharynx, systematic evaluation of the oropharynx, hypopharynx, and the larynx must follow. The true vocal cord function must be ascertained, and the presence of collapse of supraglottic structures must be documented. Signs of gastroesophageal reflux disease (GERD) should be noted including posterior glottic edema and edema/erythema of the arytenoids. Double pH probe studies, esophageal biopsy, and radionuclide studies can then further corroborate reflux findings on endoscopy.
Rigid laryngotracheobronchoscopy is the standard for evaluating a child with stridor. In anticipation of performing the procedure, it is crucial for the anesthesia team to coordinate with the endoscopist the plan for airway management during the procedure. Intravenous steroids, such as dexamethasone 0.5 to 1 mg/kg should be given in anticipation of airway edema after instrumentation. Prior to inserting the bronchoscope, topical lidocaine should be sprayed on the larynx and into the trachea to decrease airway reactivity and to prevent laryngospasm intraoperatively and on awakening.
The operative table must be carefully prepared with an age-appropriate bronchoscope and two sizes smaller in situations of anticipated airway stenosis. Additionally, appropriate pharyngeal, laryngeal, and bronchial rigid suctions, different size endotracheal tubes, and laryngoscopes—either Parsons type or anesthesia blades such as Miller or Phillips blade—must also be available. Decide whether the procedure is to be done under spontaneous ventilation, paralysis, or jet ventilation. Spontaneous respiration is ideal in that vocal cord function and dynamic compression can be evaluated. Maintaining spontaneous ventilation is also safer in the event that the airway is considered tenuous and/or there is risk of losing an airway. If possible severe stenosis is suspected, one can avoid injury from a rigid bronchoscope by substituting suspension micro-direct laryngoscopy and bronchoscopy with a Hopkins rod telescope under jet ventilation. The airway can be sized by intubating with a cuffless endotracheal tube and documenting the size at which an air leak is appreciated at less than 20 cm water pressure.
Differential Diagnosis
The differential diagnosis for a child with stridor is extensive, as seen in Table 89.1. Because an exhaustive review of all possible etiologies is impractical given the limitations of this chapter, the following discussion focuses on the five most common etiologies: laryngomalacia, vascular anomalies, laryngotracheitis, vocal cord immobility, and subglottic stenosis. The reader is referred to other chapters in this textbook that discuss most of the other etiologies.
Laryngomalacia
Laryngomalacia is the most common etiology for stridor in infancy. Laryngomalacia is posited to be due to immature cartilages and/or immature neuromuscular tone of the
larynx leading to obstruction of the supraglottis. Several classification systems exist for laryngomalacia based on severity or location (1,2). Based on an anatomic designation, the sites of obstruction can be due to inward collapse of the aryepiglottic folds, long tubular epiglottis that curls on itself, anteromedial collapse of the corniculate and cuneiform cartilages, posterior inspiratory displacement of the epiglottis against the posterior pharyngeal wall or inferior collapse toward the vocal folds, and/or short aryepiglottic folds (3).
larynx leading to obstruction of the supraglottis. Several classification systems exist for laryngomalacia based on severity or location (1,2). Based on an anatomic designation, the sites of obstruction can be due to inward collapse of the aryepiglottic folds, long tubular epiglottis that curls on itself, anteromedial collapse of the corniculate and cuneiform cartilages, posterior inspiratory displacement of the epiglottis against the posterior pharyngeal wall or inferior collapse toward the vocal folds, and/or short aryepiglottic folds (3).
TABLE 89.1 DIFFERENTIAL DIAGNOSIS: STRIDOR IN A CHILD | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||
Diagnosis of the condition is based primarily on history and physical examination findings. Patients usually present with onset of stridor that tends to worsen with crying, feeding, or in supine position within first few weeks of life. GERD has been shown to be frequently associated with laryngomalacia (4). Symptoms of GERD should be elicited including frequent spit-ups, recurrent emesis, and back arching after feeds. More severe laryngomalacia can cause weight loss and failure to thrive with or without cyanotic episodes, and this history must be attained.
On physical examination, high-pitched inspiratory stridor is the classic presentation. Suprasternal and/or substernal retractions suggest more severe obstruction. Flexible endoscopy in clinic on an awake child can confirm the diagnosis. Features of laryngomalacia including prolapse of the epiglottis, arytenoids, and supraglottic edema must be noted. Signs of reflux must also be documented (Figs. 89.1 and 89.2).
Fortunately, the natural history of laryngomalacia is spontaneous resolution over the first 1 to 2 years of life. Medical management with aggressive acid suppression therapy is often all that is necessary to control the symptoms and signs. However, increased severity of obstruction with failure to thrive, cor pulmonale, and/or cyanotic episodes prompts surgical intervention. Supraglottoplasty, done with either CO2 laser or “cold” with microlaryngeal instruments, should address specific areas of collapse or in releasing areas of constriction such as tight aryepiglottic folds. Rarely is tracheotomy necessary.
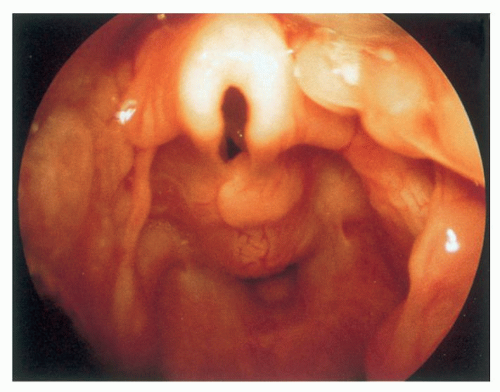 Figure 89.1 Endoscopic view of laryngomalacia during expiration. |
Vascular Anomalies
Vascular anomalies that cause stridor in a child include aberrant right subclavian artery, high-riding innominate artery, pulmonary artery sling, and vascular rings and slings. An aberrant right subclavian artery is the most common congenital vascular anomaly. Although the majority of infants with this congenital vascular anomaly present with dysphagia lusoria due to the retroesophageal course of the artery, some may present with stridor. This diagnosis is often made with a barium esophagram that reveals a filling defect in the esophagus. It is confirmed with findings
on CT angiography (CTA), MRI, or magnetic resonance angiography (MRA). Surgical correction via a right thoracotomy approach is recommended for symptomatic patients and has been to shown to be highly successful (5).
on CT angiography (CTA), MRI, or magnetic resonance angiography (MRA). Surgical correction via a right thoracotomy approach is recommended for symptomatic patients and has been to shown to be highly successful (5).
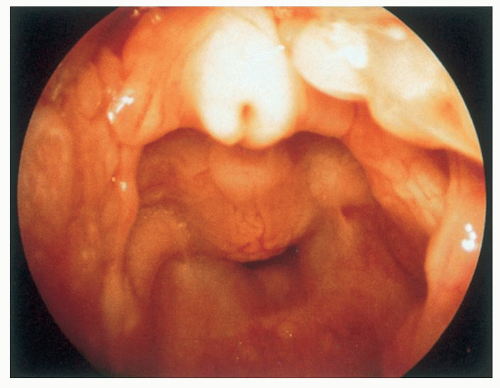 Figure 89.2 Endoscopic view of laryngomalacia during inspiration with folding inward of the epiglottis, shortened aryepiglottic folds, and collapse of the cuneiform cartilages completely obstructing the laryngeal introitus. |
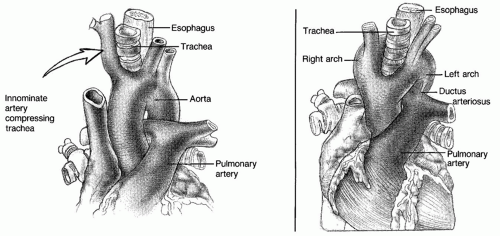 Figure 89.3 Vascular anomalies causing tracheal compression. |
An aberrant course of the innominate artery commonly causes compression of anterior tracheal wall but rarely is symptomatic enough to warrant surgical intervention. In symptomatic children, expiratory, biphasic stridor, “recurrent croup,” and/or recurrent pneumonia occur. Bronchoscopy demonstrates pulsatile compression of the anterior tracheal wall. Applying pressure on the anterior tracheal wall with the distal tip of the rigid bronchoscope may diminish the brachial pulse. Diagnosis can be confirmed with CTA, MRI, or MRA. Treatment is expectant in most cases. With severe symptoms, arteriopexy to the sternum is effective (6) (Fig. 89.3).
Lastly, a pulmonary artery sling or vascular ring can also present with stridor. The two most common types of complete vascular rings, double aortic arch and right aortic arch with left ligamentum arteriosum, make up nearly 85% to 95% of all vascular rings (7). Double aortic arches occur due to persistence of embryonic bilateral fourth branchial arch vessels and dorsal aortas. Pulmonary artery slings occur when the left main pulmonary artery arises as a branch of the right pulmonary artery, instead of from the main pulmonary artery due to an abnormality of the sixth branchial arch artery development. Pulmonary artery slings are often associated with complete tracheal rings (Fig. 89.4).
In general, both of these anomalies present with signs of tracheal compression such as biphasic stridor. In addition, chronic cough, recurrent pneumonias, and recurrent croup can occur. Symptoms of dysphagia with a double aortic arch tend to be a more frequent presentation of older children with milder tracheal compression who present later in life. Always suspect vascular anomalies in an infant with atypical “asthma” or in children with severe symptoms associated with respiratory tract infections out of proportion to what is expected; especially when a history of noisy breathing since birth is elicited.
Chest radiographs can reveal compression of the trachea, an abnormally positioned aortic arch, and/or hyperinflation of the right lung with anomalous left pulmonary artery. Since a right-sided aortic arch is almost always present in a vascular ring, identifying this on a chest radiograph is critical. A right-sided aortic arch courses over the right main stem bronchus instead of the usual left main stem bronchus as in a left-sided aortic arch. Thus, the arch
itself may not necessarily occupy the right hemithorax. The normal left-sided aortic arch displaces the carina to the right as it courses over the left main stem bronchus. This slight deviation in the normal tracheal air shadow can often be appreciated on the anteroposterior (AP) or posteroanterior view of the chest radiograph. In a right-sided aortic arch, the carina deviates to the left instead as the aorta courses over the right main stem bronchus.
itself may not necessarily occupy the right hemithorax. The normal left-sided aortic arch displaces the carina to the right as it courses over the left main stem bronchus. This slight deviation in the normal tracheal air shadow can often be appreciated on the anteroposterior (AP) or posteroanterior view of the chest radiograph. In a right-sided aortic arch, the carina deviates to the left instead as the aorta courses over the right main stem bronchus.
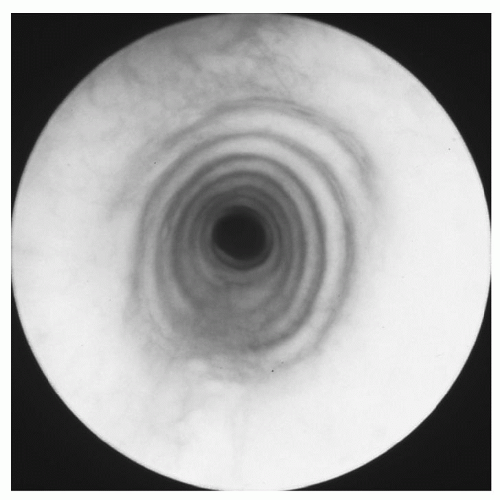 Figure 89.4 Endoscopic view of complete tracheal rings. |
A barium esophagram performed in patients with dysphagia may reveal a filling defect resulting from posterior vascular compression. Echocardiograms readily reveal anomalous vascular structures. CT/CTA or MRI/MRA generally confirms the diagnosis in cases of vascular rings or pulmonary artery sling. Lastly, bronchoscopy may be used to diagnose pulsatile vascular compression and cases of complete tracheal rings associated with a pulmonary artery sling.
While milder vascular anomalies may be observed closely, vascular rings and pulmonary artery slings generally require surgical repair. Prolonged intubation, reflex apnea, and failure of medical treatment are absolute indications for surgical repair. In addition, severe dysphagia and failure to thrive, recurrent bronchopulmonary infections, associated asthma/cystic fibrosis, or exercise intolerance are relative indications for surgical repair. Fortunately, patients without other significant comorbidities or associated anomalies have favorable surgical prognosis, and symptoms tend to resolve after repair.
Laryngotracheobronchitis
Viral laryngotracheobronchitis, or croup, is the most common infectious source of stridor in children. Although the most common cause is parainfluenza virus type 1, other viruses such as respiratory syncytial virus, influenza A, and parainfluenza types 2/3 can also cause viral croup. Most common age of occurrence is from age 6 months to 3 years, although it is rare in infants less than a year of age. When it occurs in a child less than 1 year of age, a possible underlying airway abnormality or stenosis should be suspected.
The diagnosis is largely based on history and physical examination findings. The usual course of illness begins with 2- to 3-day prodrome of upper respiratory illnesstype symptoms progressing to barking cough and inspiratory stridor. If there is presence of high fever, rapid progression of symptoms, drooling, and odynophagia, epiglottitis should be considered, and rapid evaluation and treatment should be initiated. On examination, the child will exhibit a fairly prototypical barky cough, stridor, and varying degrees of increased work of breathing.
A high-kilo voltage soft tissue neck radiograph, AP view, may demonstrate the classic “steeple” sign, depicting the narrowing of the subglottis. Lateral soft tissue radiography may demonstrate an edematous epiglottis (thumbprint sign) seen in epiglottitis, which can sometimes present with early similar clinical symptoms as croup. Flexible NPL can be safely performed in a clinically stable child and sometimes reveals an edematous subglottis visualized through abducted vocal cords.
Laryngotracheobronchitis, is usually self-limited and is most often managed conservatively as an outpatient. However, with increased work of breathing, hospital admission and close observation may be necessary. Humidification, blow-by oxygen supplementation, and continuous pulse oximetry can be used in management. Corticosteroids, such as dexamethasone at dose of 0.5 to 1 mg/kg, are prescribed to decrease subglottic edema. Lastly, nebulized racemic epinephrine rapidly reduces subglottic inflammation while steroids are taking effect; however, the effects are transient and children often develop rebound edema. Rarely do the children develop worsening stridor and respiratory distress requiring intubation. Heliox, a mixture of helium and oxygen, may supplant endotracheal intubation by reducing the work of breathing. If necessary, nasotracheal intubation with an endotracheal tube one size smaller than expected for the child’s age must be used. Failure to extubate despite observation and medical management should prompt direct laryngoscopy with bronchoscopy to evaluate for underlying subglottis stenosis or other airway anomalies.
Vocal Cord Immobility
Vocal cord immobility is the third most common congenital cause of stridor, occurring in nearly 10% of the cases. Causes of vocal cord immobility include neurologic causes such as Arnold-Chiari malformation or hydrocephalus, trauma from stretch injury to recurrent laryngeal nerve during birthing process, or trauma from injury to nerve during cardiac surgery.
Children with unilateral vocal cord immobility usually present with a weak voice and signs of aspiration. With bilateral vocal cord immobility, inspiratory stridor and an abnormal cry are also prominent. The diagnosis may be made with flexible NPL in an awake child although this assessment is often more challenging than is recognized. Vocal fold immobility is sometimes difficult to distinguish from movement resulting from a Bernoulli effect. Similarly, paresis may be over diagnosed in a sedated child. Children with significant laryngomalacia or supraglottic hyperfunction may simply obscure adequate visualization of their vocal cords. Finally, “pseudoparalysis” or cricoarytenoid joint ankylosis may be misdiagnosed as vocal fold immobility.
Such diagnostic challenges not withstanding, once diagnosed, further evaluation depends on suspected etiology. Imaging of the head down to the chest along the entire course of the recurrent laryngeal nerve might be necessary to identify neurologic or cardiovascular anomalies. Although more logistically challenging in children, laryngeal EMG may assist with the diagnosis in difficult cases and often provides information needed to make clinical management decisions. As more experience is gained with laryngeal EMG in children, it is likely that the role of this intervention will expand not only in cases with diagnostic uncertainty but as a means of providing objective data to assist in management decisions.
If an obvious cause of immobility is identified, treatment of that cause often leads to return of normal vocal fold movement such as decompression of a Chiari malformation. In idiopathic cases, observation is recommended since most cases resolve within first 2 years of life. Delayed resolution after several years has been reported in children and the precise timing beyond which spontaneous recovery of vocal fold movement in children cannot occur is unknown. If there is significant difficulty in maintaining an adequate airway in cases of bilateral vocal cord immobility, tracheostomy may be temporally needed. If the immobility is permanent, various surgical procedures are available to improve airway patency. In cases of bilateral immobility, vocal cord lateralization, excisional procedures such as laser arytenoidectomy, posterior cordotomy, and reinnervation procedures are all potential options pending the specific circumstances of the child.
Subglottic Stenosis
Subglottic stenosis is a congenital or acquired narrowing of the subglottis. The subglottis is the area extending from the lower surface of the true vocal cords to the inferior margin of the cricoid cartilage. The narrowest part of an infant’s airway is the subglottis and it normally measures 4 to 7 mm. Less than 4 mm in size in a newborn or 3.5 mm in a premature infant is diagnostic of subglottic stenosis (Fig. 89.5).
Acquired subglottic stenosis is the most common type and requires treatment more often largely because of improved perinatal intensive care and survival of premature infants who required prolonged endotracheal intubation for premature lung disease. Nearly 90% of acquired cases are due to prolonged endotracheal intubation. Risk factors for development of subglottis stenosis include prolonged duration of intubation, overly large endotracheal tube, recurrent intubations, and presence of infection during course of intubation. Other causes of acquired subglottic stenosis include blunt, penetrating, or caustic laryngeal trauma. Iatrogenic damage to subglottis from previous cricothyroidotomy, high tracheostomy, or laser surgery can also be causative.
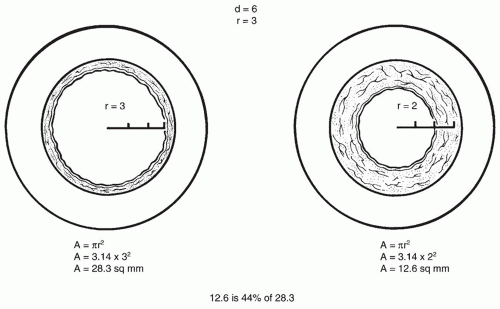 Figure 89.5 The normal newborn subglottic larynx has a diameter of 5 to 7 mm and a crosssectional area of approximately 28.3 mm2. Only 1 mm of edema reduces the area to 12.6 mm2, 44% of normal. (From Holinger LD. Evaluation of stridor and wheezing. In: Holinger LD, Lusk RP, Green CG, eds. Pediatric laryngology and bronchoesophagology. Philadelphia, PA: Lippincott-Raven, 1997:41-48, with permission.) |
On the other hand, congenital subglottic stenosis is diagnosed when all other causes have been excluded. It is thought to occur due to failure of the laryngeal lumen to completely recanalize during embryogenesis. Congenital subglottic stenosis can be divided into a membranous type when there is mainly soft tissue occluding the lumen or a cartilaginous type when it is due to abnormalities of cricoid (elliptical cricoid), which narrow the lumen.
Presenting symptoms depend on the severity of the stenosis. If severe, audible biphasic stridor possibly with signs of respiratory distress and increased work of breathing are seen. In milder cases, the child may contract recurrent episodes of croup with or without feeding issues. A thorough birth history must be documented and includes prematurity, need for intubation, and any associated comorbidities. Any feeding difficulties and failure to thrive should be noted. Signs of reflux should be sought.
On physical examination, observation of the patient’s overall body habitus and breathing patterns provides useful
diagnostic clues. Auscultation of chest and neck may reveal biphasic stridor and the voice may be hoarse or weak. Flexible NPL may allow for adequate visualization of the subglottis through abducted vocal cords. Diagnosis using a flexible fiberoptic laryngoscope in a nonsedated child may be challenging as a prominent anterior cricoid cartilage lamina may be confused with subglottic stenosis. In such cases, advancing the flexible endoscope through the vocal cords is not recommended due to the risk of inducing laryngospasm and life-threatening airway obstruction.
diagnostic clues. Auscultation of chest and neck may reveal biphasic stridor and the voice may be hoarse or weak. Flexible NPL may allow for adequate visualization of the subglottis through abducted vocal cords. Diagnosis using a flexible fiberoptic laryngoscope in a nonsedated child may be challenging as a prominent anterior cricoid cartilage lamina may be confused with subglottic stenosis. In such cases, advancing the flexible endoscope through the vocal cords is not recommended due to the risk of inducing laryngospasm and life-threatening airway obstruction.
CT and MRI, although rarely necessary, may help to quantify the length of the stenosis and, hence, aid in surgical planning. The gold standard for evaluation of the subglottis is direct laryngoscopy and bronchoscopy, which also have the advantage of identifying secondary airway lesions. Sizing of the airway with endotracheal tubes according to the Myer-Cotton staging system is recommended. This staging system describes the percent narrowing of the subglottis as determined by various sized endotracheal tubes with one of four grades. Grade I is less than 50% obstruction, grade II is between 51% and 70% obstruction, grade III is 71% and 99% obstruction, and grade IV is no detectable lumen (8).
Management of stenosis is dependent on severity of stenosis and symptomatology of the child. In general milder stenosis, Cotton-Myer grade I/II can be managed medically and with close observation. GERD therapy is prescribed as it has been shown to reduce edema and decrease the number of croup episodes. More severe stenosis, grades III/IV usually necessitates surgical intervention. Surgical options depend on the type, length, and degree of stenosis in addition to patient characteristics such as overall general medical condition, swallowing ability, presence of aspiration, age, and weight of the child. Options include tracheostomy, endoscopic dilation, and open procedures. Open procedures can include expansion procedures such as anterior or posterior cricoid split or both with cartilage grafting or cricotracheal resection.
Management
Management of stridor in general depends on the severity and acuity of the airway distress. While preparations are underway for airway management, the patient must be evaluated expeditiously and vital signs must be assessed. Initial measures include determining the patient’s oxygen saturation and initiating humidified supplemental oxygen keeping in mind the potential for CO2 retention as a possibility even if the patient exhibits normal oxygen saturation. Appropriate medical therapy must be initiated including steroids, intravenous antibiotics, and nebulized racemic epinephrine depending on the working diagnosis. Once clinically stable, the patient should be transferred to an appropriate monitored unit.
When there is impending obstruction, preparations must be made for intubation. If possible, intubation should proceed in a controlled environment with an anesthesia team present in the operating room and with the operative plan clearly discussed with all members of the team. The size of an endotracheal tube for intubation should be age appropriate and is determined by the formula: (age + 4)/4 except situations of airway stenosis where the smallest size adequate for oxygenation and ventilation should be used. Rarely is emergency tracheostomy necessary. Cricothyroidotomy is not recommended in pediatric patients due to the small size of the cricothyroid membrane and the increased incidence of laryngeal injury.
ASPIRATION
Aspiration is the penetration of oral and nasal secretions, food particles, or refluxate through the vocal cords. A small amount of aspiration occurs normally and is not considered pathologic provided effective clearance mechanisms are intact. However, when the amount aspirated overwhelms clearance and defense mechanisms, bronchopulmonary complications result.
A normal swallowing mechanism includes three phases— oral, pharyngeal, and esophageal. The oral phase includes the oral preparatory phase and the oral transport phase. The oral preparatory phase involves formation of a bolus and the transport phase involves propulsion of the bolus from the mouth into the oropharynx. The pharyngeal phase is a complicated process of movement of the bolus from the oropharynx into the esophagus that includes soft palate elevation to close the nasopharynx, laryngeal elevation, glottic closure, contraction of the pharyngeal constrictors, and relaxation of the cricopharyngeus to allow passage of bolus. Lastly, the esophageal phase is the transport of the bolus from the esophagus into the stomach. Normal swallow function is essential to prevent aspiration. In addition, protection is also provided by glottic closure that depends on normal function of the epiglottis, vocal cords, and aryepiglottic folds.
Diagnosis
Diagnosis of a child with aspiration begins with an accurate history. Aspiration often presents with cough and choking with feeding. With silent aspiration, a protective cough reflex is absent. Depending on the etiology of aspiration, the child may also present with hoarseness, stridor, or dysphagia. There may be a history of recurrent pneumonia or chronic respiratory illness. The medical history should include recent surgeries, traumas, comorbidities, and a complete birth history. Risk factors for aspiration include prematurity, central nervous system anomalies, and anatomic abnormalities of the aerodigestive tract.
A thorough head and neck examination is performed with attention to cranial nerve function. Examination of the oral cavity should focus on both form and function of the tongue and palate. Note any masses or lesions that are present. Facial dysmorphisms and any neurologic deficits must be identified.
Endoscopy
Once a thorough history and physical examination is completed, an endoscopic evaluation can diagnose aspiration and, in addition, may reveal the etiology in many cases. Simple flexible NPL can evaluate vocal cord mobility and identify obvious structural abnormalities such as a laryngeal cleft. The nasopharyngolaryngoscope, in addition, can be used to perform a functional endoscopic evaluation of swallowing, or FEES, to directly evaluate swallow mechanism. The scope is positioned at the level of the soft palate and used to visualize the hypopharynx and the larynx while the patient is fed various consistencies of colored food. Several parameters are recorded including laryngeal penetration, aspiration, pharyngeal pooling, and premature spilling. While this technique is advantageous in that it avoids radiation and is relatively inexpensive, the success of the procedure depends largely on the skill of the physician and speech language pathologist and most importantly depends on the patient’s cooperation. FEES is also considered more sensitive in detecting microaspiration. The most distinct limitation of FEES is the “white out” that precludes visualization of the swallow itself. The interpretation of the study relies on what is visualized immediately before and after the swallow. FEES is not physiologic, which is another limitation of the technique. When sensory testing to assess the laryngeal adductor reflex (LAR) is included, the study is referred to by the acronym FEEST.
Operative endoscopy is often necessary for further diagnosis. Direct laryngoscopy, bronchoscopy, and esophagoscopy can be performed to evaluate for structural abnormalities of the aerodigestive tract such as laryngeal clefts, tracheoesophageal fistulas (TEFs), or strictures. Bronchial alveolar lavage can be performed to assess for lipid-laden macrophages suggestive of aspiration and esophageal biopsy can reveal signs of reflux esophagitis.



