Pediatric Eye Examination
Gregory Ostrow
Laura Kirkeby
INTRODUCTION
The pediatric eye exam is often feared by general ophthalmologists as a difficult, loud, frustrating, and often nonproductive office visit. Unlike adult patients, children often are not able to realize or communicate what is wrong with their eyes. Moreover, they often are not willing participants in the examination and so it requires significant effort to gain all the necessary information. To obtain a good history, we have to ask the right questions to both the parent and child, as well as direct our line of questioning so that the least amount of time is wasted while we have the child’s interest. Children must be engaged throughout the visit and the physician must hold their attention and learn how to “play” with them during the exam. Pediatric ophthalmologists are not born with the ability to make an exam fun and interesting for a child. This “art” of medicine requires significant patience, adaptability, and a lot of practice. This chapter will discuss various techniques that can be used to maximize the quality of pediatric eye exams as well as some suggestions to make the exam less tedious and more enjoyable for both the ophthalmologist and the pediatric patient.
Some general considerations to keep in mind throughout the exam:
1. Gather as much information from the chart as possible prior to entering the room. You have limited time when the child is paying attention and every moment counts. If you spend time looking at the chart while you are already in the room you may have lost the chance to complete your exam with the child’s cooperation.
2. Even when a child is not cooperative, a considerable portion of the exam can be completed to rule out worrisome pathology.
3. The child is the patient, not the parent. Remember to engage and make eye contact as much as possible with the child. Keeping up to date on current movies or characters or trends that different age children enjoy can allow you to break the ice with some brief conversation prior to the exam. A little small talk and a big smile will go a long way toward a cooperative visit.
4. Begin your examination when you walk into the room and while taking your directed history. Gross abnormalities, torticollis, red eyes, chalazia, strabismus, tearing, or irregular pupils can often be recognized at the onset of the exam while talking to the child and can help you direct your history and exam toward final diagnosis.
5. Speak to children in a language they can understand. Adult words or medical jargon will quickly alienate you from a child (and possibly a parent). Ask the child “Why are you here?” and “Why are we looking at your eyes?” Let children know you will not be doing anything without explaining it to them first. Make them your ally and helper for the exam. Children will respond much better if you ask: “Do you want to play some fun games and shine some cool lights in your eyes?” rather than just examining them without warning. Describe each instrument you use in child-friendly terms: “Can I take a peek at your pretty eyes in my microscope? Do you want to hold on to the handlebars while I look?” helps to make a slit lamp exam less threatening. For the indirect exam, let a child know you are going to put on your funny hat and show some beautiful rainbows. Ask which eye they want you to look at first.
6. Whenever possible, have well-trained staff put your dilating drops in. Try to not be in the room when it occurs. When you return for the dilated exam you can re-earn their trust by letting the child know that you won’t be letting anyone else put drops in their eyes today.
HISTORY
For most busy practitioners, a majority of the history is taken by ancillary staff. This can be very helpful for a baseline history but it is usually necessary for the physician to ask further directed questions to aid in diagnosis and treatment. Many practices use intake forms for patients where the parents can fill out some of the history in the waiting room prior to their evaluation. These can be very helpful, but it is imperative that they be pediatric oriented and not a standard adult medical history form that is given to all patients. One recommendation is to have check boxes in the chief complaint section for common pediatric eye complaints and a box for “other” if the patient or parent has something else to add. Some common chief complaints include failed vision
screen at school or pediatrician’s office, red eyes, itchy eyes, tearing eyes, wandering or lazy eyes, head tilt, shaking or jiggling eyes, bumps on the eyelids, headaches, or trouble with reading. Having one of these complaints checked on an intake sheet can help ancillary staff direct their line of questions and improve workflow significantly. A diagnosis and exam sheet from the referring physician is valuable as well.
screen at school or pediatrician’s office, red eyes, itchy eyes, tearing eyes, wandering or lazy eyes, head tilt, shaking or jiggling eyes, bumps on the eyelids, headaches, or trouble with reading. Having one of these complaints checked on an intake sheet can help ancillary staff direct their line of questions and improve workflow significantly. A diagnosis and exam sheet from the referring physician is valuable as well.
The chief complaint should be stated in the child’s or parent’s own words. This should be elaborated on in the history of present illness. For children with a complaint of tearing, the staff can ask the time of onset, whether it is part-time or full-time tearing, whether the eyes get red, whether there is a green or goopy discharge, or whether it gets worse outdoors or when the child is sick. For strabismus, questions to confirm the time of onset, part-time or full-time symptoms, whether the child closes or covers one eye, whether one eye or both eyes are seen wandering, or whether there is any associated head posturing, are all good questions your staff can ask for you so as not to waste valuable time in the room. If you must take the history yourself, only take what is necessary prior to beginning your exam. You can always ask the parent more questions after you have lost the child’s attention.
Past history questions should be directed toward possible contributing factors to the child’s diagnosis. This can include prenatal and postnatal history, birth weight, gestational age, history of major trauma, surgery or disease, developmental milestones, and any medical problems. Questions on grade level and school performance are also good questions. These can be included on your intake form along with medications and medication allergies. It is also important to know if the child was prescribed any glasses or patching therapy in the past.
Family history is very important for many pediatric eye diseases. Questions of family history should be directed toward any genetic diseases as well as a family history of pediatric eye diseases like pediatric glaucoma, cataracts, strabismus, or amblyopia (rather than adult onset eye problems like senile cataracts and macular degeneration).
PHYSICAL EXAM
The physical exam begins when you enter the room. Is the child alert? Does he or she hold you or her surroundings in regard? Are there any gross abnormalities to the face or orbit? Is the child adopting any head posturing? Are there any gross ocular alignment abnormalities or ptosis? The information you gain from just looking at the child at the beginning of the exam can help direct the remainder of your examination.
VISUAL ACUITY
Corrected or correctable visual acuity assessment is one of the most important parts of the pediatric eye exam. In a young baby, this may only be measuring visual attention and eye-popping reflex, but as a child matures you can measure vision in much more detail. Pediatric visual acuity should be measured at the most advanced developmental level for each child. This begins with an eye-popping reflex in very young children, proceeds through fix and follow, Central, Steady and Maintained (CSM), HOTV or pictures, and through to Snellen vision. The ophthalmologist who sees pediatric patients should be adept at measuring visual acuity in children of all ages.
Visual acuity assessment in preverbal children is truly an art but it is an art that can be learned with attention and repetition. There can also be some variability in the measurements of young children based on a child’s health and sleep patterns. A baby ready for a nap will be much less visually attentive than a child who is well rested. Pay close attention to how the child views his or her surroundings. Does the child follow faces or bright lights? Is there a good eye-popping reflex (opening his or her eyes widely when the room light is turned off)? Will he or she follow a fixation target with both eyes open? With one eye occluded? These findings can be codified in a young child as either fixes and follows (monocular or binocular) or does not fix and follow. The smallest possible fixation target that a child will regard should be used. Smooth pursuits do not usually develop until 6 to 8 weeks of age and should not be expected prior to that. A child who can fix and follow with one eye occluded can usually have their visual acuity further defined with the CSM measurement.
CSM measurements are a behavioral technique that use central fixation (holding an object of regard aligned with the visual axis), steady fixation (nystagmus or no nystagmus), and maintained fixation (in a strabismic patient this can be measured by a child’s ability to hold regard of an object with either eye when both eyes are open). For testing fixation, a distance target is more sensitive than a near target. An eye that will not fixate centrally (eccentric fixation) is assumed to have poor vision, likely worse than 20/200. An eye that is not steady (has nystagmus) usually has reduced vision. Nystagmus can be a good sign in a child where there are concerns of severely decreased vision as an eye with nystagmus is assumed to have at least pattern vision (the ability to see shapes). An eye that will not maintain fixation when the cover is removed is assumed to be amblyopic.
In a non-strabismic patient, the 10 base down prism testing method (or induced tropia test) can be applied to test for asymmetry. This method involves placing a 10 base down prism in front of either eye while the child has both eyes open and is fixating on a target. The prism generally degrades the image slightly and so a child with equal vision would be expected to maintain fixation with the eye that is not covered by the prism. If the child switches fixation with a vertical shift, it is assumed that the eye with prism is stronger (and therefore preferred). In practice, the symmetry of this test is probably more important than whether or not the fixation is shifted. Many children will shift vertically with the prism over either eye, which signifies symmetric vision in the same way as not shifting with both eyes. In a strabismic patient, the inability to hold fixation (not maintained) often signifies amblyopia. Some large-angle infantile esotropic children will fixate with
either eye depending on which side of the face the object is held. This phenomenon is called cross fixation and a child who cross fixates presumably has equal vision in each eye.
either eye depending on which side of the face the object is held. This phenomenon is called cross fixation and a child who cross fixates presumably has equal vision in each eye.
Many young (and older) children will resist occlusion of a good eye when one eye is amblyopic. Resisting occlusion of an eye should be documented in the chart. Whenever possible, visual acuity should be tested with one eye patched rather than with an occluder. Children will try to peek around an occluder not because they are cheaters but rather they prefer to use their dominant eye. The patch should be well fixed so that the child cannot tilt his or her head to see around it during testing.
Other Testing
In preverbal children, the optokinetic nystagmus (OKN) response can be used to demonstrate visual function. An OKN response can be elicited by rotating a drum with parallel vertical stripes in the child’s visual field. The eyes follow the stripes with an involuntary pursuit movement and are brought back to their initial starting point with a saccade. The eyes continue to demonstrate the OKN response while the drum rotates. An OKN response has an estimated visual acuity of counting fingers at 3 to 5 feet. The OKN drum can be very useful when assessing visual function in infants with nystagmus. In children with horizontal nystagmus, the drum must be held so that the lines are horizontal and the drum is rotated vertically in order to elicit vertical eye movements. If a vertical OKN response can be elicited in the presence of horizontal nystagmus, then vision is usually 20/400 or better.
Although quantifying visual function in preverbal children is usually very difficult, there are a few tests that can provide an estimate of their visual acuity in Snellen or logmar equivalents. Preferential looking techniques such as the Teller acuity and Cardiff cards use patterns and pictures to elicit a change in fixation, respectively. The Teller acuity cards are rectangular and have a high contrast pattern stimulus on one side and a plain stimulus on the other side. An examiner presents the card in front of the child without knowing the orientation of the pattern (to prevent bias) and monitors fixation through a small central peephole. If a child looks directly toward the pattern then it is presumed that the child can distinguish that level of spatial frequency. The examiner will then present the next card with gratings that have a higher spatial frequency until the child does not accurately fixate on the pattern. The highest spatial frequency that the child can locate is the grating acuity threshold and can be recorded as a Snellen equivalent. The test may be performed monocularly to detect amblyopia or binocularly to demonstrate the presence of visual ability in infants with neurologic or developmental disorders. Teller acuity cards are known to underestimate strabismic amblyopia.
The functional integrity of the entire visual pathway can be evaluated by measuring the visual evoked potentials (VEP). VEPs are generated by electroencephalographic activity in the visual cortex in response to a visual stimulus. A normal VEP requires that all components of the visual pathway including the macula, optic nerve, tracts, radiations, and the occipital cortex are functioning properly. The child wears three electrodes, which include an active electrode over the occipital area, a reference electrode on the forehead, and a ground electrode on the earlobe. The stimulus used in VEP testing is usually a pattern checkerboard or diffuse flash. In most cases, pattern-reversal VEP is the preferred stimulus and is elicited by a digital checkerboard with squares that reverse from black to white and back again. Although flash VEP can be less accurate, it can detect visual function in the presence of a media opacity, nystagmus, or when the patient has poor cooperation or is suspected to be malingering. The age-related visual acuity determined by the VEP response is approximately 20/400 in early infancy, which improves to approximately 20/20 by 6 months of age. VEP testing must be performed and analyzed by trained specialists, and uncooperative children may require sedation.
Visual acuity assessment in verbal children, while no less of an art form, is often less difficult for a general ophthalmologist. If a child is able to identify characters but not letters, Lea symbols or Allen cards can be used (Fig. 4.1). Parents can be given these pictures or symbols prior to the exam so that they
may teach them to the child at home. Many practitioners will use large (20/400) symbols with both eyes open to teach the children what the symbols are and to make the exam more of a game. Both Allen and Lea test only to a 20/30 level, which is adequate for younger children. HOTV is more sensitive than symbols for amblyopia in a preliterate child, and full lines are more sensitive than single letters due to the crowding phenomenon. If a child is shy or does not know the names of the HOTV letters, a card with HOTV in large print can be given to the child, and they can match with their finger what they see on the screen (Fig. 4.2). Parents can be helpful in full line screening as they can point to the letters in order and the child can point to the matching letter on their card in front of them. Tumbling E’s are used in a similar fashion to HOTV with a child pointing in the direction of the legs on the E.
may teach them to the child at home. Many practitioners will use large (20/400) symbols with both eyes open to teach the children what the symbols are and to make the exam more of a game. Both Allen and Lea test only to a 20/30 level, which is adequate for younger children. HOTV is more sensitive than symbols for amblyopia in a preliterate child, and full lines are more sensitive than single letters due to the crowding phenomenon. If a child is shy or does not know the names of the HOTV letters, a card with HOTV in large print can be given to the child, and they can match with their finger what they see on the screen (Fig. 4.2). Parents can be helpful in full line screening as they can point to the letters in order and the child can point to the matching letter on their card in front of them. Tumbling E’s are used in a similar fashion to HOTV with a child pointing in the direction of the legs on the E.
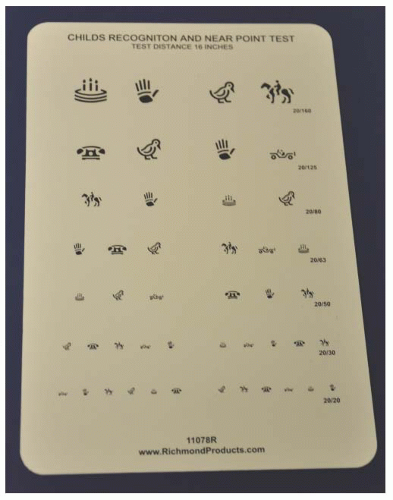 FIGURE 4.1. Allen card with picture of optotypes used for vision testing at near distance. |
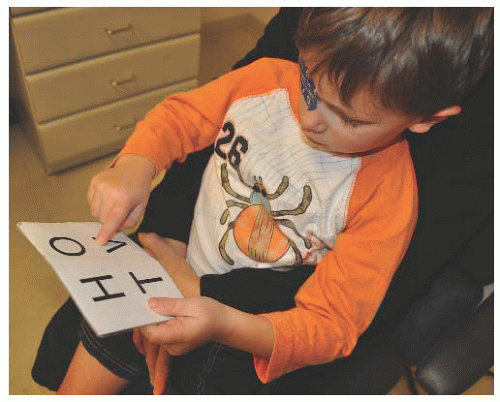 FIGURE 4.2. A child using an HOTV card to match the letters on a screen at distance. |
When a child is comfortable with his or her letters, vision should be tested with Snellen letters at a distance.
EXTERNAL EXAMINATION
Significant external pathology is often seen in the beginning of the exam when the child is being observed. Significant eyelid pathology, skin tags, growths, chalazia, or dysmorphology can usually be seen with ambient room lighting. In cases where there is some obvious pathology that needs a somewhat enlarged view, a handheld 20D or 28D lens can be used as a magnifier. This is especially helpful when examining the lids or orbits of a young child who may be difficult to examine with a slit lamp.
OCULAR ALIGNMENT AND MOTILITY
A thorough ocular alignment and motility examination is imperative for the pediatric ophthalmic examination. Any extraocular muscle imbalance in young children can disrupt the binocular visual system and interfere with visual development, which can cause permanent vision loss.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


