Chapter 25 Sporadic Medullary Thyroid Microcarcinoma
Introduction
Thorough experience has been gained from biochemical screening programs for the early diagnosis of C-cell disease in families with hereditary medullary thyroid cancer (MTC).1,2 Based on such research, several study groups outside North America have considered routine calcitonin (CT) measurements (CT screening) worthwhile in patients with nodular thyroid disease with the objective of diagnosing sporadic MTC in an early and therefore potentially curable stage (see Chapters 23, Sporadic Medullary Thyroid Carcinoma, and 24, Syndromic Medullary Thyroid Carcinoma: MEN 2A and MEN 2B).3–14
Discussions have been intensive as to the advantages and disadvantages associated with thyroid nodular CT screening.15–19 Statements concerning CT screening have recently been incorporated in the collaborative guidelines published by the American Association of Clinical Endocrinologists (AACE) and the European Thyroid Association (ETA), which cover diagnostic and therapeutic aspects of thyroid nodular disease.20 Based on the decision model and the calculations by Shine21 and by Cheung et al.,22 together with the preliminary evaluations of prospectively applied CT screening protocols,3–14 it was concluded that the “measurement of basal serum CT level may be a useful test in the initial evaluation of thyroid nodules.” Measurement of nonstimulated serum CT level may therefore be considered before thyroid surgery for nodular goiter. If CT level is increased, the test should be repeated and, if confirmed, a pentagastrin- or calcium-stimulation test can be performed to increase diagnostic accuracy (it is of note that such stimulation tests are not available in the United States).20
As expected, such basal CT screening in patients with nodular thyroid disease resulted in many patients being identified as “at risk” for one of the various types of C-cell hyperplasia (CCH) or MTC. Subsequent stimulated CT levels when elevated have been found to be highly predictive of MTC or with one of the various types of CCH.23,24 There were no false-positive tests regarding these two entities (CCH and MTC) when applying defined cutoff levels for basal CT and stimulated CT and when applying a strictly individualized combined interpretation of both basal and stimulated CT levels.23,24 With an elevated stimulated CT level > 100 pg/ml, the finding of MTC is assured.25
Although clinically palpable sporadic MTC with cervical lymph node (LN) metastases prevail in larger single-center clinical MTC series,26,27 small and most frequently clinically “silent,” medullary thyroid microcarcinomas (microMTC) dominate in CT screening programs.3–14
Definition and Clinical and Biochemical Characteristics of Medullary Thyroid Microcarcinoma and C-Cell Hyperplasia
Definition
MTC refers to malignant tumors of the thyroid gland showing C-cell differentiation. The tumor cells are immunoreactive for CT in the majority of such cases. Tumor cells are typically positive for a variety of neuroendocrine markers such as chromogranin A and synaptophysin. Carcinoembryonic antigen is expressed in most cases (see Chapters 23, Sporadic Medullary Thyroid Carcinoma, and 24, Syndromic Medullary Thyroid Carcinoma: MEN 2A and MEN 2B). If the largest tumor diameter measures ≤ 10 mm and the lesion is limited to the thyroid gland, the lesion is called microMTC.28,29
Frequency and Prevalence
Reviewing autopsy studies, the frequency of microMTC accounts for 0.04% to 0.80%.30,31 The current prevalence of MTC ranges from 0.4% to 1.4% in “CT screening programs.”3–6,8–12,14 In the French nationwide database (1971 to 1996), sporadic microMTC represented 3.6% of all sporadic MTCs before 1984, 14.3% from 1984 to 1989, and, as a consequence of more systematic screening, 22% from 1990 to 1996.30
The majority of microMTCs are nonpalpable. Ultrasonography of the neck, which should be applied routinely in all patients with presumed C-cell disease, may detect solitary or multiple nodules of various sizes, but microMTC is suspected infrequently, especially in nodular thyroid goiter.32 Reporting the clinical characteristics of 80 patients with microMTC,30 the lesions were suspected because of elevated CT (47.5%), identified as pathologic findings at surgery (36.2%), clinically palpable lymph nodes (10%), or distant metastases (6.3%). Other investigators also described clinically suspected enlarged LNs in the lateral neck or distant metastasis on various sites in association with microMTC.31–35 Diarrhea or flushing may be observed in patients with nonpalpable thyroid tumor yet clinically identified lymph node.30,31
Morphologic Characteristics
C-Cell Hyperplasia (CCH)
The meticulous histologic examination of the thyroid glands removed during “CT screening programs” may reveal C-cell hyperplasia (CCH) with or without microMTC.24,36 There are several divergent definitions of CCH (see Chapter 44, Surgical Pathology of the Thyroid Gland).37 A rigorous classification is proposed, defining CCH by a quantity of C cells of > 50 cells per low-power field within both thyroid lobes in immunohistologic examinations.38 Different types of CCH (focal, diffuse, nodular, or neoplastic) according to proposed morphologic criteria38–41 may be documented in thyroids removed. The term CCH refers to the (reactive) “physiologic” and “neoplastic” variants. Different neoplastic potential is described for these two pathologic conditions.41–43 “Neoplastic” CCH (so-called C-cell carcinoma in situ) is generally accepted as being the precursor lesion of hereditary MTC, associated with germline mutations in the RET proto-oncogene. As shown recently,24 “neoplastic” CCH was documented in virtually every patient with hereditary MTC. The malignant potential of (reactive) “secondary” or “physiologic” CCH has not been fully demonstrated, and its clinical relevance in the development of sporadic medullary thyroid cancer thus remains unclear.36,40,43 Differentiating between “neoplastic C-CCH” and microinvasive MTC may prove very difficult in individual cases. “Neoplastic” CCH is characterized morphologically by groups of intrafollicular atypical C cells with partial or complete obliteration of the follicular spaces.43 There is a progressive increase in the proliferation index accompanied by an increase in molecular alterations and monoclonality, leading to invasive MTC.44 The presence of fibrosis around tumor cell nests and the demonstration of defects in the follicular basement membrane by immunohistochemistry or electron microscopy may definitively serve to discriminate between both entities.45
Medullary Thyroid Microcarcinoma
Location and Focality
Although multifocal and bilateral tumors are documented mainly in patients with hereditary disease, these tumor variants are also described in about 20% of patients with sporadic disease (18.5%,33 25.6%31).
In a study on sporadic microMTCs,32 histologic examination revealed unifocal tumors in 68 (77.3%) and bilateral, multifocal tumors in 29 (22.7%) patients, all with sporadic MTC. Tumor mean diameter was 4.2 ± 2.6 mm (range: 0.32 to 10 mm).
By definition (International Union against Cancer [UICC]), unifocal microMTC is classified as pT1a (UICC 1997, UICC 2009) or multifocal lesions in one or both lobes as pT1b (UICC 1997) or pT1am (UICC 2009).46 The UICC staging definitions based on the TNM criteria published in 200946 describe UICC stage I as pT1a(m)N0, M0, stage III pT1a(m) N1a (metastasis to prelaryngeal, pretracheal, paratracheal lymph nodes) M0; stage IVa as pT1a(m) N1b (metastasis to unilateral, bilateral or contralateral lateral cervical or superior mediastinal lymph nodes), and stage IVb as pT1a(m) N1a or N1b M1.
LN Compartments and LN Metastasis
Dralle47 proposed a simple LN classification, which is more meaningful when applied to MTC as opposed to the classic Robbins’ level classification.47 The “compartmental hierarchy” concept facilitates a better understanding of the disease and its potential for spread. His “compartmental classification” consists of cervicocentral (C1; right: C1a; left: C1b), right cervicolateral (C2), left cervicolateral (C3) and mediastinal (C4; right C4a; left C4b) compartments.
Central (C1) Dissection
LN metastasis occurs very early in the course of MTC, independent of the size, number, and location of the tumors.35 Among patients with microMTC who had lymph node dissection at surgery (68.8%), lymph node involvement with tumor was observed in 30.9% and was significantly more frequent in multifocal than in unifocal sporadic microMTC.30 However, Hamy and coworkers33 examined 601 LN from 41 patients with sporadic microMTCs and no involvement was documented. They concluded that systematic C1 dissection is of questionable value as lymph node involvement is uncommon in sporadic microMTCs.
Pillarisetty et al.48 retrospectively analyzed 18 patients, 4 (22.2%) of whom presented with LN metastasis. Subdividing the tumors in lesions ≤ 5 mm (9 patients; all diagnosed incidentally) and > 5 mm (9 patients, all with suspected MTC preoperatively), 4 of 6 patients with lesions > 5 mm with lymph node dissection had LN metastasis. Follow-up documented biochemical persistence in four patients in this group.
Lateral (C2/C3) Dissection
Scollo35 reported LN metastasis in 8 (67%) of 12 patients with microMTC. LN metastases were found in the central (C1) and lateral ipsilateral and contralateral neck (C2/C3), with varied frequency.35 In turn, Dralle47 described LN metastasis in 5 (14%) of 35 microMTCs, all localized exclusively in central or in the ipsilateral lateral compartments. Therefore, the authors recommend central (C1) neck dissection and ipsilateral lateral neck dissection.47 In other studies, LN metastases were documented in 11 (11.3% overall) of 97 patients affecting the central (2 patients), central and ipsilateral (5 patients), or contralateral neck (5 patients), respectively.32,49 In accordance with Scollo et al.,35 Scheuba et al.32 recommended C2 and C3 dissections in sporadic mircoMTCs depending on the CT levels and tumor characteristics (discussed later).
Mediastinal (C4) Dissection
With regard to microMTC, Machens et al.50 did not document LN metastases in the mediastinal compartment (C4), and so during initial surgery dissection of compartment C4 is thus not recommended. However, mediastinal LNs may be involved in individual patients with microMTC.32
Desmoplastic Stromal Reaction as an Intraoperative “Marker” for LN Metastases
About one third of all intrathyroidal MTCs fail to develop a “desmoplastic stromal reaction (DSR).”51–53 DSR is defined as the presence of a newly formed fibrotic (collagenous) stroma surrounding the invasive epithelial tumor cells, which is not found in the non-neoplastic thyroid parenchyma. DSR can be documented in (hematoxylin and eosin [H&E]) frozen sections.39,51 “DSR-negative” MTCs do not develop LN metastasis. The sensitivity and specificity for the parameter “DSR” to differentiate between N0 and N1 were 100% and 36%, respectively. A negative “desmoplastic stromal reaction” was shown to be an excellent intraoperative marker to exclude LN involvement.51 Initial bilateral lateral (C2, C3) neck dissection can therefore be avoided in all “DSR-negative” tumors. Meticulous (functional) bilateral lateral neck dissection is strongly recommended in “DSR-positive” patients.
Biochemical Characteristics and Correlation to Morphology
CCH or MicroMTC
In the majority of studies, a pentagastrin-stimulated CT value above 100 pg/mL was considered to be strongly related to MTC.8,25 However, there is an overlap of thyroid C-cell pathology for MTC, microMTC, and C-cell hyperplasia. To avoid “unnecessary” surgical procedures, Iacobone et al.54 proposed new cutoff values for basal CT of > 30 pg/mL and for stimulated CT of > 200 pg/mL. The positive predictive value of the test, to detect MTC, was 100% and the negative predictive value was 63%. Therefore, French study group recommends surgery in the presence of these cutoff values.54,55
Based on a small number of patients, Milone56 suggested a CT cutoff after pentagastrin stimulation of 275 ng/L to better distinguish CCH from MTC presurgery, thus being more helpful in selecting patients for thyroid surgery.
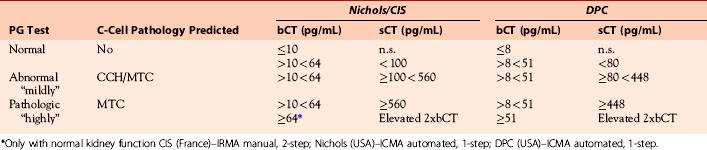
According to Scheuba et al.,24,32 patients with microMTC may be classified as those with “mildly” elevated CT levels and those with “highly” elevated CT levels (definition see Table 25-1). Patients with “mildly” elevated CT levels may show the various types of CCH (79.8%) or microMTCs (20.2%). No absolute threshold value was shown for basal or stimulated CT levels, which are able to reliably differentiate nonmalignant conditions (normal or CCH) from microMTC.23,54,56 In patients with “highly” elevated CT, microMTC was documented in 100%. The recommended biochemical criteria were helpful in predicting malignant C-cell disease in 153 (96.2%) of 159 patients.32 Increasing stimulated CT levels (steps of 200 pg/mL) demonstrated a highly significant linear trend in the increase of patients with MTC and a decrease of patients with CCH (p < 0.0001).24 Overall, more females than males had had MTC (p < 0.0124). In two subgroups with stimulated CT levels between 100 and 200 pg/mL and 201 and 400 pg/mL, respectively, MTC was documented significantly more frequently in females than in males.24 Guyetant et al.57 and Cherenkeo58 calculated a threefold higher prevalence of microMTC in women in the group of patients with basal and stimulated CT levels not exceeding 30 and 200 pg/mL. As a consequence, the indication for (total) thyroidectomy should be more liberal in females than in males.24
Table 25-1 Interpretation of the Pentagastrin (PG) Test and Prediction of C-Cell Pathology: Grouping of Patients Dependent on Basal (b) and Simulated (s) Calcitonin (CT) Levels; Ranges Dependent on Different CT Assays71,72
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


