Strabismus
Alex V. Levin
Thomas W. Wilson
Stephen P. Kraft
David Smith
Linda Calpa
Strabismus can be classified into congenital or acquired forms, as well as comitant versus incomitant entities. Congenital strabismus is generally considered a misalignment that manifests within the first 6 months of life, while acquired forms have their onset after that time period. Comitant strabismus implies that the degree of misalignment is the same in all fields of gaze, contrasting with incomitant strabismus, in which the measured angle of the eye turn varies in the different fields of gaze.
Incomitant strabismus can vary in the horizontal or vertical plane, or both. If a horizontal misalignment (esotropia or exotropia) differs in the upgaze and downgaze positions, this leads to pattern strabismus (including A, V, Lambda, Y, or X patterns). A misalignment, either horizontal or vertical, that changes when shifting from the right to left gaze positions generates a horizontal incomitance. Finally, if a vertical misalignment (hypertropia or hypotropia) changes on fixating from upgaze to downgaze, this is termed a vertical incomitance.
Incomitant strabismus can be classified etiologically into innervational and mechanical forms. Innervational entities include innervation deficits (paresis or palsy), which can be supranuclear, nuclear, or infranuclear. Excess innervation of muscles may also occur. Mechanical causes imply restrictions due to problems within the orbit, and these can include abnormalities in the muscles, soft tissues, or bones, as well as lesions within the socket. Restrictions can be caused by congenital disorders or they can be acquired as a result of trauma, surgery, systemic disorders, or other problems.
I. Comitant Strabismus
a) Esotropia
 Figure 1.1 Infantile Esotropia Infantile esotropia, also referred to as essential infantile esotropia or by the older term congenital esotropia, presents as a manifest deviation with onset before 6 months of age. The angle of deviation is usually over 30 prism diopters. The eye movements are full in the vertical and horizontal planes except for mildly limited abduction of the right eye. As these children often cross-fixate, using the adducted eye to view the contralateral field rather than abducting the ipsilateral eye, it can be difficult to elicit full abduction. A rapid Doll head maneuver or patching the nontested eye may be required to elicit abduction. Infantile esotropia is also associated with inferior oblique overaction (note left eye in upgaze; also see Fig. 1.31), dissociated vertical deviation (Figs. 1.19 and 1.20), latent nystagmus, and, less commonly, manifest nystagmus. |
 Figure 1.2 Alternating Fixation The top photo shows that when the right eye fixates there is a left esotropia. The bottom photo shows that when the left eye fixates a right esotropia is present. With alternating fixation the deviation switches back and forth from a left esotropia to a right esotropia. This indicates equal vision in each eye (no fixation preference). If the vision were better in one eye, then covering that eye would result in temporary fixation by the fellow eye. That eye would then revert to the esotropic position as soon as the cover was removed from the better eye as the preferred eye takes up fixation. Note also the position of the corneal light reflex (Hirschberg reflex), which is always more lateral relative to the visual axis in the esotropic eye and more central in the fixating eye. |
 Figure 1.3 Ciancia Variant with Cross-Fixation One subgroup of infantile esotropia, the Ciancia variant, shows nystagmus on attempted abduction of either eye. When fixating with either eye the child adopts a face turn in order to fixate with the eye in the adducted position: In that position the nystagmus dampens. The left photo shows the child fixating with the right eye in adduction, and the right photo shows him fixating with the left eye in adduction. The marked nystagmus on lateral gaze serves to distinguish the Ciancia variant from the more common cross-fixation of infantile esotropia not associated with nystagmus. |
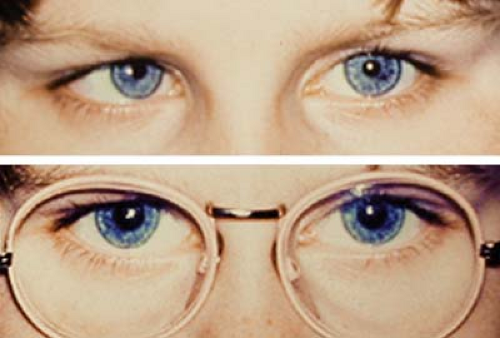 Figure 1.4 Accommodative Esotropia with and without Glasses The top photo shows a patient with a large right esotropia. The patient has a hyperopic cycloplegic refraction of +4.00. The bottom photo shows the patient wearing glasses and the correction, in which the eyes are straight. The esotropia is now controlled, confirming that this child has accommodative esotropia. Approximately one third of these patients will always need hyperopic correction (glasses or contact lenses) to maintain straight eyes, one third can be tapered out of their correction, and one third will need strabismus surgery because of the development of a nonaccommodative component. |
 Figure 1.5 Partially Accommodative Esotropia This girl is wearing glasses that correct all of her hyperopia as measured during atropine refraction. The atropine cycloplegia ensures that the full hyperopic refraction is measured. This is particularly important when correction of the nonatropine cycloplegic refraction does not lead to complete straightening of the eye. While wearing the glasses she has a small residual right esotropia, representing the nonaccommodative portion of her esodeviation. Surgery is required to correct the nonaccommodative portion of the strabismus. The child would still wear spectacles postoperatively to correct the accommodative portion of the deviation to keep the eyes straight. |
 Figure 1.6 Esotropia with Convergence Excess The top photo shows the patient fixating in the distance, where there is no strabismus. The lower photo shows her fixating at one-third meter on an accommodative target: Her left eye deviates inward. This convergence excess form of esotropia can be a subtype of accommodative esotropia, due to the high accommodative convergence–to–accommodation (AC/A) ratio. Convergence excess may also occur with a normal AC/A ratio. The gradient method of determining the AC/A ratio would distinguish between the two possibilities. If the deviation is reduced to zero or close to zero at near with a reading add, this may also suggest a high AC/A ratio. |
 Figure 1.7 Accommodative Esotropia with High Accommodative Convergence–to–Accommodation (AC/A) Ratio Treated with Bifocals The upper image shows the child fixating on an accommodative target in the near position (one-third meter) while looking through the distance portion (upper segment) of the glasses: There is an esotropia. The lower image shows him looking at the same target, but now through the add (lower segment) at near: The deviation is eliminated. This child has a high AC/A ratio. The bifocal add is correcting the excess deviation that occurs at near. Note that the bifocal is executive style and set high enough so that the child can easily fixate through the add in the near fixation position. It is recommended that the top of the segment be set no lower than the inferior edge of the pupil when the patient is fixating in the distance. |
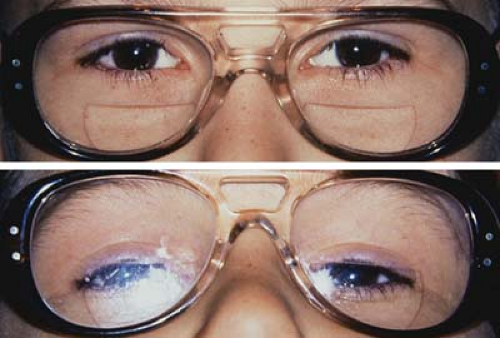 Figure 1.8 Bifocals Set Too Low The upper image shows the bifocal set several millimeters below the lower eyelids. The child is viewing a distance target with full hyperopic correction for his accommodative esotropia: The eyes are straight. The lower image shows the child fixating through the bifocal in the near position. While the add is effective in maintaining good alignment for the excess near deviation (convergence excess, see Fig. 1.6), the child has to use an awkward chin-up head posture to be able to use the bifocal segment. Figure 1.7 demonstrates proper spectacle construction for this disorder. |
 Figure 1.9 Pseudoesotropia The wide flat nasal bridge and the prominent epicanthal folds in this Asian child result in covering of the nasal sclera of the left eye particularly when the child is fixating slightly in right gaze. These features combine to give the impression of an esotropia. However, the corneal light reflexes (Hirschberg reflex) are symmetrically centered in each eye, thus ruling out the presence of a manifest deviation. There is no strabismus on the cover test. |
 Figure 1.10 Negative Angle Kappa In this photo the patient is fixating with her right eye. However, the light reflex in that eye is located slightly temporal within the pupil when compared to the centered reflex in the left eye, giving the child the appearance of a right esotropia. A cover test will show no movement of the right eye on covering the left eye, indicating that there is no strabismus. The off-centered light reflex persists under monocular conditions in the right eye. This is due to a negative angle kappa: A disparity between the visual axis (joining target and fovea) and the anatomic pupillary axis (joining midpupil to fovea). (Compare to Fig. 1.18, positive angle kappa.) |
 Figure 1.11 Factitious Esotropia This photo shows a marked symmetrical convergence in a patient who has recently had cycloplegic drops placed in both eyes (note that both pupils are dilated). When the patient is asked to focus on a near target the failed attempt at accommodation induces convergence. The light reflex is symmetric in each eye, so there is no true esotropia: The eyes are aligned when fixating on the near target. Convergence spasm in hyperopic noncyclopleged patients presents with a similar clinical appearance except that the pupils are constricted due to the near synkinesis. Convergence spasm can also be associated with psychological disorders. |
b) Exotropia
 Figure 1.12 Basic Exotropia This child is fixating with the right eye. There is a left exotropia. The angle of deviation is the same on distance and near measurements, representing a basic exotropia. Note that the corneal light reflex (Hirschberg reflex) now appears more nasal relative to the pupil center as compared to the more central reflex in the fixating right eye. As this is a comitant deviation (same amount of deviation in all positions of gaze), the eye movements of both eyes in all directions are equal and full. |
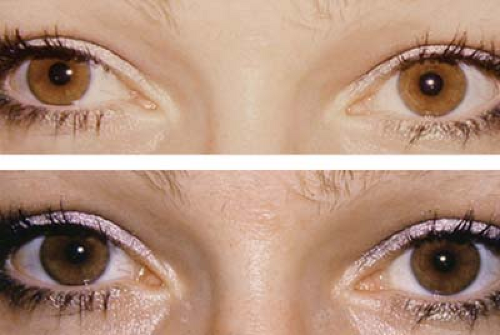 Figure 1.13 Divergence Excess Exotropia The top photo shows the patient fixating in the distance: The right eye diverges. The lower photo shows the patient fixating at near, where the eyes are straight. This patient therefore has a divergence excess exotropia. However, if after 45 minutes of occlusion of the right eye the deviation at near increases to equal, or almost equal, the distance measurement, then the patient has a simulated divergence excess exotropia. The implication is that fusional convergence is keeping the eyes straight at near. If the near deviation increases through plus lenses held over the two eyes, then it also indicates the presence of a simulated divergence excess, on the basis of accommodative convergence, which is keeping the eyes aligned at near. |
 Figure 1.14 Convergence Weakness Exotropia The upper photo shows a young child who has a 10 prism diopter right exotropia while fixating at distance. The lower photo shows the child fixating at near, where the right exotropia is larger. When there are little or no deviation at distance and an exodeviation at near accompanied by a decreased near point of convergence, with reduced convergence amplitudes, the convergence weakness is often termed convergence insufficiency. This form of exodeviation may respond to convergence exercises. Convergence insufficiency can also occur in the absence of an actual exodeviation. |
 Figure 1.15 Sensory Exotropia The photo shows a patient with a dense cataract in the left eye, which precludes binocular vision. Strabismus is common in older children and adults with long-standing sensory deprivation or vision loss due to cataracts or other eye disorders. In younger children sensory esotropia is more common with an incidence almost equal to sensory exodeviation. Sensory esotropia is rare in older children and adults. Surgical correction of sensory deviations is particularly challenging because in many cases there will be a tendency for the poorly seeing eye to drift out of alignment again. |
 Figure 1.16 Infantile Exotropia The photo shows an infant with a large-angle right exotropia, which presented before the age of 6 months. Infantile exotropia, also known as essential or congenital exotropia, is much rarer than infantile esotropia (Fig. 1.1). The exodeviation is usually very large, almost always over 40 prism diopters. Infantile exotropia has also been reported in association with various neurologic and developmental disorders. |
 Figure 1.17 Exotropia with Refractive Error The top image shows a child with a left exotropia when she does not wear her myopic spectacles. The bottom image shows that her eyes are straight when she wears her glasses. The improvement is likely due to a combination of accommodative convergence and stronger fusional convergence. Improved control of exotropia can also be seen in patients with moderate or high hyperopia who are given their hyperopic correction. Without glasses the patient may choose not to accommodate fully and the exotropia manifests due to lack of fusion and accommodative convergence. When the patient wears the hyperopic correction, fusional convergence may improve, leading to straight eyes. |
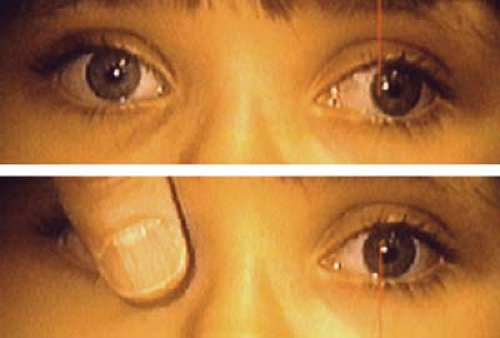 Figure 1.18 Positive Angle Kappa (Pseudoexotropia) The top photo shows a patient with an apparent left exotropia. The corneal light reflex in the fixating right eye is central. The bottom photo shows the patient’s right eye being covered to force fixation with the left eye, which has a vision of 6/6. However, in both images the light reflex in the left eye remains located slightly nasal within the pupil, giving the child the false appearance of a persisting left exotropia. Pseudoexotropia is particularly common following retinopathy of prematurity complicated by a temporal dragging of the macula. To fixate with the fovea, the eye must be held in a turned-out position as the disparity between the visual and anatomic pupillary axes is exaggerated. |
II. Dissociated Deviations
a) Dissociated Vertical Deviation
 Figure 1.19 Unilateral Dissociated Vertical Deviation (DVD) The upper image shows a right hypertropia when the left eye fixates. The middle image shows the left eye being covered to force fixation with the right eye. In the lower image, the right eye continues to fixate but there is no manifest hypotropia of the left eye, confirming the diagnosis of unilateral right DVD. In dissociated vertical deviations, one eye is moving independently of the other (nonyoked innervation) in contrast to “true” vertical deviations, in which a switch of fixation to the hypertropic eye always results in an equal downward deviation of the fellow eye (yoked innervation). DVD with a downward drift has also been rarely reported. |
 Figure 1.20 Bilateral Dissociated Vertical Deviation (DVD) The upper photo shows that when the patient fixates with the left eye the right eye drifts upward and outward. The lower photo shows that when she fixates with the right eye the left eye drifts upward and outward. Indirect ophthalmoscopy showed excyclotropia of the hyperdeviated eye in each instance. These findings confirm the presence of bilateral DVD. Note that there is never a hypotropia of the fixating eye when fixation is switched (Fig. 1.19). If a patient presents with a latent or manifest DVD in one eye, patching of the fellow eye for several minutes may bring out a bilateral DVD that was not apparent on initial examination. In side gaze, fixation by the adducting eye can be blocked by the nose, causing that eye to drift upward. To differentiate this from overaction of the inferior oblique (Fig. 1.31), a cross-cover test will fail to show a hypotropia of the abducting eye in DVD. |
b) Dissociated Horizontal Deviation
 Figure 1.21 Dissociated Horizontal Deviation (DHD) The upper image shows a child with a right exotropia when he fixates with the left eye. This horizontal deviation becomes manifest when there is a lack of visual attention or a disruption in fusion. In the lower image, the child is fixating with his right eye, yet there is no manifest exotropia of the left eye. There is a symmetric low hyperopic refractive error in the two eyes, leading to symmetric accommodative demand for the two eyes. These findings suggest a right dissociated horizontal exodeviation. Most cases of DHD are exodeviations. Dissociated esodeviations are much less common. |
III. Incomitant Strabismus: Patterns
a) A-pattern Strabismus
 Figure 1.22 A-pattern Exotropia with Overaction of the Superior Obliques The photos show the nine diagnostic positions of a patient with an exotropia in primary position (center photo). The exotropia increases significantly on direct downgaze, while on upward gaze the deviation is much smaller. The overactions of the superior obliques are evident on gazes into the down-right and down-left positions. There is mild underaction of both inferior oblique muscles evident in the upper right and upper left photos. |
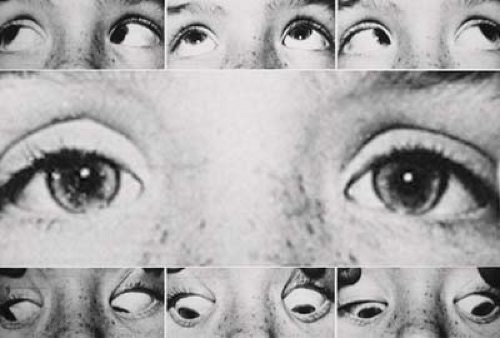 Figure 1.23 A-pattern Exotropia without Overaction of the Superior Obliques This patient has a small exotropia in primary position (center photo) that is larger on downgaze and less on upgaze. There is no overaction of the superior oblique muscles (lower right and lower left images). |
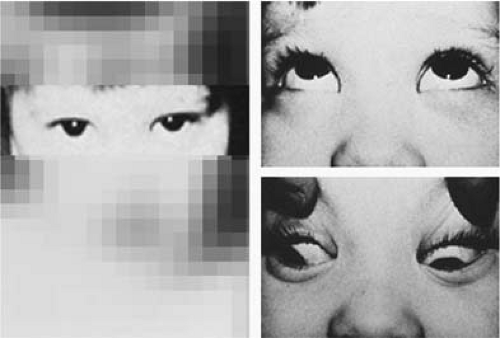 Figure 1.24 Head Posture with A-pattern Exotropia The left photo shows the child with a chin-down head posture, viewing straight ahead with eyes in upgaze. The top right photo shows normal alignment in the upgaze position while the bottom right photo shows a large exotropia on downgaze. The chin-down position allows the child to maintain binocular vision. |
 Figure 1.25 A-pattern Esotropia with Overaction of the Superior Obliques This patient shows an esotropia in primary position (center photo). The esotropia is markedly reduced on downgaze and increases significantly on upgaze. The superior obliques are overacting as seen in the lower right and lower left gaze positions where the adducting eye is relatively hypotropic. The inferior oblique muscles are underacting, as seen in the upper right and upper left gaze positions where the adducting eye is also relatively hypotropic. |
 Figure 1.26 A-pattern Esotropia without Overaction of the Superior Obliques This patient has an esotropia in primary position (center photo) that is markedly reduced on downgaze and increases significantly on upgaze. However, the superior and inferior oblique muscle actions are normal. |
 Figure 1.27 Head Posture with A-pattern Esotropia
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|