Stem Cell Transplantation for Ocular Surface Diseases
Scheffer C. G. Tseng
Edgar M. Espana
Mario A. Di Pascuale
BASIC CONCEPTS
OCULAR SURFACE HEALTH IS MAINTAINED BY A STABLE TEAR FILM
Anatomically, the ocular surface encompasses the entire mucosal epithelial lining bordered by the skin at the superior and inferior eyelid margins. Histologically, this epithelial surface covers two major territories (i.e., the cornea and the conjunctiva). The primary function of the ocular surface is to provide clear vision during an open-eye state. To achieve this goal while maintaining comfort and preventing microbial invasion, the ocular surface has to be covered by a stable tear film. Therefore, the mechanism by which the ocular surface health is ensured is inherently built into the relationship between ocular surface epithelia and the preocular tear film. As recently summarized,1 compositional factors including the ocular surface epithelia, meibomian glands, and lacrimal glands and hydrodynamic factors such as eyelid blinking and closure are essential to constitute ocular surface defense that governs how preocular tear film stability is maintained (Fig. 1). These two major factors are integrated via two neuronal reflex arcs, triggered by the sensory drive of the first branch of trigeminal nerve (V1), and mediated by the parasympathetic branch and the motor branch of the facial nerve (VII) as the efferent output, respectively (Fig. 2). Such a neuroanatomic integration of ocular surface defense explains how external adnexal glands and eyelids can be integrated with ocular surface epithelia as a unit to maintain a stable tear film.
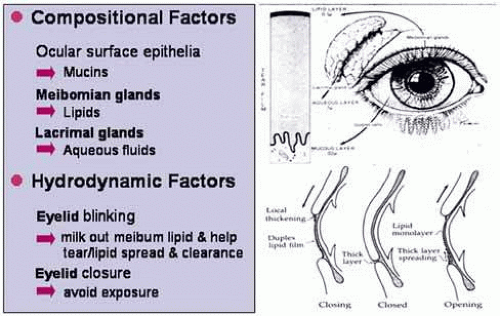 Fig. 1 Ocular surface defense. Ocular surface health is maintained by a stable tear film, which requires both compositional and hydrodynamic factors. The former includes ocular surface epithelium producing mucins, meibomian glands producing meibum, and lacrimal glands producing aqueous tears. The latter includes eyelids, which blink at desirable frequencies to allow tears to spread and clear, and close completely during the close eye state to prevent evaporation. |
 Fig. 2 Neuroanatomic integration of compositional and hydrodynamic factors. Two neuronal reflexes are involved to integrate both factors as an integral unit to maintain a stable tear film. Both reflexes are triggered by the sensory input of the first branch of the trigeminal nerve (V1), while the compositional one is mediated by the parasympathetic branch of the facial nerve (VII), and the hydrodynamic one is mediated by the motor branch of the facial nerve. |
Based on this concept, one predicts that deficiency or alteration of any of these elements involved in such neuroanatomic integration can lead to an unstable tear film, a hallmark of various forms of dry eye.2 Therefore, investigation into dysfunction of this neuroanatomic integration is the first step toward better understanding of the pathogenesis of various ocular surface disorders, and is a prerequisite before any ocular surface reconstruction.
TWO TYPES OF OCULAR SURFACE FAILURE
SQUAMOUS METAPLASIA
According to the resultant epithelial phenotype defined by impression cytology 3, all severe ocular surface diseases can be classified to express one of the two major types of ocular surface failure. The first type is squamous metaplasia (Fig. 3) in which a normal nonkeratinized ocular surface epithelium transforms into a skin-like keratinized epithelium.3 Because of skin-like epithelial differentiation (skin-like), the ocular surface with squamous metaplasia becomes nonwettable, a hallmark of various dry eye disorders.2 If the underlying insults are primarily derived from poor ocular surface defense, such squamous metaplasia can be reversed to a normal state when ocular surface defense is restored, indicating that epithelial progenitor cells (i.e., stem cells) of the ocular surface are not intrinsically altered. Squamous metaplasia can be caused by insults not originating from ocular surface defense. In xerophthalmia caused by systemic vitamin A deficiency,4,5 squamous metaplasia can also be reversed by replacement of vitamin A. Nevertheless, squamous metaplasia can also be caused by various insults damaging epithelial progenitor cells, the basement membrane, and the underlying stroma leading to chronic inflammation and scarring as seen in various forms of cicatricial keratoconjunctivitis such as chemical burns, Stevens-Johnson syndrome, ocular pemphigoid, etc.6,7 Except for early active ocular cicatricial pemphigoid, in which systemic immunosuppression can reverse squamous metaplasia, the rest cannot be reversed by conventional medical treatments. The irreversibility of such abnormal epithelial differentiation strongly implies that epithelial progenitor cells (i.e., stem cells [SC]), may have been intrinsically altered.
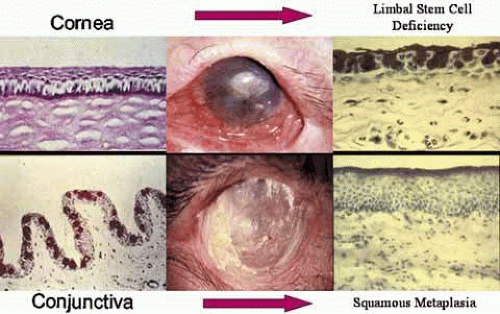 Fig. 3 Two types of ocular surface failure. In limbal stem cell deficiency, the corneal epithelium is replaced by conjunctival epithelium, while in squamous metaplasia corneal and conjunctival epithelia transform into a keratinized (skin-like) epithelium. In addition to the change in epithelial phenotype, both types of ocular surface failure are also accompanied by the destruction of the basement membrane and the inflammation and scarring of the underlying stroma. |
LIMBAL STEM CELL DEFICIENCY
The second type of ocular surface failure is limbal stem cell deficiency (LSCD) (Fig. 3), which is characterized by the replacement of the normal corneal epithelium by an invading conjunctival epithelium.8 This pathologic state of LSCD can experimentally be created in rabbits by damaging the limbal epithelium, which contains corneal epithelial SC.9 Corneas with LSCD manifest poor epithelialization (persistent defects or recurrent erosions), chronic stromal inflammation (keratitis mixed with scarring), corneal vascularization, and conjunctival epithelial ingrowth. Consequently, patients with LSCD experience severe irritation, photophobia, and decreased vision, and are poor candidates for conventional corneal transplantation. Because most of these features can also be found in other corneal diseases, the sine qua non criterion for diagnosing LSCD is the existence of conjunctival epithelial ingrowth onto the corneal surface (conjunctivalization). Clinically, the presence of conjunctivalization may be suggested by observing the loss of limbal Vogt’s palisades under slit-lamp examination10 and by occurrence of late fluorescein staining,11 reflecting poor epithelial barrier function.12 However, the definitive diagnosis of conjunctivalization relies on the detection of conjunctival goblet cells on the corneal surface by impression cytology.8 Accurate diagnosis of LSCD is crucial to guide the choice of appropriate procedures for transplanting limbal epithelial SC.
Based on the underlying etiology, corneal diseases manifesting LSCD can be subdivided into two major categories (Table 1).8 In the first category, limbal epithelial SC are destroyed by known or recognizable offenders such as a chemical or thermal burn, Stevens-Johnson syndrome/toxic epidermal necrolysis, multiple surgeries or cryotherapies or medications (iatrogenic), contact lens, severe microbial infection, radiation, and antimetabolites including 5-fluorouracil and mitomycin C.8,13,14,15 A second category is characterized by a gradual loss of the SC population without known or identifiable precipitating factors. In this situation, the limbal stromal niche is presumably affected and progressively deteriorates by a variety of etiologies that include aniridia and coloboma, neoplasia, multiple hormonal deficiencies, peripheral ulcerative corneal diseases, neurotrophic keratopathy and idiopathic limbal deficiency.8,10,16,17,18 These diseases can also be categorized by the underlying cause being hereditary or not as summarized in Table 1. The aforementioned information explains why transplantation of epithelial SC and restoration of SC stromal environment is necessary in ocular surface reconstruction.
TABLE 1. Ocular Surface Diseases with Limbal Stem Cell Deficiency | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
KEY STRATEGIES
Considering all of the basic concepts together, we propose that the general strategy of ocular surface reconstruction is analogous to growing a flowering plant in the garden (Fig. 4). Several key strategies are undertaken: (1) to restore ocular surface defense so that a stable tear film can be maintained, analogous to providing rain/water; (2) to restore stromal substrate that is important to support existing or transplanted epithelial SC, analogous to providing a top soil; and (3) to restore epithelial SC, analogous to providing a good seed. These strategies are similarly applied to corneal and conjunctival surface reconstruction. Two major threats to successful ocular surface reconstruction are severe deficiencies in ocular surface defense leading to the lack of tear film protection and chronic inflammation or ischemia in the stroma that continue to damage the stromal substrate.
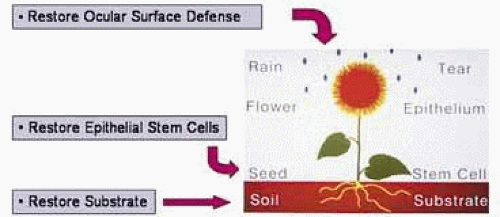 Fig. 4 General strategies of ocular surface reconstruction. Similar to growing a flowering plant in a garden, ocular surface reconstruction requires restoration of ocular surface defense to maintain a stable tear film (like rain), restoration of epithelial stem cells (SC; like seed), and restoration of stromal substrate (like soil). (Modified from Tseng SCG, Tsubota K: Important concepts for treating ocular surface and tear disorders. Am J Ophthalmol 124:825, 1997, with permission) |
FIRST STRATEGY: RESTORE OCULAR SURFACE DEFENSE
Before reconstruction, one should realize that keratinization in squamous metaplasia and vascularization in LSCD are two important pathologic mechanisms to prevent such corneal complications as epithelial defects, ulcers, or melt in eyes without an unstable tear film. Therefore, one should avoid performing conventional corneal transplantation to correct these two types of corneal failures if the ocular surface defense cannot first be restored. Because ocular surface reconstruction aims to restore a clear avascular cornea, which will require a stable tear film to maintain its health (see “Basic Concepts” section), it is of utmost important to restore a sound ocular surface defense. If not restored or unable to be restored, poor ocular surface defense in these eyes represent a contraindication for corneal surface reconstruction with epithelial SC transplantation.
Deficiencies in ocular surface defense can be recognized by history taking, and external and biomicroscopic examinations, and by the use of special tests such as dynamic tear function test, dye staining and impression cytology. Measures taken to correct severe aqueous tear deficiency dry eye include punctal occlusion and frequent application of autologous serum drops for mechanical microtrauma caused by lid margin and lash abnormalities such as trichiasis, entropion, or meibomian gland orifice metaplasia, which can be corrected by high oxygen permeability (Dk) contact lens, scleral contact lens, or appropriate plastic surgeries including mucous membrane graft. Symblepharon that causes obliteration of tear meniscus, misdirected lashes, inability of adequate blinking and closure, and motility restriction should also be corrected by fornix reconstruction before corneal surface reconstruction. Exposure problems may be corrected by Botox-induced ptosis, high DK contact lens, scleral lens, or tarsorrhaphy.
SECOND STRATEGY: RESTORE STROMAL ENVIRONMENT
The state and severity of LSCD can be graded as partial or total. In partial LSCD, a portion of the limbal SC remains intact. In partial or total LSCD, if the central cornea still preserves a normal corneal epithelial phenotype and satisfactory vision, treatments should be directed to maintaining the remaining corneal epithelium and to activating the remaining limbal SC. Besides bandage contact lens or scleral lens to shield against continuous attrition, one new way of expanding remaining limbal or conjunctival epithelial SC in vivo is to transplant preserved amniotic membrane to restore stromal environment that has been destroyed in diseases mentioned in Table 1.
Amniotic membrane (i.e., the innermost layer of the placental membrane) consists of a simple epithelium, a thick basement membrane, and an avascular stroma. When appropriately procured and processed, cryopreserved amniotic membrane can be used as a surgical graft for substrate replacement and does not elicit immunologic reactions.19 A number of studies have shown that amniotic basement membrane facilitates epithelialization and maintains epithelial phenotype, while amniotic avascular stroma exerts anti-inflammatory, antiangiogenic and antiscarring effects [for reviews see Dua and Azuara-Blanco,20 Kruse et al.,21 Sippel et al.,22 and Tseng and Tsubota23), properties important for reconstruction of epithelium-lining tissues. For partial LSCD, debridement of conjunctivalized epithelium from the corneal surface24 with or without additional amniotic membrane transplantation25 is effective to restore the corneal surface. Because of its anti-inflammatory effect, amniotic membrane transplantation as a temporary patch (bandage) is also effective in restoring ocular surfaces during the acute attack of chemical burns26 and Stevens-Johnson syndrome27.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


