Child Abuse
Alex V. Levin
Child abuse is often categorized into four subgroups: physical abuse, sexual abuse, child neglect, and emotional abuse. All types of child abuse may have ocular manifestations. It is estimated that 4% to 6% of all child abuse cases will first present to an ophthalmologist. In most developed countries, ophthalmologists would be considered mandated reporters of suspected child abuse. The suspicion need not be proven by the physician. Child protective agencies, the judicial system, and the police are entities responsible for determining whether the suspicion is validated and, if so, determining who the perpetrator is. The ophthalmologist’s responsibility is to report the ocular manifestations and the degree of certainty to which these findings support a diagnosis of abuse.
Inflicted eye injuries may be isolated, part of the battered child syndrome, or secondary to shaken baby syndrome. Long-term outcomes in abused children include visual loss due to amblyopia, injury, and the sequelae of brain injury (e.g., cortical visual impairment, visual field loss). Children who are victims of sexual abuse may experience the ocular effects of sexually transmitted disease (e.g., cytomegalovirus due to HIV infection [Chapter 19: Infectious Diseases, Figs. 19.9, 19.10 and 19.11]). Noncompliance and neglect are frequent problems in the ophthalmic care of children. Ophthalmologists will often see parents missing appointments made for their child and failing to comply with prescribed therapy such as patching without any apparent reason for doing so, such as financial or child care obstacles. Nonorganic failure to thrive, also known as psychosocial dwarfism, is a more dramatic and systemic manifestation of child neglect. Lastly, emotional abuse may have its ocular manifestation in what children are allowed to see. In today’s society, children are increasingly and inappropriately exposed to graphic if not real images of sexual activity, drug abuse, and violence. Emotional abuse also entails severe verbal belittlement and harsh discipline.
It may be difficult to draw distinct lines along the continuums that describe the many behaviors referred to as child abuse. In some cultures, actions such as spanking, coining, and even shaking may be acceptable practices. Marriage and sexual intercourse with young adolescents are accepted in some cultures as well. Child care practices and means of discipline vary widely around the world. However, as ophthalmologists, we must uphold a standard that protects children from harm and rely on public systems and personal advocacy aimed at following through on our suspicions in any individual case that a child may indeed be at risk for, if not already a victim of, child abuse.
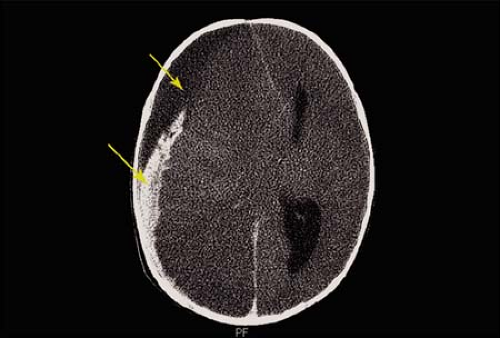 Figure 12.1 Shaken Baby Syndrome—Brain Injury Shaken baby syndrome is a form of physical abuse in which the perpetrator submits a child to violent acceleration–deceleration forces with or without impact of the head. Characteristic brain injuries include subdural hemorrhage (arrows). This child’s imaging suggests blood of two separate ages. The hemorrhage size is compressing the brain, causing a shift of the midline and obliteration of the ventricles. There is also diffuse severe cerebral edema with loss of gray-white differentiation. Other brain injuries in shaken baby syndrome include subarachnoid hemorrhage and, less commonly, parenchymal hemorrhage or contusion and brain laceration. |
 Figure 12.2 Shaken Baby Syndrome—Brain Injury Approximately 25% to 35% of the victims of shaken baby syndrome die and another third survive with long-term neurologic sequelae including visual loss or blindness, cerebral palsy, and mental retardation. This image demonstrates the cerebral atrophy that may occur. The most common cause of visual loss following inflicted childhood neurotrauma is cortical visual impairment due to coup or contrecoup contusion of the occipital lobes or infarction of the posterior cerebral circulation as a result of severe cerebral edema. |
 Figure 12.3 Shaken Baby Syndrome—Rib Fractures This child has numerous rib fractures, some of which are circled. In the “classic” form of shaken baby syndrome, the perpetrator grasps the child by the thorax and shakes him or her violently. There are usually no external signs of injury. Crying of an infant is the most common inciting event, and victims are usually less than 1 year old (although child victims as old as 5 years have been reported). Posterior and posterior–lateral rib fractures are the most common thorax injury. Other fractures occur when the child is grasped by a limb and shaken. This may result in stripping of the periosteum with subperiosteal hemorrhage and typical metaphyseal fractures, termed chip, corner, or bucket handle fractures of the long bones. |
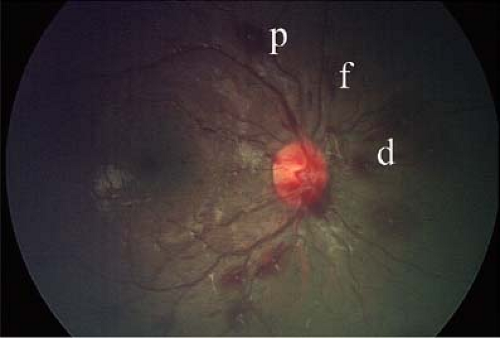 Figure 12.4 Shaken Baby Syndrome—Mild Retinal Hemorrhages Retinal hemorrhages are the characteristic ocular manifestation of shaken baby syndrome and perhaps the most common manifestation of physical abuse that an ophthalmologist will encounter. One must carefully describe the number, type, pattern, laterality, and distribution of the hemorrhages to best document and interpret the finding. Use of the generic term “retinal hemorrhages” is discouraged. This child shows a nonspecific hemorrhagic retinopathy characterized by a small number of intraretinal (nerve fiber layer [flame hemorrhage, f] more than deeper [dot/blot] hemorrhage, d) and preretinal, p hemorrhages confined to the peripapillary region. Although shaken baby syndrome may be the most common cause of this picture in an otherwise previously well infant, there are numerous other causes that should be considered. |
 Figure 12.5 Shaken Baby Syndrome—Moderate Retinal Hemorrhages As compared to Fig. 12.4, this child has a larger number of intraretinal and preretinal hemorrhages, which extend beyond the view of this photograph throughout the macula and almost to the midperiphery. Although this is more likely a victim of shaken baby syndrome, such patterns can also be seen after severe life-threatening accidental injury (e.g., motor vehicle accident), normal birth, and leukemia, and perhaps in rare cases as a result of other systemic diseases which are usually readily apparent. Note that this victim of shaken baby syndrome does not have papilledema. Papilledema occurs in less than 10% of cases.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|