Gastrointestinal
Alex V. Levin
Thomas W. Wilson
Stephen P
During development, neural crest migration to form the gastrointestinal tract and many of the ocular tissues occurs at similar times of gestation. As a result, some abnormalities of both systems may coexist. Yet, other coexisting abnormalities seem to have their basis in manifestations of a mutated gene that has a role in both locations that may be quite different and not embryologically based. Some gastrointestinal disorders also involve the eye as a complication of the primary problem, as seen with iron deposition in Wilson disease. Gastrointestinal disorders, such as Alagille syndrome, may be indications for eye examination both for diagnosis and for possible later complications. Some ocular findings, such as uveitis, should prompt the ophthalmologist to consider gastrointestinal manifestations that have yet to be recognized or diagnosed, such as inflammatory bowel disease.
 Figure 17.1 Inflammatory Bowel Disease—Episcleritis Inflammatory bowel disease is a term encompassing ulcerative colitis, Crohn disease, and overlap patients. It is a chronic gastrointestinal disorder with potential ophthalmic manifestations both related to the disease and secondary to its treatment. Patients can develop diffuse (seen in this image) or nodular episcleritis, and there may be a correlation with gastrointestinal disease activity. There may be associated mild nongranulomatous iritis. The episcleritis often responds to systemic treatment of the gastrointestinal disease, but topical treatment is useful, particularly when patients have pain and uveitis. |
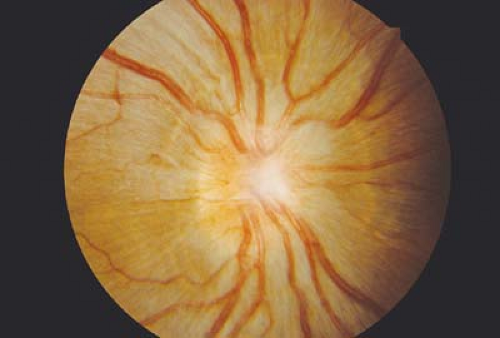 Figure 17.2 Inflammatory Bowel Disease—Scleritis Nodular and posterior scleritis are uncommon findings of inflammatory bowel disease. Nodular scleritis is more common in Crohn disease than ulcerative colitis and more severe when there is also arthritis involving large peripheral joints. Posterior scleritis causes severe pain and potential vision loss from optic nerve or retinal edema. The retinal folds and peripapillary elevation seen in this photograph are secondary to the severe scleral inflammation and thickening, mimicking a posterior retrobulbar mass. The sclera is thickened on B-scan ultrasound. |
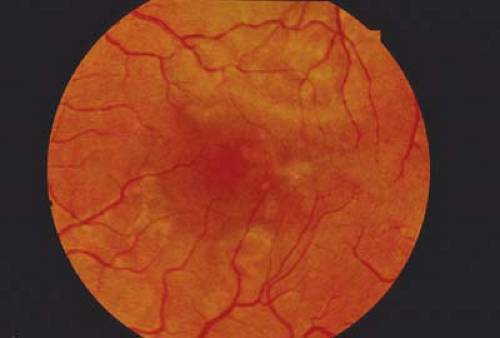 Figure 17.3 Inflammatory Bowel Disease—Chorioretinitis The white patches and areas of pigmentation seen in this image are the result of chorioretinitis and subsequent retinal pigment epithelium hypertrophy, respectively. Macular involvement can reduce the visual acuity. Papillitis (Chapter 9: Optic Nerve, Fig. 9.27) and retinal vasculitis are other uncommon manifestations of inflammatory bowel disease. Retinal vasculitis and chorioretinitis can coexist. Systemic treatment of the gastrointestinal disease with consideration of sub-Tenon deposteroids is recommended for the fundus manifestations of inflammatory bowel disease.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|