Skin and Lacrimal Drainage Systems
Brian C. Tse
Matthew W. Wilson
William R. Morris
SKIN: INTRODUCTION AND TERMINOLOGY
Dermatology and skin pathology (dermatopathology) have contributed to the significant advances in the understanding of immunologic and pathologic mechanisms of skin disease in the last 25 years. The histologic evaluation of biopsies from periorbital and lid skin has become more common for inflammatory conditions and for the rapidly increasing number of skin cancers, which are most commonly found on the central face.
Histologic findings in normal periorbital skin are similar to other areas of the body with a keratinizing epidermis and a prominence of sebaceous glands and blood vessels (Figs. 7.1A and B). Eyelid skin is very thin, as the epidermis is composed of only a few layers of keratinocytes (squamous cells). Of note, the typical rete ridge (digitated) pattern is absent, and the sparse dermis is composed of fine fibrillar collagen fibers. Virtually all inflammatory dermatoses and cutaneous neoplasms may affect the periorbital skin and eyelids, while others are specific to the region.
TERMINOLOGY
The following histologic terms are essential to a basic understanding of dermatopathology and are seen in a variety of conditions.
Hyperkeratosis is increased thickness of the stratum corneum, which is the most superficial, cornified layer of the epidermis. Orthokeratosis is hyperkeratosis composed of cells with complete keratinization and no remnants of nuclei. Parakeratosis is a manifestation of incomplete keratinization in which nuclei are retained within the cells of the stratum corneum. Generally, a thick granular layer is found beneath orthokeratosis due to slow upward migration of keratinocytes, while a thin or absent granular layer is seen beneath extensive parakeratosis due to increased cell turnover and migration. The changes in the superficial portions of the epidermis are a clue to epidermal pathologic processes. Leukoplakia (white plaque) is strictly a clinical term. Any lesion of a mucous membrane, including the conjunctiva, with hyperkeratosis will appear as leukoplakia. Hyperkeratosis may be induced by an underlying lesion, including pingueculum, pterygium, papilloma, or carcinoma in situ.
Hyperplasia is an increased number of cells in the epidermis, which results in overall architectural changes: projection above the skin surface, elongation of the rete ridges, and widening of the rete ridges. Acanthosis is defined more specifically as an increased thickness of the stratum spinosum (spinous or middle layer) of the epidermis.
Acantholysis is a loss of cohesion between epidermal cells (keratinocytes) that may be caused by a variety of pathologic processes which result in a degeneration of intercellular connections. This separation may lead to histologic clefts, tiny intraepidermal vesicles, or larger intraepidermal bullae. Acantholysis may occur secondary to spongiosis (intercellular edema), ballooning (intracellular edema), or a genetic or immunologic dissolution of anatomic attachments or intercellular ground substance.
Spongiosis is a histologic term that describes the fluid accumulation between epidermal cells that eventually leads to cleft or vesicle formation. It is most commonly seen in inflammatory conditions, especially in the spectrum of dermatitis. Ballooning or intracellular edema is a characteristic of virally infected cells that will eventually lead to cell lysis and formation of coalescent clefts or spaces.
It is important to make a distinction between atypical cells, dyskeratotic cells, and necrotic cells in the epidermis. In an atypical cell, the normal nuclear-to-cytoplasmic ratio is altered in favor of the nucleus (nuclear hyperplasia). The nucleus will stain darker than normal (hyperchromasia), while the nuclear configuration may be abnormal such as multinucleated, indented, or cerebriform. The cell may contain an abnormal mitotic figure. When individual nuclei are sufficiently atypical or large numbers of atypical cells are present, the lesion is usually malignant or cancerous. Atypical cells, however, such as those seen in lymphomatoid papulosis—a benign inflammatory condition—should not be regarded as the only criterion necessary for a diagnosis of malignancy. Architectural histologic features and clinical presentation must also be taken into consideration. Dyskeratosis refers to increased keratinization of individual epidermal cells that are characterized by abundant eosinophilic staining cytoplasm and small, normal-appearing nuclei. In contrast, necrotic keratinocytes have nuclear karyolysis and pyknosis with homogeneous pink cytoplasms.
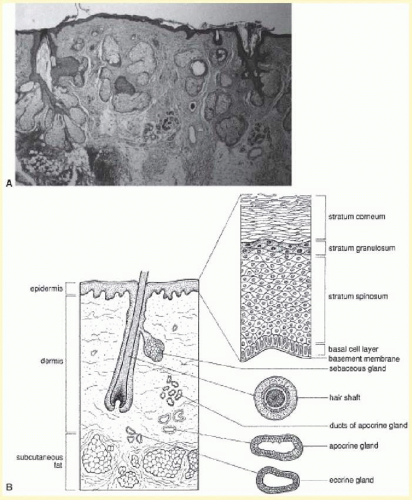 FIG. 7.1 A: Photomicrograph of normal periorbital skin. B: Schematic of normal periorbital skin. |
Vesicles or bullae are distinguished by size and refer to separations within the epidermis (intraepidermal vesicle or bulla) or beneath the epidermis (subepidermal bulla). Subepidermal bullae may occur within the dermal-epidermal junction zone or beneath this zone.
Atrophy refers to thinning of the epidermis, effacement of the rete ridges, disorder of epidermal architecture, diminution or loss of skin appendages, and alterations of the collagen and elastic fibers in the dermis. These changes are seen clinically as wrinkling and laxity of skin.
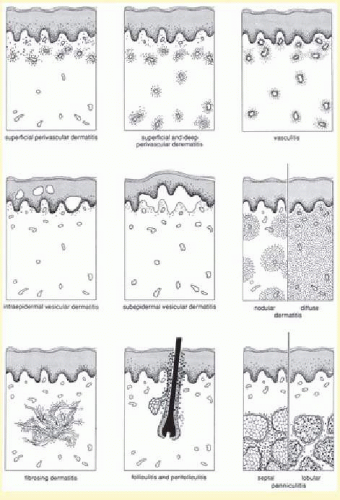 FIG. 7.2 Basic histologic patterns of inflammatory skin diseases. |
The study of dermatology and dermatopathology is made difficult by the large number of described conditions and diseases and is often hindered by obscure historic terminology. In 1978, Ackerman published a landmark textbook, Histologic Diagnosis of Inflammatory Skin Diseases, a Method by Pattern Analysis. He successfully presented a scheme to simplify the analysis of inflammatory skin diseases by describing nine basic histologic patterns with many subcategories (Fig. 7.2). This categorization has allowed skin pathologists to more precisely diagnose many inflammatory conditions and to provide the clinician with a more useful differential diagnosis when a specific diagnosis cannot be rendered.
INFLAMMATORY DERMATOSES
Dermatitis is inflammation of the skin and is often used synonymously with eczema. These terms can be combined to form eczematous dermatitis, which may encompass a broad spectrum of cutaneous disorders. Dermatitis of any nature is the most common pathology of periorbital and eyelid skin.
Clinical and histologic changes may be divided into acute, subacute, and chronic dermatitis, although lesions may appear or persist in any of the stages. The earliest clinical changes of acute dermatitis are erythema and edema, which may progress to vesiculation, oozing, and eventually crusting and scaling. There are often secondary changes due to scratching or infection. Chronic dermatitis is characterized by papules and plaques with indistinct borders, less intense erythema, increased skin markings (lichenification) with fine scale and firmness, or induration to palpation. Subacute dermatitis is vaguely intermediate between acute and chronic, with erythematous scaling papules, rare small vesicles, and slight clinical induration. End-stage chronic dermatitis is often referred to as lichen simplex chronicus and is most commonly seen in atopic dermatitis.
A thorough clinical history and examination with emphasis on the distribution and characteristics of lesions often allow for a more specific characterization of the dermatitis with a relationship to cause. The most common form of dermatitis around the eyes is irritant contact dermatitis, which is a non-immunologically mediated reaction of the skin caused by exposure to an inciting substance. All individuals will react if the concentration of an irritant substance is sufficiently high or the duration of contact is long enough. Mild irritant dermatitis is usually caused by soaps and detergents, while more acute and severe dermatitis may be related to more toxic acids, alkalies, and solvents. Allergic contact dermatitis is a type IV immunologic reaction requiring a primary exposure, sensitization, and re-exposure to an allergen with an immunologic delay before clinical expression of the dermatitis. A detailed history and subsequent patch testing may be necessary to identify a specific allergen. Atopic dermatitis is a chronic, severely pruritic dermatitis associated with a personal or family history of atopy (asthma, allergic rhinitis, atopic dermatitis). It is characterized by a typical morphology and distribution, a chronic relapse in course, and a variety of associated findings. Periorbital and eyelid skin involvement is common. Seborrheic dermatitis, dyshidrotic dermatitis of the hands and feet, stasis dermatitis of the lower extremities, and nonspecific neurodermatitis are other variants. Photodermatitis may be either irritant or allergic in etiology and requires a history of an association between the appearance of the dermatitis and sun exposure.
Blepharitis is simple, diffuse inflammation of the eyelids. Sebhorrheic blepharitis is a specific type of chronic blepharitis primarily involving the eyelid margins and is often associated with dandruff and greasy scaling of the scalp, eyebrows, central face, chest, and pubic areas. Hyperemic, inflamed eyelid margins and yellow, greasy scales on the lashes are characteristic identifiers.
All types of dermatitis are characterized histologically by spongiosis and a mild, superficial perivascular infiltrate (predominantly lymphohistiocytic, mononuclear cell) in the superficial dermis. Confluent spongiosis leads to intraepidermal vesiculation in acute dermatitis (Fig. 7.3A), while milder or focal spongiosis without vesiculation is seen in subacute variants (see Fig. 7.3B). Chronic dermatitis is characterized by a compact orthokeratosis (usually secondary to the patient rubbing), irregular epidermal hyperplasia, and scant to absent spongiosis. In the superficial dermis (papillary dermis), the collagen bundles are abnormally thickened and are oriented perpendicular to the plane of the epidermis (see Fig. 7.3C).
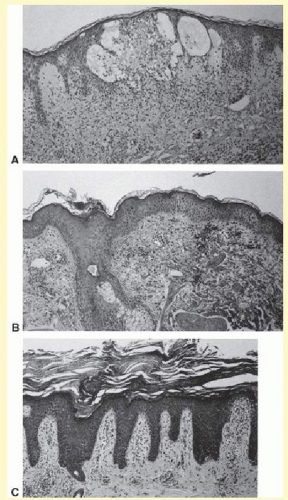 FIG. 7.3 A: Acute dermatitis with confluent intraepidermal spongiosis leading to vesicle formation. B: Subacute dermatitis with moderate intercellular edema (spongiosis). C: Chronic dermatitis with lichen simplex chronicus (compact orthokeratosis, irregular epidermal hyperplasia, and papillary dermal fibrosis). |
Urticaria is the widespread appearance of pruritic hives or erythematous, slightly indurated, non-scaling dermal papules or plaques. These may occur at any body site and usually are transient, with individual lesions lasting less than 24 hours; new lesions, however, may appear continuously or in bouts. When periorbital or lid skin is involved, there are coalescent, erythematous papules without surface scale or change. Biopsy shows a normal epidermis with edema of the superficial dermis and a scant perivascular lymphohistiocytic infiltrate. Eosinophils may be seen in urticaria of short duration, while neutrophils are present in conditions of a more chronic nature. Angioedema presents with deeper, more indurated swelling characterized by deep dermal and subcutaneous edema on biopsy. Urticaria and angioedema are often associated clinically and may be due to a multitude of etiologies. There is also a specific type of hereditary angioedema secondary to a low serum level of the inhibitor of the first component of complement.
CUTANEOUS INFECTIONS
Cellulitis is an infection involving the dermal and subcutaneous tissues around the eye, resulting in erythema, edema, tenderness, and warmth. Staphylococcal infections are the most common pathogens. Histologically, there is edema throughout the dermis with a sparse, widespread infiltration of neutrophils between collagen bundles. The epidermis appears normal.
An external hordeolum, or stye (Fig. 7.4), results from acute purulent inflammation of the superficial sweat and sebaceous glands or hair follicles of the eyelids, while an internal hordeolum occurs in the meibomian glands within the tarsal plates of the eyelids. Hordeolums are characterized histologically by dense inflammation containing neutrophils and foreign body multinucleated giant cells around intact or ruptured skin appendages. A chalazion is chronic inflammation of a sebaceous gland, either the meibomian glands (deep type) or glands of Zeis (superficial type), resulting in a firm, painless nodule of the eyelid (Fig. 7.5A). Histologically, there is deep dermal or subcutaneous suppurative granulomatous inflammation containing neutrophils, plasma cells, lymphocytes, histiocytes, and giant cells in a zonal configuration around central lipid material (see Fig. 7.5B).
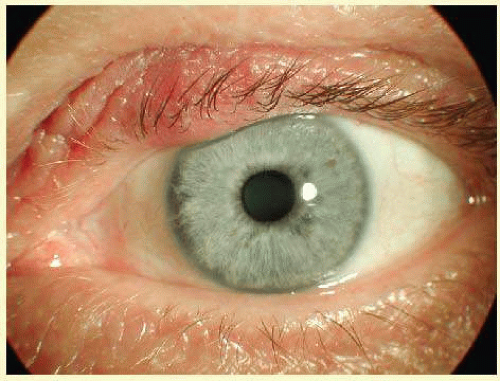 FIG. 7.4 Hordeolum—Clinical photograph of tender erythematous mass on the upper eyelid. (Photo courtesy of William Morris, MD.) |
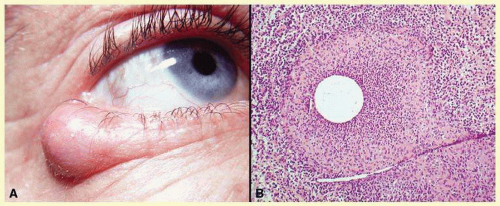 FIG. 7.5 Chalazion—A: Typical clinical appearance of chalazion. B: Lipogranulomatous reaction with epithelioid cells, lymphocytes, and plasma cells surrounding a central nidus of meibomian gland secretion. Clear area in center represents lipid material dissolved out during processing of tissue. Giant cells are sometimes seen (hematoxylin and eosin stain). (Photos courtesy of William Morris, MD.) |
Erysipelas is a specific type of acute cellulitis caused by group A hemolytic Streptococcus and characterized clinically by a sharply demarcated, warm, red, dermal, and subcutaneous plaque on the face.
Blepharoconjunctivitis is a specific type of chronic blepharitis that primarily involves the eyelid margins and, secondarily, the conjunctiva. Chronic sensitivity to staphylococcal infection is the proposed etiology. Histologic changes are those of a chronic dermatitis (epidermal hyperplasia, hyperkeratosis, and parakeratosis), along with dermal inflammation containing neutrophils similar to cellulitis.
VIRAL INFECTIONS
Umbilicated vesicles on an erythematous base progressing to pustules and crusted papules are characteristic of generalized vaccinia (small pox), with new cases recently reported secondary to the small pox vaccine. These vesicles are also characteristic of varicella (chickenpox), herpes zoster (shingles), and primary and recurrent herpes simplex infections (Fig. 7.6A). Herpesviruses are DNA-containing viruses that infect host cell nuclei and result in similar, characteristic histologic changes. There is marked intraepidermal vesiculation and necrosis with massive ballooning and rupture of keratinocytes, spongiosis, and acantholysis. A dense, superficial, dermal, perivascular lymphohistiocytic infiltrate with neutrophils is also commonly seen infiltrating the epidermis. Multinucleated epithelial giant cells with nuclei, which are steel gray and demonstrate peripheral margination of clumped chromatin material, are characteristic of early and well-developed vesicles (see Fig. 7.6B). Progression to near total epidermal necrosis makes these characteristic cells more difficult to identify. Occasionally, eosinophilic staining and small intranuclear inclusions may be visible. A Tzanck smear may be obtained by unroofing a vesicle, scraping the base, and staining the base with Giemsa stain. This rapid diagnostic method enables identification of multinucleated epithelial giant cells and single keratinocytes with characteristic nuclear changes. However, real-time PCR testing has allowed for earlier detection of DNA-containing viruses and has now become the diagnostic gold standard.
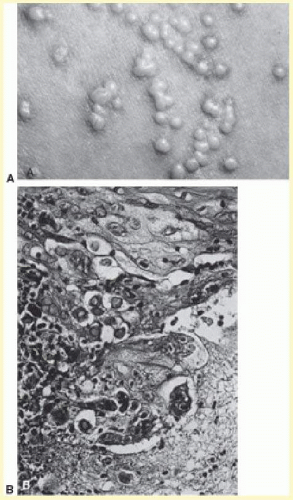 FIG. 7.6 A: Recurrent herpes simplex infection with umbilicated pustulovesicles on an erythematous base. B: Herpes simplex infection with intraepidermal vesicle containing characteristic multinucleated epithelial giant cells. |
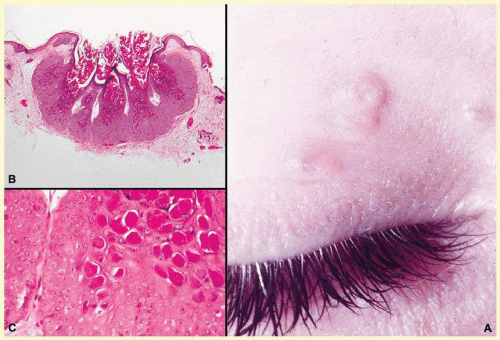 FIG. 7.7 Molluscum contagiosum—A: Umbilicated lesions typical of molluscum contagiosum on the upper lid of a child. Infection near the edge of the lid may cause a toxic follicular conjunctivitis. B: Low-power photomicrograph demonstrating crater shape of excised lesion (hematoxylin and eosin stain). C: High-power photomicrograph illustrating the large clumps of eosinophilic viral inclusions in the epithelial cells (“molluscum bodies”) (hematoxylin and eosin stain). (Photos courtesy of William Morris, MD.) |
Lesions of molluscum contagiosum often affect the periorbital and lid skin as 1- to 3-mm dome-shaped papules with a small central dell. This large pox virus multiplies in the cytoplasm, and homogeneous purple intracytoplasmic inclusion bodies (molluscum bodies) are seen in an acanthotic epidermis on histology (see Fig. 7.7).
Verruca vulgaris (warts) are caused by a variety of papilloma viruses and may present as small papules with a digitated surface or elongated filiform warts around the eyes. Histologically, they demonstrate varying degrees of massive papillomatosis, hyperkeratosis, and acanthosis with parakeratosis and collections of serum in the stratum corneum at the tips of the digitations (Fig. 7.8). In early warts, the keratinocytes in the granular layer and just beneath the granular layer are vacuolated with condensation and clumping of dark-staining keratohyaline granules and occasional eosinophilic inclusion bodies in the nuclei.
FUNGAL AND PARASITIC INFECTIONS
Dermatophytosis may affect periorbital and eyelid skin as typical circinate, scaling, erythematous plaques (ring worm) or may primarily infect the eyelashes, resulting in lash loss. Biopsy demonstrates a minimal superficial perivascular lymphohistiocytic infiltrate with overlying orthokeratosis and focal parakeratosis. On high-power examination, hyaline-segmented hyphae may be seen in the orthokeratotic areas of the stratum corneum with the help of histochemical stains such as periodic acid-Schiff stain (PAS) and Gomori methenamine silver (GMS). In candidiasis, pustules on an erythematous base are often present, and, there are septate pseudohyphae and small oval spores in the stratum corneum.
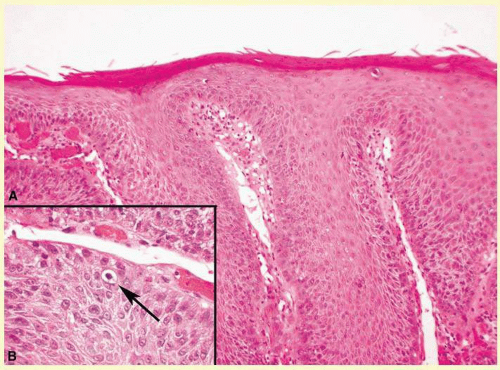 FIG. 7.8 Verruca vulgaris—A: Low-power photomicrograph illustrating papillomatous growth with a fibrovascular core, hyperkeratosis, and acanthosis (hematoxylin and eosin stain). B: High-power photomicrograph demonstrating intranuclear viral inclusion (black arrow) (hematoxylin and eosin stain). (Photos courtesy of William Morris, MD.) |
Pityrosporum orbiculare, in its yeast phase, is part of the normal flora of the central face, and small spores (3 µm) are often visible in the stratum corneum, especially in the superficial portions of hair follicles. Tinea versicolor is a more specific disease and presents as hyper- or hypopigmented, scaling patches on the face. Scrapings examined in potassium hydroxide (KOH) solution or a biopsy stained with PAS will demonstrate small hyphae and spores in clusters within the stratum corneum (often termed spaghetti and meatballs).
The parasitic mite Demodex folliculorum lives in hair follicles with large sebaceous glands, especially around the nose and eyes. Histologically, the mite is frequently seen as an incidental finding in a facial hair follicle with a minimal surrounding inflammatory infiltrate (Fig. 7.9). Many dermatologists believe that some cases of acne rosacea and folliculitis are caused by large numbers of Demodex, especially in immunosuppressed patients. In these instances, there is dense follicular and perifollicular inflammation.
BULLOUS DISEASES
Vesicles (small) and bullae (large) may occur within the epidermis at various levels of cleavage (intraepidermal vesicles) and beneath the epidermis (subepidermal vesicles). A separation plane may be seen beneath the electron microscopic basement membrane or, due to dissolution of various components, within the basement membrane itself. Lesions of pemphigus (intraepidermal), cicatricial pemphigoid (subepidermal), and the erythema multiforme-Stevens-Johnson complex (combined intraepidermal and subepidermal) may occur on the eyelids and on the conjunctiva.
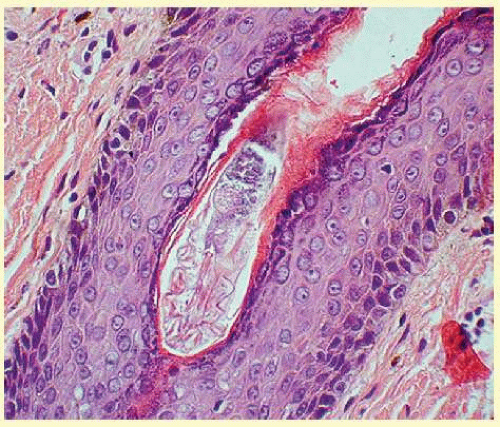 FIG. 7.9 Demodicosis—Demodex folliculorum residing in hair follicle (hematoxylin and eosin stain). (Photo courtesy of William Morris, MD.) |
Pemphigus represents a group of diseases that has circulating antibodies directed against intercellular substances or keratinocyte surface antigens. A cleavage plane in the granular layer is characteristic of superficial pemphigus; a supra-basilar or midepidermal plane is characteristic of the most severe form, pemphigus vulgaris. Clinically, superficial, flaccid blisters rapidly erode and spread easily when compressed. Histologically, the keratinocytes separate immediately above the basal layer, extending to the midepidermis (pemphigus vulgaris) without spongiosis. Individual keratinocytes appear rounded with prominent nuclei. No intercellular bridges are visualized, and there is no significant inflammation in an early lesion (Fig. 7.10). A direct immunofluorescent study (skin biopsy) and an indirect immunofluorescent study (serum) show intracellular deposition of immunoglobulin G (IgG) and complement proteins throughout the epidermis. Pemphigus vulgaris, often fatal before the advent of steroid and immunosuppressant treatment, still remains a very severe disease.
Bullous pemphigoid occurs mainly in older patients and is characterized by large, tense, firm bullae. Histologically, there is a discrete subepidermal separation with a prominence of eosinophils in the inflammatory infiltrate. Almost all patients have circulating IgG antibodies that deposit at the dermoepidermal junction in a linear fashion. Bullous pemphigoid rarely leaves significant scars. Cicatricial pemphigoid is a related subepidermal bullous disorder that mainly affects the mucosa of the conjunctiva and oropharynx. The lesions characteristically resolve with scarring, which may eventually lead to blindness. Histologically, the lesions are similar to bullous pemphigoid, but there are often more neutrophils in the infiltrate with extensive spongiosis in the epidermis. Again, IgG antibodies are directed against protein components of the basement membrane.
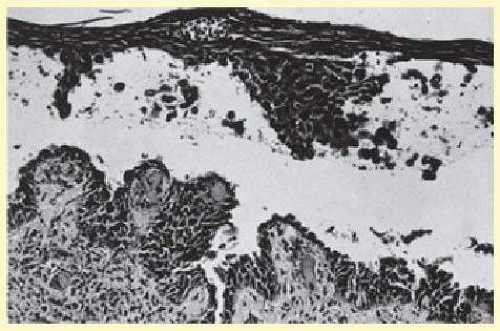 FIG. 7.10 Pemphigus vulgaris showing acantholytic keratinocytes in a suprabasalar vesicle. |
Erythema multiforme is a common pathway cutaneous reaction to drugs, viral or bacterial infections, or unknown causes. Characteristic “target” lesions are seen as round-to-oval erythematous plaques with central darkening and marginal erythema. In Stevens-Johnson syndrome—the most severe form—the mucocutaneous surfaces (including the conjunctiva) are predominantly affected in association with a systemic syndrome and may lead to death. Histologically, erythema multiforme and Stevens-Johnson syndrome are characterized by a dense lymphohistiocytic infiltrate that obscures the dermoepidermal junction associated with progressive necrosis of keratinocytes from the basilar to the uppermost portions of the epidermis. The intraepidermal and subepidermal vesiculation may lead to severe scarring of mucosal surfaces.
LID AND PERIORBITAL MANIFESTATIONS OF SYSTEMIC DISEASES
All of the connective tissue or collagen vascular diseases may affect the skin near the eyes. Lupus erythematosus (LE) is an extremely heterogeneous disease that includes a broad spectrum of clinical forms in which cutaneous disease may occur with or without systemic involvement. Scaling, erythematous papules and plaques with follicular plugs, hypopigmentation and hyperpigmentation, and discrete margins are characteristic of chronic cutaneous LE (discoid LE). Histologically, there is hyperkeratosis, follicular plugging, thinning of the epidermis, vacuolar alteration at the dermoepidermal junction (tiny, oval, clear spaces), a thickened light microscopic basement membrane, and a superficial and deep perivascular and periadnexal mononuclear inflammatory infiltrate in the dermis. Increased mucin often can be seen between collagen bundles in any of the collagen vascular diseases.
A common cutaneous manifestation of dermatomyositis is a violaceous heliotrope around the eyes, on the lids, and on the cheeks. Histologically, there is orthokeratosis, thinning of the epidermis, loss of the rete ridge pattern, and vacuolar alteration at the dermoepidermal junction with a mild lymphohistiocytic infiltrate in the dermis.
Scleroderma may occur in either a generalized systemic form or several localized cutaneous forms. The characteristic clinical lesion is a sclerotic plaque with an ivory center, which appears bound down when palpated. Histologically, the epidermis is atrophic with thickening of the entire reticular dermis extending into the subcutaneous fat and associated loss of adnexal structures. Individual collagen bundles are broad, eosinophilic, and oriented horizontally. In the early stages, there may be an inflammatory infiltrate at the dermoepidermal junction, but in later lesions, only sclerosis and absence of adnexal structures are seen.
A wide variety of systemic metabolic disorders may lead to deposition of material in the skin, often around the eyes or on the lids. Small, yellowish, dome-shaped papules are seen in primary systemic amyloidosis or cutaneous amyloidosis. Histologically, small homogeneous globules may be detected in the dermis, especially around blood vessels. Lipoid proteinosis often demonstrates a characteristic string of small dermal papules with a yellowish hue along the eyelid margins. Again, glycoprotein material is seen as homogeneous bundles or fibers around blood vessels in the superficial dermis (Fig. 7.11).
Xanthelasma commonly occurs in older individuals with normal serum cholesterol. However, in younger patients, it should alert the physician to look for hypercholesterolemia. Soft, yellowish papules and plaques are most prominent on the lower eyelids and cheek but may be seen on the upper eyelids. Histologically, dense clusters of foam cells are found in the superficial dermis, with the intracellular lipid giving it a vacuolated appearance (Fig. 7.12).
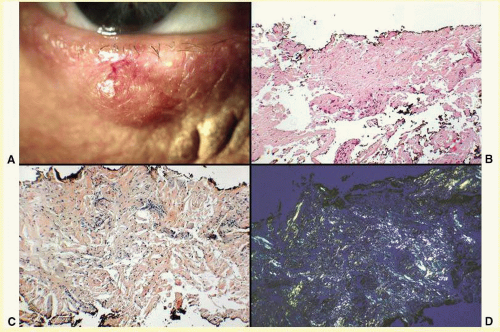 FIG. 7.11 Amyloidosis—A: Erythematous appearance of amyloidosis involving the lid. This was incorrectly diagnosed as a chalazion. B: Amorphous eosinophilic material (amyloid) present within the excised tissue (hematoxylin and eosin stain). C: Positive staining of amyloid material with Congo Red (Congo Red stain). D: When viewed with polarized light, apple-green birefringence of the Congo Red-stained amyloid deposits is visible (Congo Red stain/polarized light). (Photos courtesy of William Morris, MD.) |
Xanthogranulomas are often a manifestation of an underlying systemic condition. Erdheim-Chester disease presents with xanthelasma and xanthogranulomas (Fig. 7.13). Juvenile xanthogranuloma may be single or multiple, orange-hued, firm papulonodules on the face. They may be present at birth but most often arise during infancy. There is a dense, diffuse dermal inflammatory infiltrate characterized by large Touton multinucleated giant cells with an external ring of foamy cytoplasm that encloses a ring of nuclei with an amphophilic center. Most lesions involute spontaneously. Xanthogranulomas may appear on the iris and produce hemorrhage and glaucoma. Histologically, early lesions show a dense collection of histiocytes, some of which have pale, vacuolated cytoplasm. An inflammatory infiltrate of lymphocytes and eosinophils is also present. Mature lesions show the characteristic foam cells and Touton giant cells. Touton giant cells have a central wreath of nuclei surrounded by foamy cytoplasm (Fig. 7.14). In late lesions, the infiltrate is replaced by fibrosis.
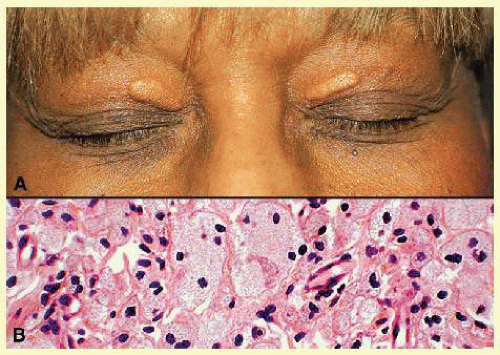 FIG. 7.12 Xanthelasma—A: Clinical photograph of xanthelasma showing typical distribution of the xanthomatous nodules on the eyelids. B: High-power photomicrograph of many multinucleated foamy xanthoma cells (hematoxylin and eosin stain). (Photos courtesy of William Morris, MD.) |
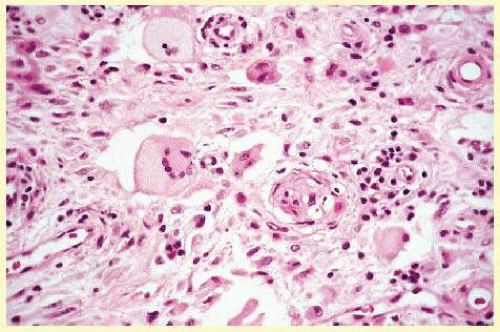 FIG. 7.13 Erdheim-Chester disease—This xanthogranulomatous disease is characterized by dermal infiltrate of fibrohistiocytes and Touton giant cells. The histiocytic cells are S-100 negative. (Photos courtesy of William Morris, MD.) |
Cutaneous histiocytic proliferations (Langerhans cell histiocytosis) represent a spectrum ranging from multifocal lesions involving multiple organs (Letterer-Siwe disease) to unifocal osseous lesions (eosinophilic granuloma). Cutaneous lesions are characterized by a dense, diffuse nodular infiltrates in, with atypical histiocytes demonstrating large, hyperchromatic, kidney bean-shaped nuclei, some of which may infiltrate the epidermis. Characteristic, tennis racket-shaped Birbeck granules may be seen in Langerhans cells on electron microscopy.
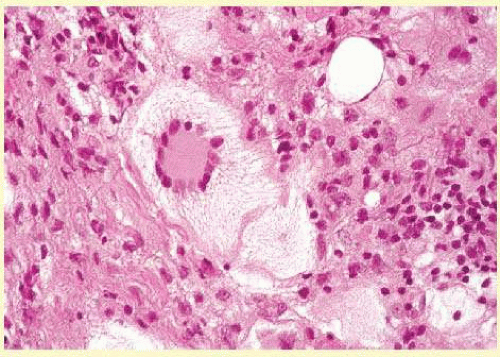 FIG. 7.14 Xanthogranuloma—This Touton giant cell is characterized by a homogeneous eosinophilic center surrounded by a circle of multiple nuclei that is, in turn, surrounded by a large foamy ring (hematoxylin and eosin stain). (Photos courtesy of William Morris, MD.) |
CONGENITAL ABNORMALITIES
Congenital abnormalities are most often diagnosed on clinical morphologic findings; histologic changes are rarely definitive. Phakomatous choristoma is a congenital tumor of the lenticular anlage, which usually involves the medial aspect of the lower lid. Histologically, cells resembling lens epithelial cells and lens “bladder” cells, along with patches of a thick, irregular, PAS-positive basement membrane analogous to the lens capsule, grow irregularly within a dense fibrous tissue matrix (Fig. 7.15).
The ichthyoses are a group of inherited disorders of keratinization characterized by dryness and excessive scaling of the skin. Ichthyosis vulgaris (autosomal dominant) often demonstrates fine scaling of the eyelids, lashes, and surrounding skin; X-linked ichthyosis, additionally, may show large, darker, polygonal scales. One of the two rare autosomal recessive types, lamellar ichthyosis, demonstrates large, thick scales often associated with ectropion of the lids and conjunctival changes. In ichthyosis vulgaris, there is compact orthokeratosis overlying a markedly diminished or absent granular layer without significant inflammation in the dermis (Fig. 7.16). X-linked and autosomal recessive ichthyoses also show compact orthokeratosis, but the changes in the granular layer are not distinctive. In the autosomal-dominant epidermolytic hyperkeratosis, a distinct histologic change is characterized by intracellular edema, vacuolization of keratinocytes, and the appearance of large, clumped keratohyalin granules, especially in the superficial portions of the epidermis.
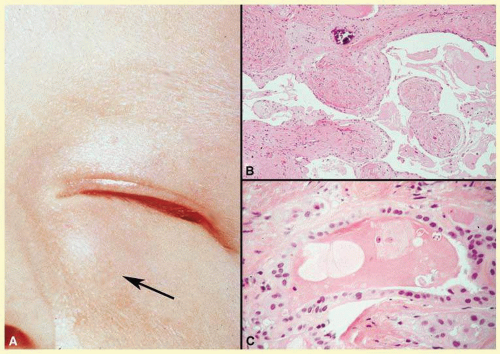 FIG. 7.15 Phakomatous choristoma (Zimmerman tumor)—A: Typical location of a phakomatous choristoma in the nasal portion of the lower lid of an infant. B: Low-power photomicrograph showing collagenous tissue that has cords and nests of epithelial cells with a prominent basement membrane. Dystrophic calcification is also present (hematoxylin and eosin stain). C: Higher-power view illustrates cells similar to “bladder cells” seen in cataractous lenses (hematoxylin and eosin stain). (Photos courtesy of William Morris, MD.) |
Epidermolysis bullosa is a group of related inherited conditions characterized by skin fragility and blistering in a variety of distributions. Histologically, the subcategories are characterized by varied levels of separation in the skin. Subepidermal bullae, which can lead to scarring, may occur around the eyes in one of the most severe forms, autosomal recessive dystrophic epidermolysis bullosa.
AGING
Skin aging is intrinsic (age-related, occurring on non-sunexposed skin) and extrinsic (predominantly sun induced). The epidermis is usually thin with a disorderly maturation of keratinocytes. The most characteristic histologic finding is a tremendous increase in elastic tissue, visualized as basophilic-to-gray staining, amorphous masses in the superficial dermis, often termed basophilic degeneration or solar elastosis (Fig. 7.17). Progression of age-related changes may result in an ectropion (turning out) or an entropion (turning in) of the lower eyelid. Histologically, both show chronic, nongranulomatous, dense inflammation, and scar formation of the skin and conjunctiva. Ectropion shows increased orbicularis and Riolan muscle ischemia, fragmentation of elastic and collagenous tissues in the orbital septum and tarsus, and hypertrophy of the tarsus. Entropion displays increased atrophy of the orbital septum and tarsus. Dermatochalasis is an age-related change manifested by lax, redundant skin of the eyelids. These folds may encroach within the palpebral fissure, thereby impairing vision.
Most of the severe effects of the sun and other environmental factors can be avoided by using sunscreen and avoiding excessive sun exposure. Skin cancers and precancerous lesions are discussed later in this chapter.
CYSTS AND BENIGN, PREMALIGNANT, AND MALIGNANT TUMORS
Cysts
Epidermal Inclusion Cysts and Milia
Epidermal inclusion cysts are follicular cysts of the hair follicle infundibulum, which most often occur on the outer upper portion of the eyelid as firm, round, slow-growing lesions. Cystic dilatation of the follicle occurs from occlusion of the orifice, which may be precipitated by trauma. Milia are identical to epidermal cysts but are smaller. Multiple epidermal cysts, especially of the face and scalp, may occur in Gardner syndrome.
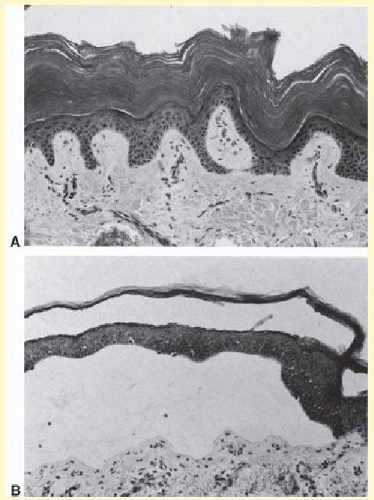 FIG. 7.16 A: Ichthyosis vulgaris showing compact orthokeratosis with a markedly diminished granular layer. B: Epidermolysis bullosa, recessive dystrophic type, with a noninflammatory subepidermal bulla. |
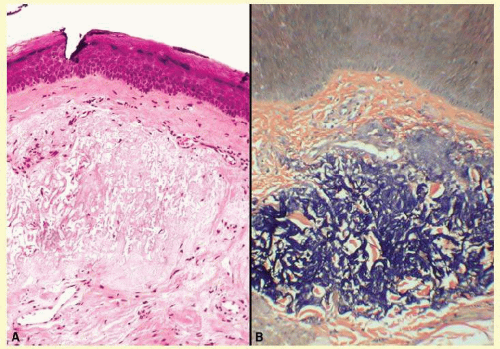 FIG. 7.17 Actinic (solar) elastosis—A: With standard hematoxylin-eosin staining, the areas of sun-damaged collagen stain present a somewhat vermiform appearance and stain more basophilic than the undamaged dermal collagen (hematoxylin and eosin stain). B: The Verhoff-VonGiesen elastic stain stains the damaged collagen like elastic tissue (Verhoff-VonGiesen stain). (Photos courtesy of William Morris, MD.) |
Histologically, epidermal cysts have a wall composed of epidermis with a granular cell layer that is essentially identical to the surface epidermis. Within the cyst, there is loose, laminated keratin, much of which may be lost during processing (Fig. 7.18). Occasionally, the cyst will rupture and produce a foreign body reaction with multinucleated giant cells in the adjacent tissue.
Hidrocystomas
Cysts resulting from occlusion of the eccrine or apocrine duct are referred to as hidrocystomas. Apocrine hidrocystomas are usually solitary and translucent and are often found near the eye. Eccrine hidrocystomas may be solitary or multiple and are clinically indistinguishable from apocrine hidrocystomas.
Histologically, apocrine hidrocystomas are irregularly shaped cysts lined by a double layer of epithelium: the outer layer is myoepithelium, and the luminal layer demonstrates decapitation secretions (Fig. 7.19). Eccrine hidrocystomas are more rounded and show a flattened wall with one or two layers of cuboidal cells (Fig. 7.20).
Pilar (Trichilemmal) Cysts
Pilar, or trichilemmal, cysts were previously referred to as sebaceous cysts. They are less common than epidermal cysts and may arise from hair follicles on the eyelid surface or the brow. These often occur in an autosomal-dominant pattern of inheritance. In contrast to epidermal cysts, these cysts are easily excised and appear as firm, smooth, white cysts. The name, trichilemmal cyst, came about because these cysts are derived from the isthmus portion of the hair follicle from which keratinization analogous to the outer root sheath of the hair, or trichilemma, occurs.
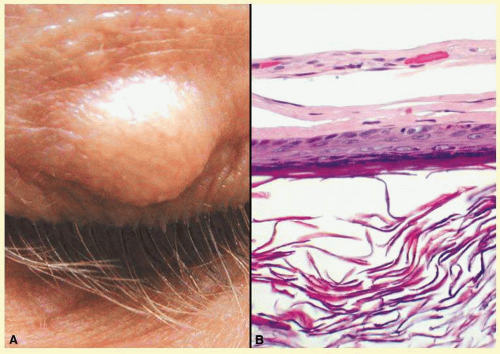 FIG. 7.18 Epidermal inclusion cyst—A: Clinically this cystic lesion usually has a smooth dome-shape and is light yellow to white. B: Histopathologically, this cystic lesion is lined with stratified squamous epithelium that includes the granular cell layer. The lumen is filled with keratin produced by the epithelium (hematoxylin and eosin stain). (Photos courtesy of William Morris, MD.) |
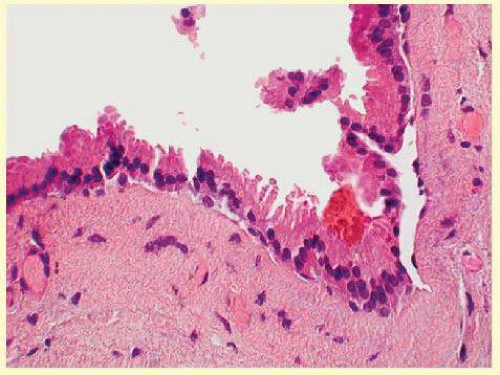 FIG. 7.19 Apocrine hidrocystoma—Apocrine cells line the hidrocystoma wall. Notice the “decapitation snouts” at the apex of the cells, indicating that the cytoplasm has been pinched off to form the glandular secretion (hematoxylin and eosin stain). (Photo courtesy of William Morris, MD.) |
Histologically, pilar cysts possess an epithelial wall without clearly visible intercellular bridges. There is palisading of the peripheral cell layer, and the cells closest to the cyst cavity appear swollen with a pale cytoplasm (Fig. 7.21). Within the cyst cavity, there is homogeneous compact eosinophilic material that can exhibit focal calcification. Cyst rupture is accompanied by a foreign body granulomatous response.
Dermoid Cysts
Dermoid cysts are usually present at birth and commonly occur around the eyes. They may be adherent to the periosteum. Dermoid cysts are believed to result from sequestration of the skin and its appendages along embryonic lines of closure and, thus, are commonly found at the frontozygomatic suture. Histologically, dermoid cysts are lined by epidermis possessing various mature skin appendages. These include hair follicles with terminal hairs, sebaceous glands, eccrine glands, and, occasionally, apocrine glands.
Steatocystoma
Steatocystoma may occur as solitary cysts (simplex) or multiple cysts (multiplex). The latter is often inherited as an autosomal-dominant trait. These cysts are small and firm and, when punctured, exude an oily or creamy fluid. Steatocystoma is derived from cystic dilatation of the sebaceous duct, which empties into the hair follicle. Histologically, the cyst wall is folded and shows several layers of epithelial cells with a palisading of the peripheral cell layer. The cells lining the cystic cavity are covered by a thick, eosinophilic cuticle. Characteristically, flattened sebaceous lobules are present either within or close to the cyst wall.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


