photographs. Pseudoesotropia can be differentiated from a true manifest deviation by use of the corneal light reflex and the cover-uncover test, when possible. Once pseudoesotropia has been confirmed, parents can be reassured that the child will “outgrow” the appearance of esotropia. As the child grows, the bridge of the nose becomes more prominent and displaces the epicanthal folds, so that the sclera medially becomes proportional to the amount visible on the lateral aspect. It should be stressed that it is the appearance of crossing that the child will outgrow. Some parents of children with pseudoesotropia may incorrectly believe that there is an actual esotropia that will resolve on its own. Because true esotropia can develop later in children with pseudoesotropia, parents and pediatricians should be instructed that reassessment is needed if the apparent deviation does not improve.
 FIGURE 8.1. Pseudoesotropia caused by a wide nasal bridge and epicanthal folds. Note that the light reflex is centered in each pupil. (Reprinted with permission from Olitsky SE, Nelson LB. Pediatric clinical ophthalmology—A color handbook. London, UK: Manson Publishing, 2012, ISBN 9781840761511.) |
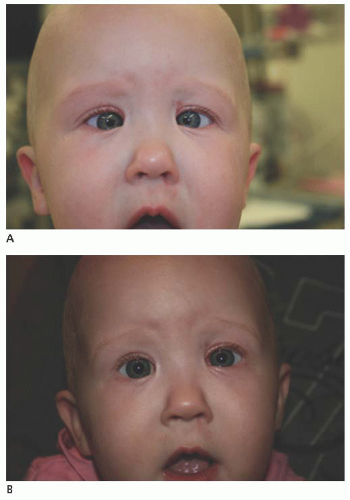 FIGURE 8.2. A: Congenital esotropia. B: Three days following surgery for congenital esotropia. (Reprinted with permission from Olitsky SE, Nelson LB. Pediatric clinical ophthalmology—A color handbook. London, UK: Manson Publishing, 2012, ISBN 9781840761511.) |
in adduction in patients with congenital esotropia. The differentiating features of these two conditions are listed in Table 8.1. IOOA results in elevation of the involved eye as it moves nasally (Fig. 8.4). DVD may also result in elevation as the eye moves nasally because the nose acts as a cover, dissociating the eyes. However, the vertical misalignment in DVD usually occurs equally in abduction, adduction, and primary position. When the adducting
eye in IOOA fixates, there is a corresponding hypotropia in the contralateral abducting eye. In DVD, contralateral hypotropia does not occur. IOOA and DVD frequently occur together in these patients. IOOA can be classified as Grades I to IV. Grade I represents 1 mm of higher elevation of the adducting eye in gaze up and to the side. Grade IV indicates 4 mm of higher elevation. These differences in elevation between the two eyes are measured from the 6 o’clock position on each limbus. A measurement of the degree of adduction that is required to elicit the overaction is also helpful when considering treatment. A moderatesize overaction that occurs with limited adduction may be more noticeable than a larger overaction that is seen only in extreme side gaze.
 FIGURE 8.3. Bilateral dissociated vertical deviation (DVD). A: Right DVD when left eye is fixating. B: Left DVD when right eye is fixating. (Reprinted with permission from Tasman W, Jaeger E. The Wills Eye Hospital atlas of clinical ophthalmology, 2nd Ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2001.) |
Table 8.1 DISTINGUISHING FEATURES OF DISSOCIATED VERTICAL DEVIATION AND INFERIOR OBLIQUE OVERACTION | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
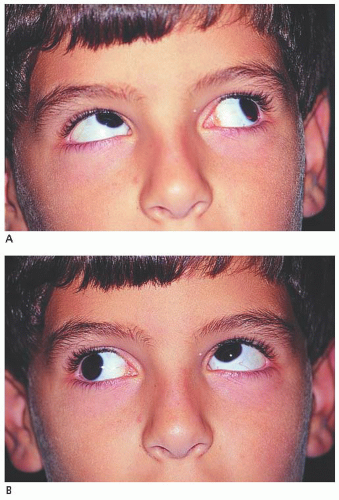 FIGURE 8.4. A-B: Overacting inferior oblique muscles. (Reprinted with permission from Tasman W, Jaeger E. The Wills Eye Hospital atlas of clinical ophthalmology, 2nd Ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2001.) |
Table 8.2 DIFFERENTIAL DIAGNOSIS OF CONGENITAL ESOTROPIA | ||||||||
|---|---|---|---|---|---|---|---|---|
|
small-angle exotropia. Because the role of binocular potential at birth could not be eliminated in predicting who would fall into each of these three categories, it is not known if active intervention, that is, further surgery, for small-angle deviations has any role in improving the long-term success rate of maintaining ocular alignment.
Table 8.3 CHARACTERISTICS OF THE MONOFIXATION SYNDROME | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||
lateral rectus muscles and a recess-resect procedure in the fellow eye are performed.
esodeviation, whereas after removal of the glasses the esodeviation is now quite large. Parents often blame the increased esodeviation on the glasses and note that their child has become dependent on them. This situation can best be explained on the basis of the child using the appropriate amount of accommodative effort after the glasses have been worn. When the child removes her glasses, she will continue to use an accommodative effort to bring objects into proper focus and increase the esodeviation. The strong desire these children have to wear their new glasses may be secondary to the relief of asthenopia, benefits of single binocular vision, or both. Explaining these phenomena to parents ahead of time is more effective than the same explanation after the fact.
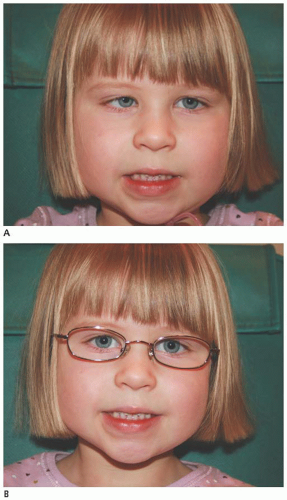 FIGURE 8.5. A: Accommodative esotropia. B: Glasses eliminate the need to accommodate and therefore the esotropia. (Reprinted with permission from Olitsky SE, Nelson LB. Pediatric clinical ophthalmology—A color handbook. London, UK: Manson Publishing, 2012, ISBN 9781840761511.) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


