Some Thoughts on the Orbicularis Oculi
HOW TO APPROACH THE MEDIAL ORBITAL WALL FOR FRACTURE OR DECOMPRESSION
1 The lower orbicularis oculi muscle is attached to the orbital rim medially (˜50%), and laterally to the suborbicularis oculi fat (SOOF) and rim by orbital retaining ligaments. Thus, ligamentous release and transection of the muscle along the rim will allow the skin, muscle, and underlying fascia to move upward as a unit.
2 The concept of high-sutured orbicularis oculi support to deep temporal fascia and/or periosteum alone, i.e., to hold up the lid or prevent ectropion, may deny the fact that the lid margin itself offers very little support. Thus, e.g., for festoons or full-cheek elevation, separate points of attachment along the lower rim and malar bone may also be crucial, not just at the new lid level or higher.
3 Motor innervation to the lower lid enters obliquely from the lateral off the temporal branch of VII, but primarily from below off the zygomatic branches of cranial nerve VII. Thus, the concept of a skin/muscle flap to leave innervated muscle is true, but it alone cannot support the entire lid and cheek.
4 The skin of the lid is very thin and the muscle of the lid is very vascular, with tremendous numbers of anastomoses. Thus, not only will full-thickness grafts of lid skin survive, but grafts of lid and muscle will also. This vascularity will also allow long, thin myocutaneous flaps to be transposed with success.
5 Surgeons have little problem approaching the orbital bones by many routes or the lateral wall, e.g., by orbitotomy or from above. Even the roof can be exposed, when required, by craniotomy or via a trans-lid approach. The medial orbital has not received enough “exposure,” so the canalicular/fornix approach is presented. Note that the medial orbit can also be approached via a vertically oriented W in the medial upper lid, and otolaryngologists often utilize endoscopy for transsinus placement of support for the lamina papyracea.
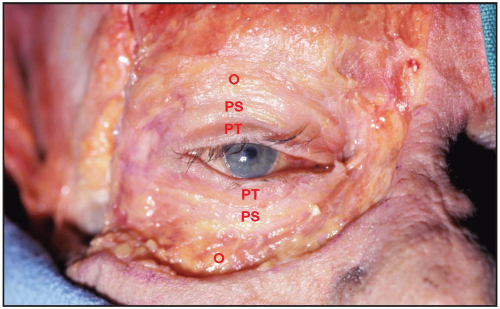 Figure 7D.1 The periorbital skin has been removed, exposing the orbicularis oculi muscle. This muscle acts as an antagonist to the levator palpebrae superioris muscle innervated by the third cranial nerve. The orbicularis oculi muscle is divided into palpebral and orbital portions. The palpebral portion is further subdivided into pretarsal (PT) and preseptal (PS) portions. The orbital portion (O) of the orbicularis oculi arises medially from the superomedial orbital margin, the maxillary process of the frontal bone, the medial canthal tendon, the frontal process of the maxilla, and the inferomedial orbital margin. The peripheral fibers sweep across the eyelid over the orbital margin in a series of concentric loops, the more central ones forming almost complete rings. In the upper lid, the orbital portion spreads upward onto the forehead, covers the corrugator supercilii muscle, and continues laterally over the anterior temporalis fascia. In the lower lid, the orbital portion covers the origins of the elevator muscles of the upper lip and nasal ala and continues temporally to cover part of the origin of the masseter muscle. Occasionally, the lower orbital portion interspersed with fat may actually continue downward into the cheek. The preseptal portion diverges from its origin on the medial canthal tendon and lacrimal diaphragm and passes across the lid as a series of half ellipses to meet at the later canthal raphe. The muscle bundles are not interrupted and do not interdigitate at the raphe. Medially, the orbicularis oculi unites to join the medial canthal tendon, which inserts on the medial orbital margin and nasal bones.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|