Chapter 59 Standard Bilateral Parathyroid Exploration
Modern management of parathyroid disease has evolved with the influence of several fundamentally new and important factors. First is the reality that primary hyperparathyroidism (primary HPT) is no longer a rare endocrine disorder but the most common cause of hypercalcemia in the outpatient population, with estimated prevalence of 1 in 500 women and 1 in 2000 men.1 A second and related factor is a higher prevalence of asymptomatic primary HPT, where a clear biochemical diagnosis of parathyroid disease exists without noticeable symptoms or clinically detectable consequences, such as bone density loss or kidney stones.2 Among other reasons, more patients are being diagnosed in such an asymptomatic phase of the disease because calcium has become a routine component of automated chemistry panels, leading to incidental detection of symptomatic hypercalcemia. Conversely, more practitioners are also recognizing the need to screen patients with osteoporosis, osteopenia, and kidney stones for underlying primary HPT, utilizing not just calcium, but a panel that includes calcium, intact parathyroid hormone (PTH), and 25-hydroxyvitamin D levels (see Chapter 56, Primary Hyperparathyroidism: Pathophysiology, Surgical Indications, and Preoperative Workup). Finally, perhaps the most visible change in the landscape of parathyroid disease management is the paradigm shift toward focused parathyroid surgery—the exploration of a single site of suspected parathyroid gland abnormality.3 Most parathyroid surgeons have adapted this as the favored initial approach to parathyroid surgery, guided by radiologic studies and intraoperative PTH measurement (see Chapters 57, Guide to Preoperative Parathyroid Localization Testing, 60, Minimally Invasive Single Gland Parathyroid Exploration, 61, Minimally Invasive Video-Assisted Parathyroidectomy, 62, Local Anesthesia for Thyroid and Parathyroid Surgery, 63, Intraoperative PTH Monitoring during Parathyroid Surgery, and 64, Radio-Guided Parathyroid Exploration).
This chapter, however, is devoted to the approach of a standard, “bilateral” parathyroid exploration. This technique of achieving the surgical cure of PHPT was the original operative approach preferred from the 1920s through the late 1990s. It has been also been described as “conventional” or “traditional” parathyroidectomy, and the authors have also referred to it as “comprehensive.” At its essence, this approach can be defined as the examination of all parathyroid glands bilaterally with appropriate resection of diseased glands. It is imperative to recognize that “conventional” or “bilateral” parathyroid procedures are not obsolete but in fact remain essential and are at the core of successful parathyroid surgery. Bilateral parathyroidectomy will remain integral to the surgical treatment of PHPT and, for appropriate patients, is the ideal initial operation. It is also important to recognize that bilateral parathyroid examination can be performed in a minimally invasive manner. This approach requires a thorough understanding of parathyroid gland anatomy and embryology and of specific indications based on clinical presentation, parathyroid imaging, and intraoperative findings. In this chapter, we provide the rationale for and method of bilateral parathyroid exploration, illustrated with relevant clinical examples and a strategy for addressing the problematic circumstance of finding a “missing gland” (see also Chapter 58, Principles in Surgical Management of Primary Hyperparathyroidism).
Anatomy and Embryology Relevant for Bilateral Parathyroid Exploration
There are typically four parathyroid glands in most individuals, and thus bilateral exploration ideally aims to identify all four (see Chapter 2, Applied Embryology of the Thyroid and Parathyroid Glands). A large autopsy study identified four parathyroid glands in 84% of human cadavers, five or more glands in 13%, and only three parathyroids in 3%.4,5 Supranumerary parathyroids are most often located in the thymus. The possibility of having an unusual number or location of parathyroid glands has direct impact on the success of parathyroid surgery and the potential need for bilateral parathyroidectomy, yet it remains difficult to predict such anomalies reliably. The potential for missed ectopic or supranumerary parathyroids and persistent or recurrent hyperparathyroidism should be discussed with patients prior to surgery to properly inform expectations of surgery.
The key aspects of parathyroid anatomy and embryology to adapt to bilateral parathyroidectomy are illustrated in Figures 59-1 to 59-3. Normal parathyroid glands are approximately 5 to 6 mm in greatest dimension, weigh 15 to 35 mg, and can be inconspicuous with their orange-tan color embedded or flattened within a surrounding yellow fatty tissue envelope. The appearance of parathyroids can be variable even when they are biochemically functioning normally. When diseased, parathyroid glands may display variable morphologic changes in size, shape, texture, and firmness. Abnormal parathyroids are generally fuller in all dimensions, have a darker brown or reddish-brown color, and do not compress easily or are significantly firm when gently probed. They may have an irregular and knobby shape, more prominent vascular pedicles, or a plexus of vasculature. Glands of patients with secondary and tertiary hyperparathyroidism may be sclerotic and light in color from this fibrosis.
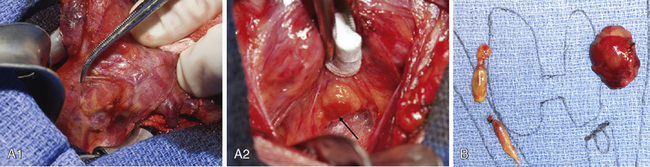
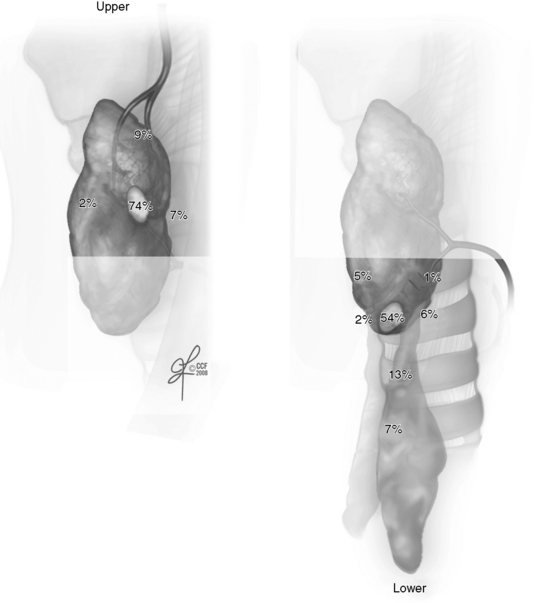
Figure 59-2 Normally expected distribution of upper and lower parathyroid glands.
(Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2008-2011. All rights reserved.)
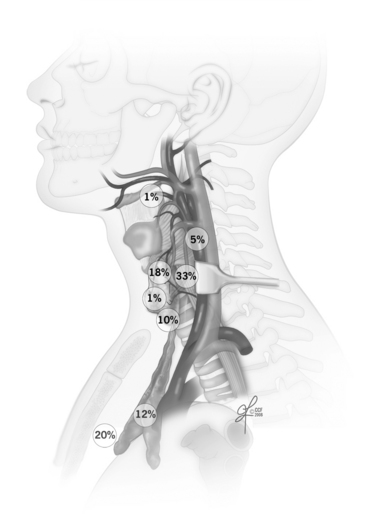
Figure 59-3 Distribution of ectopic parathyroid glands.
(Reprinted with permission, Cleveland Clinic Center for Medical Art & Photography © 2008-2011. All rights reserved.)
In cases of borderline abnormal appearance, it is helpful to determine in vivo parathyroid weight prior to excision of the parathyroid. This can be readily done by measuring parathyroid length (L), width (W), and height (H) using a small ruler or micrometer device without removing the gland. Because most glands are oval, calculating the volume of an ellipsoid using sizes in millimeters estimates parathyroid gland weight in milligrams (weight [mg] ≈ L × W × H ×½) [mm3]). We have observed that the metric of the total volume of diseased glands (TVDG) is statistically the same, whether the surgical findings are single or multigland parathyroid disease.6 In other words, the size of a typical single adenoma will be similar to the additive size (by volume or weight) of both double adenomas or of four hyperplastic glands. This implies that there ought to be caution for the likely presence of multigland disease—and therefore the need for bilateral parathyroid exploration—when only a mildly enlarged parathyroid is encountered first. Even when imaging studies suggest a single site of parathyroid disease and intraoperative PTH falls appropriately, a parathyroid gland that is 75 to 200 mg in size will rarely be a single adenoma (see Chapter 63, Intraoperative PTH Monitoring during Parathyroid Surgery). There is ongoing interest and some controversy in defining what truly constitutes an abnormal parathyroid and whether this is a matter of purely morphologic form, biochemical function, or a combination of both features (see Chapter 58, Principles in Surgical Management of Primary Hyperparathyroidism).
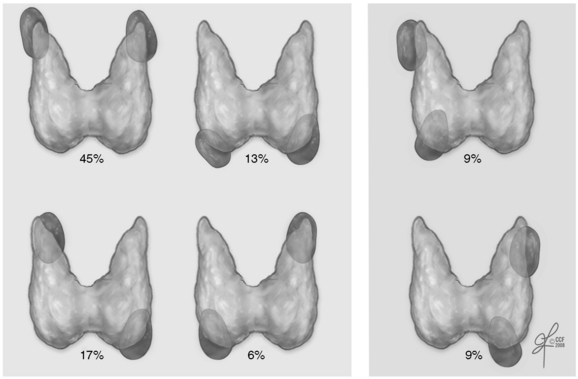
Embryologically, the upper parathyroids develop from the fourth branchial pouch and migrate caudally with the thyroid, whereas the lower parathyroid glands derive from the third branchial pouch and migrate with the thymus. The upper parathyroid glands have a narrower area of distribution and are fairly reliably positioned in the perithyroidal fat posterior to the superior pole of the thyroid gland and near the path of the recurrent laryngeal nerve as it enters the cricothyroid muscle (see Figure 59-2). In contrast, the lower parathyroids are more widespread around the lower pole of the thyroid gland, thyrothymic ligament, and pretracheal fat. Symmetry is usually present between parathyroid locations in the left and right sides of the neck, and this can strategically be used when trying to locate parathyroid glands. Double parathyroid adenomas, however, do not have a uniform or random distribution pattern: when only two glands are enlarged and histologically hypercellular, they tend to be upper parathyroids, a pattern designated as “fourth pouch disease.”7 This will occur in 45% of double adenomas, rather than the 17% expected if all six double adenoma locations occurred equally frequently. With other gland combinations, moreover, bilateral distribution is present in 82% (Figure 59-4).
Migratory distribution of the parathyroids can lead to ectopic locations within the thymus, within the sheath encompassing the carotid artery, jugular vein, and vagus nerve even in high cervical locations, retroesophageally and even intrathyroidally. Some but not all of these areas can be accessed via the usual cervical incision during bilateral parathyroid exploration. Recently, Perrier et al. proposed novel nomenclature to further classify cervical parathyroid adenomas into regions relevant for parathyroid exploration (see Chapter 60, Minimally Invasive Single Gland Parathyroid Exploration).8 Ectopic parathyroid locations in the anterior mediastinum, other deeper regions of the mediastinum, and even pericardium require alternate surgical approaches often in collaboration with thoracic surgeons.
The Rationale for Bilateral Parathyroid Exploration
Diagnosis
Bilateral parathyroid exploration principally involves patients with PHPT, although it is also needed in those who have secondary or tertiary hyperparathyroidism from renal disease. The latter diagnoses are covered in detail in separate chapters (see Chapters 65, Surgical Management of Multiglandular Parathyroid Disease, 66, Surgical Management of Secondary and Tertiary Hyperparathyroidism, and 67, Parathyroid Management in the MEN Syndromes). Traditionally, the diagnosis of PHPT has rested on the demonstration of simultaneously elevated serum total or ionized calcium with elevated intact PTH, in the setting of normal or high calcium excretion in the urine. With this combination of findings, the diagnosis of PHPT is practically definitive. In part, this is because modern measurements of PTH detect the intact molecule, reflecting the entire protein derived from the parathyroid glands and essentially eliminating confounding diagnoses from ectopic sources of PTH, such as tumors producing PTH related peptide (PTHrp). The rare hereditary condition of benign familial hypercalcemic hypocalciuria (BFHH) is excluded by the finding of normal or high levels of calcium in a 24-hour urine collection.
Approximately 10% of patients will have unusual biochemical presentations that do not fit these classical diagnostic criteria but are nonetheless found to have PHPT. There are at least two atypical versions of the disease. Normocalcemic PHPT manifests with normal total serum calcium but high PTH and has been relatively well appreciated; despite borderline laboratory values, these patients suffer from kidney stones, osteoporosis, and bone fractures.9 Patients with the other form of PHPT have high calcium levels but normal PTH. Diagnosis is somewhat easier if PTH values are “inappropriately” high-normal for the degree of hypercalcemia (40 to 60 pg/mL on a scale where 60 pg/mL is maximal reference range) but can be challenging when values are as low as 5 to 15 pg/mL. This atypical version has not been well characterized.
Table 59-1 provides a recommended diagnostic workup for PHPT and strategies to clarify the diagnosis in challenging scenarios. It is advisable to obtain a baseline bone density assessment with DEXA bone scan, especially if this did not precede referral of the patient to the surgeon. Urinary calcium excretion lower than 50 mg/dL should prompt consideration of explanations that include BFHH, renal disease, and the use of thiazide diuretics, among others.
Table 59-1 Diagnostic Workup for Primary Hyperparathyroidism
A detail-oriented and meticulous determination of clinical history is essential to enhance recognition of those patients who will be better served with a bilateral exploration. Some investigators have even proposed a scoring system to aid this process, particularly for identifying MEN kindred.10 Furthermore, when faced with the challenge of finding a missing parathyroid, confidence in the diagnosis and reasons for surgery is essential; otherwise, the surgeon may falter in the necessary steps to persist in the logical (and often lengthy) navigation through such surgery.
Treatment
Parathyroidectomy has the following operative goals: (1) achieving normocalcemic state and normal long-term PTH, (2) avoiding injury to the laryngeal nerves, (3) engendering minimal postoperative morbidity and negligible mortality, and (4) accomplishing cosmetic scar appearance acceptable to the patient. Surgery remains the most clearly demonstrated mechanism for durable cure of PHPT and symptomatic improvement, particularly related to osteoporosis and bone fractures, and neurocognitive issues.1 All of the surgical techniques that have evolved since the early 2000s share these goals: focal and unilateral exploration with or without intraoperative PTH measurement, radioguided parathyroid surgery, and videoscopic and robotically assisted parathyroidectomy.11 It is again important to stress that standard, bilateral parathyroid exploration meets these goals as well, although recent literature has questioned comparative performance with respect to morbidity and cosmetic outcomes.3,12–14 Especially when performed by experienced surgeons, bilateral parathyroid exploration has an excellent long-term track record of curing PHPT and can be achieved with minimal morbidity.15,16
Rationale for Parathyroid Surgery and Bilateral Exploration
A joint statement in 2005 by national professional associations of endocrine surgeons and endocrinologists stated that operative management is clearly indicated for all patients with classic symptoms or complications of PHPT.1 More challenging has been the perspective of decision making for those with apparently asymptomatic PHPT. Experts organized by the National Institutes of Health in 2002 proposed parathyroidectomy for the following patients: (1) those < 50 years of age, (2) those who cannot participate in appropriate follow-up, (3) those with a serum calcium level > 1.0 mg/dL above the normal range, (4) those with urinary calcium > 400 mg/24 hour, (5) those with a 30% decrease in renal function, or (6) those with systemic complications of PHPT including nephrocalcinosis, osteoporosis (T-score lower than − 2.5 SD at the lumbar spine, hip or wrist), or a severe psychoneurologic disorder.
It is difficult to predict reliably the development, timing, and progression of disease in patients with asymptomatic hyperparathyroidism. Long-term nonoperative management can be costly. For these reasons, other experts have advised a more liberal approach to recommendations of parathyroidectomy beyond the criteria identified by the National Institutes of Health (NIH), provided that surgery can be performed safely and with minimal risks for a disease that, in some patients, may be minimally problematic at the time of presentation. Thus, for example, parathyroidectomy may be appropriate to consider for patients with osteopenia (T-scores −1 to −2.5 SD) and mild neurocognitive symptoms.17,18
The indications for bilateral parathyroid exploration as the initial surgery for PHPT, once a patient has met the criteria indicated previously, are listed in Table 59-2. The guiding principle of bilateral parathyroid exploration is that some patients have significantly higher risk for multigland parathyroid disease, such that successfully achieving the operative goal of normocalcemia is contingent on the evaluation of all parathyroid glands in their usual anatomic locations and the appropriate resection of those that appear abnormal.
Table 59-2 Indications for Bilateral Parathyroid Exploration as the Initial Surgery for Parathyroid Disease



