ROOF and Beyond (Superolateral Zone)
The “ROOF”—Retro-orbicularis oculi fat
1 Below the superolateral orbicularis oculi (preseptal and orbital part) and suborbicularis fascia, but above the orbital septum, the retro-orbicularis oculi fat (ROOF) pad extends from beyond the midsupraorbital rim to beyond the lateral orbital rim.
2 This fat pad contributes to fullness in the upper lid and may require removal or reduction, in addition to other measures, to reduce fullness in the lateral upper lid (e.g. lateral fat pad reduction and lacrimal gland prolapse treatment).
3 The heaviness in the lateral upper lid as noted may be caused by one or more of the following:
(a) The lateral subseptal fat pad, which can be treated by reduction similarly to other retroseptal fat.
(b) A low-hanging, obvious orbital lobe of the lacrimal gland, which can be treated by resection or recession by sutures, depending on preference or concerns.
(c) The ROOF, which lies over the superolateral bone and orbital septum across the upper lateral and middle lid region.
4 The ROOF can be safely reduced along the rim, although often a large vessel may require cautery. This vessel is anastomotic with the supraorbital vein medially, or if arterial with the supratrochliar.
5 Because the lacrimal nerve crosses the superolateral rim here, treatment of the ROOF may temporarily cause a small area of numbness in the lateral brow area.
6 The ROOF is part of the overall galeal fat pad, which extends upwards under the frontalis for 3 cm (±). This fat pad envelops the underside of the corrugator laterally, then continues medially to allow a corrugator gliding sleeve. It is often seen under the medial edge of the procerus muscles.
7 The galeal fat, of which the ROOF is one part, is responsible for the easy mobility of the lower 2 + cm of forehead. The mobile forehead actually exists as the muscles ride over and through the fat.
8 Because of this mobility, treatment of a droopy brow (as from facial paralysis) from above rarely works, as the glide planes are still active. Therefore, to stabilize the paralyzed brow exactly without movement or migration, the subgaleal fat needs removal so the brow can be fixed directly by anchors or another subperiosteal device.
9 Because the fat is a poor holder of sutures, elevation of the lateral brow by suturing to this fat rarely provides predictable long-term results.
10 Exposure of the ROOF, however, will provide access to the lateral corrugators where they insert into the underside of the frontalis muscles over a broad area. From here, corrugator resection medially may also proceed with ease.
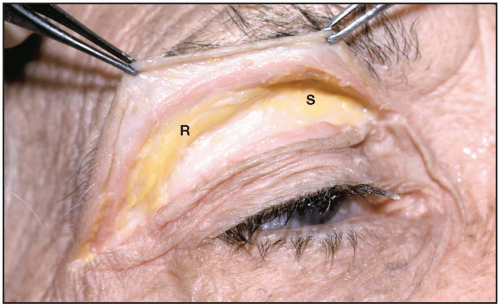 Figure 4.1
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|