Conjunctiva
Alex V. Levin
Thomas W. Wilson
David Rootman
Jerome Kazdan
The conjunctiva is derived from surface ectoderm and has an important role in maintaining ocular surface integrity. Goblet cells within the conjunctiva provide the inner layer of the trilaminar tear film for lubrication and surface wetting. Tumors of the conjunctiva are often benign but must be observed for possible malignant transformation. Conjunctival findings may assist in the diagnosis of systemic diseases, and conjunctival biopsy can be a useful diagnostic tool. As the conjunctival epithelium is contiguous with the corneal epithelium and vascular supply to the limbus is brought in part by the conjunctiva, it is not uncommon for conjunctival disease to coexist with corneal disease or anterior segment inflammation (iritis).
The conjunctiva also extends upward and downward to form the superior and inferior fornices where it reflects out onto the inner surface of the lids. Bulbar conjunctiva, which overlies the globe, may or may not be affected in some disorders. The same is true for palpebral conjunctiva. The fornices may serve as repositories for chemical or particular matter, and therefore, lid eversion is an essential part of complete conjunctival examination. Defects or foreign bodies in the conjunctiva can be detected by topical fluorescein staining, whereas rose bengal can be used to detect devitalized conjunctival epithelial cells.
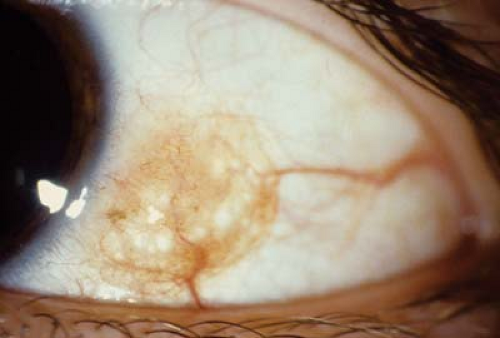 Figure 4.1 Amelanotic Nevus In childhood, most conjunctival nevi initially appear amelanotic and show little or no active melanin production until the pubertal years. Microcysts within the lesion are common. Prominent vessels leading to the lesion with telangiectasia within the nevus may also be seen. Conjunctival nevi are most commonly located in the perilimbal area in the interpalpebral fissure. Even though conjunctival nevi have a low chance of malignant transformation, nevi that are increasing in size or become more inflamed should be excised with cryotherapy at the base of the lesion. |
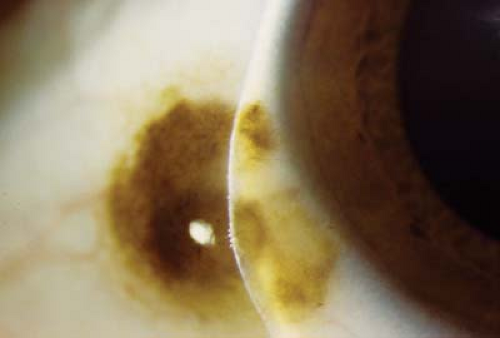 Figure 4.2 Melanotic Nevus Conjunctival nevi consist of melanocytic nevus cells classified based upon location within the epithelium. The nevus cells can be located in the epithelium (junctional nevus), subepithelium, or both layers (compound nevus). Most of the lesions are located near the limbus, are slightly raised, and can contain a variable amount of pigment. Lesions should be followed by serial photography. Although rare, malignant transformation can occur, especially in the teenage years. Signs of transformation include growth, formation of an elevated mass, increased feed vasculature, and extension into contiguous structures. |
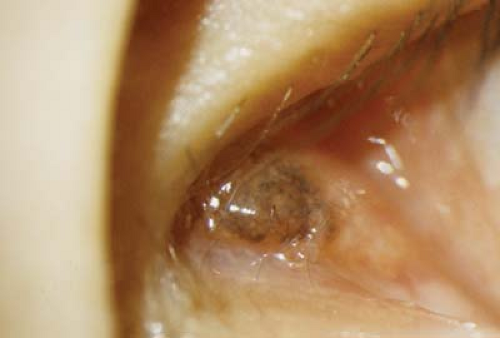 Figure 4.3 Caruncle Nevus A nevus located within the caruncle typically presents during puberty, contains small cysts, and does significantly change in size. The caruncle is an extension of the conjunctival tissue and serves little purpose in terms of ocular health. Surgical excision is recommended for pigmented lesions that are changing in size, gaining pigmentation, or associated with inflammation. |
 Figure 4.4 Axenfeld Loops Axenfeld loops are areas of pigmentation surrounding an intrascleral nerve or blood vessel. They are typically located a few millimeters posterior to the limbus and appear as variably sized, slate gray, pigmented patches circumferentially equidistant from the limbus. Under high magnification, the pigment appears as rectangular deposits at the level of the episclera. These lesions are a normal variant, benign, and of no ophthalmic concern. |
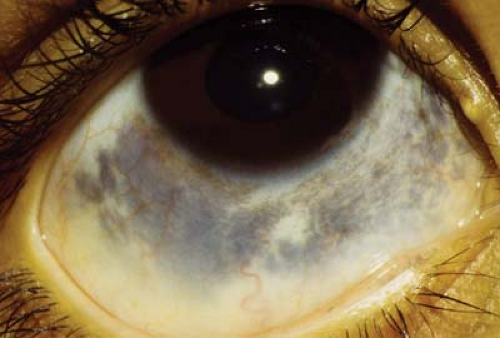 Figure 4.5 Ocular Melanosis Ocular melanosis is a form of episcleral pigmentation, usually slate gray, that tends to occur as broad patches with no anatomic correlate, unlike Axenfeld loops (see Fig. 4.4). This form of episcleral pigmentation is seen in darkly pigmented individuals and is not associated with malignant transformation. The lesions may be uni- or bilateral. Pigmentation does not move with the conjunctiva. |
 Figure 4.6 Oculodermal Melanocytosis The combination of ocular melanosis (see Fig. 4.5) and similar skin pigmentation, known as nevus of Ota, is called oculodermal melanocytosis. The skin has a bluish gray appearance. Other uveal structures, including the iris and retinal pigment epithelium, can have increased pigmentation (Fig. 4.7). Nevus of Ota is more common in darkly pigmented individuals and is typically unilateral. It is more common in certain ethnic groups, particularly in far eastern Asia. When found in the Caucasian population it has a higher incidence of associated malignancy, including choroidal melanoma. |
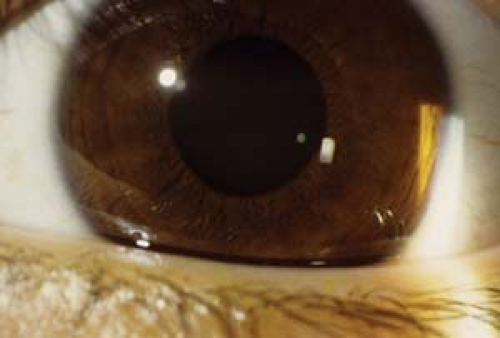 Figure 4.7 Iris Melanosis Iris melanosis is often associated with oculodermal melanocytosis (see Figs. 4.5 and 4.6). The usual iris crypts are missing, particularly in the peripheral two thirds of the iris. Instead, the iris appears flat with or without a large number of tiny bumps following no particular pattern. The iris tends to be chocolate brown, particularly when compared to the other eye. Gonioscopy is normal and there is no increased association with glaucoma. However, eyes with iris melanosis in the presence of oculodermal melanocytosis may have a higher risk of ocular melanoma. Malignant transformation is very rare in childhood.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|