Nerve Blocks 101
In a 1998 article titled “How to Block and Tackle the Face”1, I presented a system for facile nerve blocks that would allow the surgeon to be more effective and efficient with local anesthesia once the block methods were adopted. I did not show the intraoral injections (e.g., inferior alveolar nerve or the long buccal nerve course) that I use, since most nondental surgeons shy away from them. In a like manner, I avoided intraorbital blocks used by ophthalmologists. In this chapter, I have made some additions, namely, for the lacrimal nerve (which I originally omitted) and for the cervical plexus, which will extend the surgeon’s range to the neck. Furthermore, as I am not constrained by journal limitations, the exposition is much grander in photographs and schematics and, thus, easier to understand.
My fervent hope for all who read this chapter is that you immediately start to practice these blocks. Once you become proficient, you will never again directly inject the nasal tip or lip without blocking first because you will know how much it will hurt. You will block the lips in preparation for marking the white roll with needles dipped in ink. You will start performing cases with blocks and simple oral premedications and marvel at your own skills.
 Figure 8.1 The infraorbital nerve opens downward and medially above 5-8 mm below the rim. In some cases the lower rim may have a ridge (arrows) which may be mistaken for fracture. |
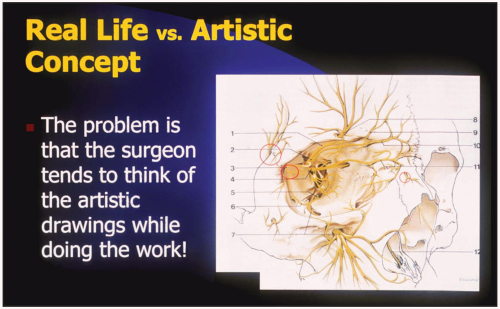 Figure 8.2 My original article1 explained block techniques to anesthetize the entire face. Some things were left out, but the overall explanation found there makes solid reading. As anatomy is taught less and less, we have learned to rely on illustrators’ drawings. If they are wrong, how can we think correctly in the operating room? The red circled areas in this drawing by a first class artist shows nerves going in incorrect directions and in incorrect positions. |
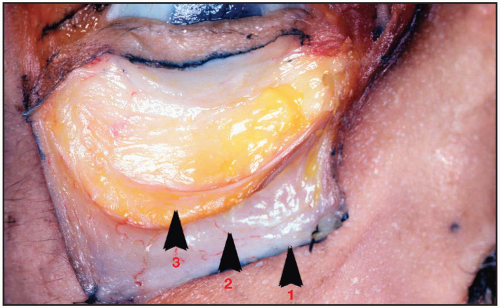 Figure 8.3 Where is the infraorbital nerve on straight gaze? Under 1, 2, or 3? Most people choose no. 2, but the answer is no. 1, on a line dropped from the medial limbus. The distance from the rim to the foramen is slightly greater for men, but 5.5 to 7.5 ±½ mm is the range. |
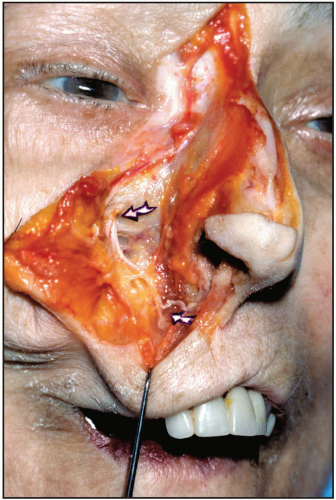 Figure 8.4 • The upper arrow shows the infraorbital exit. • The lower arrow shows a distal branch that rides over the levator to the upper lip to supply the base of the columella. |
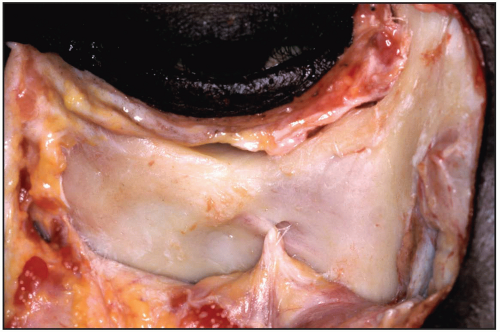 Figure 8.5 The foramen opens downward and medially, so injections to it should come from below and medial. |
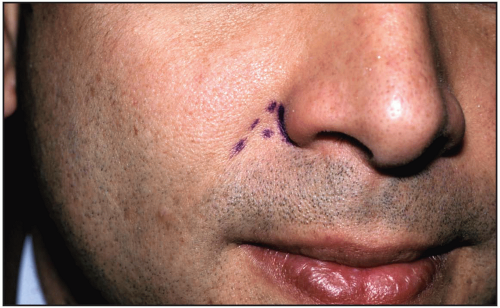 Figure 8.6 The dot between the nasolabial fold and alar base is the best entrance point. |
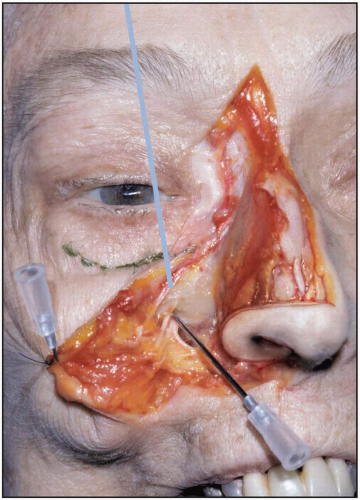 Figure 8.7 The rim is marked in green. The foramen is 5 to 8 mm down on a line from the medial limbus. |
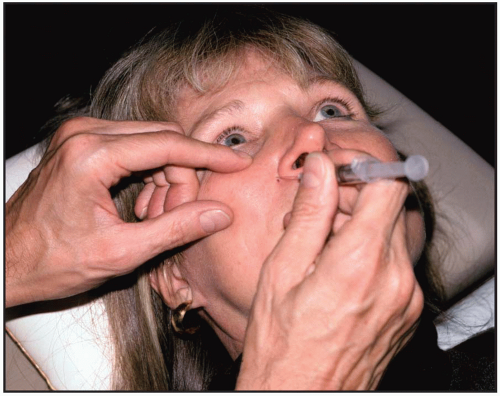 Figure 8.8 With a finger on the rim, the patient looks forward. The needle is held with a pen grip, and the surgeon inserts the needle to the foramen. With little practice, the surgeon can get into the foramen 90% of the time, and that number increases. Tell the patient he or she may feel an electric shock; that’s good a sign. At that point, you should inject because your position is correct. You will never get a neuritis. |
 Figure 8.9 This zone is the usual area of numbness for this block. Often, though, the numbness encroaches more on the lip or sidewall of the nose. In addition the lateral red border may often cover a larger area. |
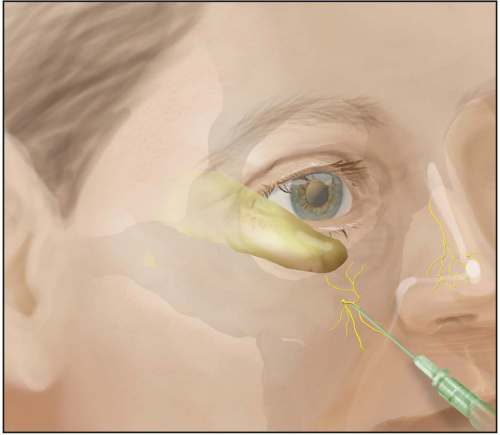 Figure 8.10 If the needle enters the foramen, the anterior superior alveolar nerve—which comes off between 5 and 20 mm prior to the foramen—may be blocked. In that case, the gingiva and front four teeth on that side will be affected. The anterior superior alveolar nerve travels through a small canal in the anterior maxilla (canalis spinosus) before supplying the teeth. Therefore, if the maxillary face is fractured, yet the lip has normal sensation and the gingiva is numb, the anterior face of the maxilla may be cracked. At times, a Caldwell-Luc opening to the maxillary sinus will desensitize the teeth and gingiva ipsilaterally due to disruption of the intrabony course of the anterior superior alveolar nerve. |
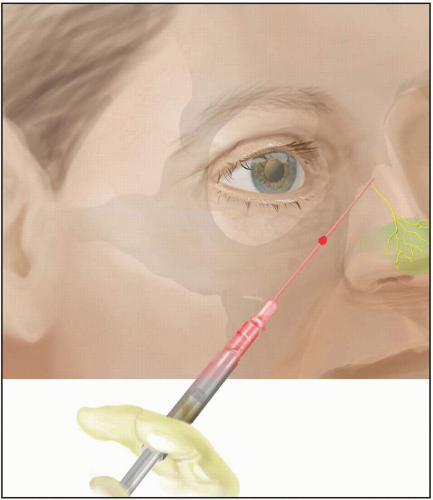 Figure 8.11 The dorsal nasal nerve, the dorsal branch(es) of the ethmoidal nerve, exits from under the nasal bone edge about 6 to 9 mm from the midline. There may be 1-3 branches although only one is shown. It passes under the nasalis muscle and provides sensation to the nasal tip. Once the infraorbital nerve is blocked, the dorsal nasal nerve can be blocked with a painless stick. The dorsal nasal nerve may have one to three branches to the tip region. Clinically, for a nasal tip lesion, the skin’s adherence to underlying cartilage makes direct injection painful. Blocking prior to tip injection is always a better option. |
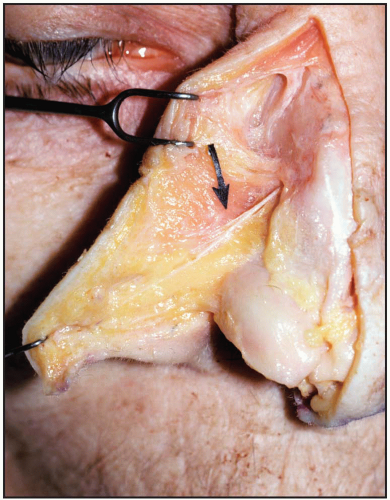 Figure 8.12 Transection of the nerve(s) is common via an intercartilaginous nasal incision, which explains tip numbness after some rhinoplasties. This block can be done from above or from the side, gliding along the deep distal bony edge toward or from the cheek after your infraorbital injection has been done. Where it comes out depends on nasal bone length to some degree. As it passes through a small groove at the edge of the nasal bones, it may remain single or split. The dorsal nasal nerve exits between 6.5 and 8.5 cm from the midline under the nasalis muscles (i.e., under the nasal SMAS layer). Anywhere from one to three branches may be found coursing almost straight along the midline toward the nasal tip. |
 Figure 8.13 Top: Dental professionals are taught early on the method of blocking the inferior alveolar nerve as it enters the lingula on the medial surface of the ramus. In addition, the long buccal nerve may be injected behind the third molar along the lower ramus, which will affect the cheek. Some physicians—e.g., some surgical dermatologists, plastic surgeons, and otolaryngologists—may feel better operating more toward the surface. The sensation of the entire lower lip from commissure to commissure depends on blocking the mental nerves. Usually three or four branches exit the mental foramen about the apex of the first or second bicuspids, but this varies. The 2-3 lip branches that block from the labiomental fold to vermilion can be effaced with the thumb for easy visualization. A third branch, and sometimes others through bone, supplies sensation to the chin pad; however, in many cases, a sensory branch off the mylohyoid nerve supplies a quarter-sized area of the chin pad on each side. Therefore, the pad will need additional supraperiosteal injection, as will be shown.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|