Split-thickness skin grafting has been an important tool in the kit of otologic surgeons for over 100 years. These grafts can be placed primarily at the time of tympanoplasty or tympanomastoidectomy. Split-thickness skin grafts may also be placed secondarily to address post-surgical mastoid cavities or tympanic grafts presenting with myringitis. Although split-thickness skin grafting is not required for epithelialization to occur, it does appear to decrease the time required for complete healing.
48.2 Patient Selection
We use primary split-thickness skin grafts routinely, not only in tympanomastoidectomy surgery, but also in canalplasty and aural atresia repair. In cavities or grafts that remain poorly healing, we also perform secondary split-thickness skin grafting as needed to obtain a dry, safe ear.
48.3 Surgical Technique
48.3.1 Primary Grafts
Our current technique for primary split-thickness skin grafting at the Massachusetts Eye and Ear Infirmary has been passed down from Schuknecht to generations of trainees. The basic setup is shown in ▶ Fig. 48.1. After general anesthesia has been induced, the arm is prepped and mineral oil is applied to the donor site and the battery-powered dermatome. The graft is harvested from the medial aspect of the ipsilateral upper arm (▶ Fig. 48.2). Following harvest, the skin graft is laid flat, epithelial side down, onto OTOSILK graft dressing (Boston Medical Products, Inc., Westborough, Massachusetts) that has been lightly covered with bacitracin. The OTOSILK allows for easy manipulation of the grafts without sacrificing pliability.

Fig. 48.1 Basic materials for collecting a split-thickness skin graft. OTOSILK graft dressing is lightly coated with bacitracin. A battery-powered dermatome is used to collect the graft after applying mineral oil to the skin and the dermatome blade. Following graft harvest, the site is covered with a plastic adhesive dressing and a needle is used to fenestrate the adhesive to allow egress of blood. The arm is then wrapped with sterile gauze.
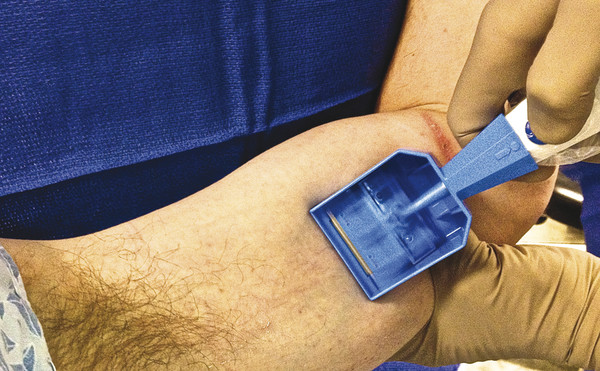
Fig. 48.2 The split-thickness skin graft is harvested from the inner aspect of the ipsilateral upper arm.
The grafts are then cut into smaller pieces, covered with moist gauze, and set aside for later use during surgery. We favor thin grafts given that they better conform to surfaces and appear to survive better over time. As shown in ▶ Fig. 48.3, a 5 cm x 4 cm graft is sufficient for a canal wall-down procedure. The donor site is then covered with a sterile adhesive dressing wrapped with sterile gauze.
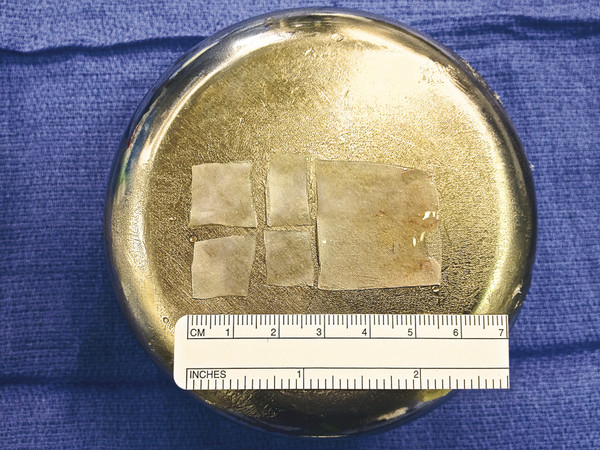
Fig. 48.3 The harvested split-thickness skin graft is laid epithelial side down onto the OTOSILK graft dressing, spread flat, and cut into smaller pieces. A graft of this size will comfortably line a canal wall-down cavity.
Once the tympanomastoid procedure is completed and the fascia and cartilage grafts have been placed (▶ Fig. 48.4), the trimmed skin grafts are brought into the field and placed over the exposed bone and fascia with the epithelial and OTOSILK sides facing up. It is our practice to rotate an inferiorly based periosteal flap over bone paté into a canal wall-down cavity for partial obliteration,1 and we also place skin grafts over areas of the flap that lie exposed within the cavity. We partially overlap the grafts at the edges (▶ Fig. 48.5). To hold the grafts in place, we apply multiple OTOSILK otologic strips soaked in cortisporin solution in a starburst pattern that covers all the grafts. Pieces of cotton soaked in cortisporin are then gently laid on top of the strips.2 The otologic strips are then folded back over the cotton to complete the “rosebud” dressing (▶ Fig. 48.6), and lateral strip gauze packing is placed.
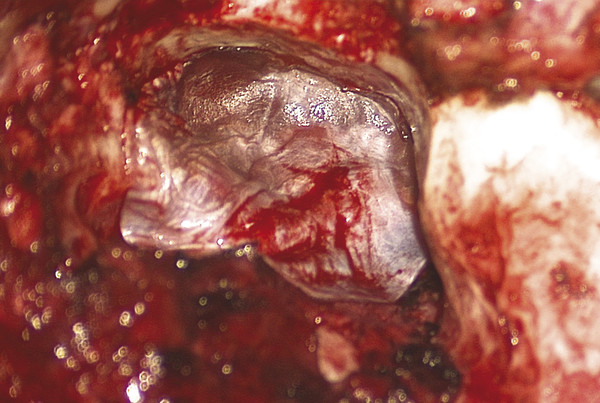
Fig. 48.4 The tympanomastoid cavity immediately prior to grafting. This is a canal wall-down procedure performed on a left ear, and the cartilage and fascia grafts have been placed. Note the inferiorly based periosteal flap that has been rotated forward to partially obliterate the cavity.
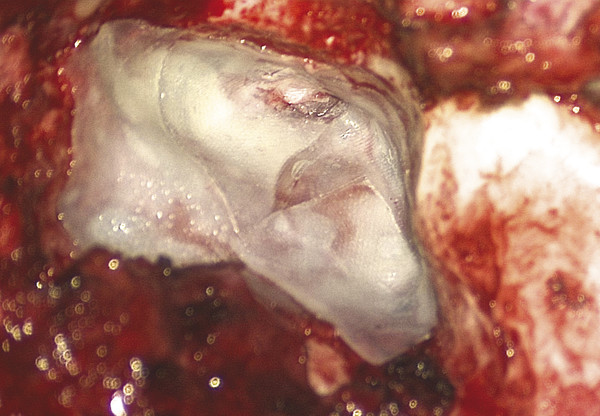
Fig. 48.5 Split-thickness skin grafts placed over the fascia graft, exposed bone within the cavity, and the exposed portion of the inferiorly based periosteal flap.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


