10 Silent Sinus Syndrome Silent sinus syndrome (SSS), is a rare disorder involving the maxillary antrum, characterized by an indolent course of subclinical maxillary sinusitis that leads to progressive contraction of the maxillary sinus. This process can eventually lead to prolapse of the orbital contents, enophthalmos (recession of the globe into the orbital vault) and ensuing ocular symptomatology. Patients with SSS therefore typically present with complaints of asymmetric facial features and visual changes, rather than symptoms typically associated with chronic maxillary sinusitis. The pathophysiology, presentation, imaging, clinical implications, and treatment of this unusual disorder are discussed in this chapter. The first report of SSS was an article by Montgomery in 1964.1 In this paper, the author describes his experience with two patients who experienced diplopia and enophthalmos associated with collapse of the maxillary sinus. Of note, the two patients in this report possessed mucoceles of the maxillary sinus. Subsequently in 1981, Wilkins and Kulwin reported a series of five patients, each of whom presented with spontaneous enophthalmos and ptosis unassociated with antecedent orbital trauma.2 The authors observed that the patients each had unexpected defects in the orbital floor, which was attributed to their chronic, ipsilateral maxillary sinusitis. Thereafter, Wesley et al published another early report of SSS, documenting a single patient who presented with spontaneous enophthalmos without demineralization of the orbital floor.3 The term silent sinus syndrome was first introduced by Soparkar et al in the ophthalmology literature.4 In this report, the authors analyzed an impressive series of 14 patients presenting to Baylor College of Medicine with spontaneous, unilateral enophthalmos and hypoglobus (downward displacement of the globe) associated with “asymptomatic, bone thinning, maxillary sinus disease” through extensive correlation of physical exam attributes along with computed tomography (CT) characteristics. This group coined the term silent sinus syndrome to describe this constellation of ocular and sinonasal findings. None of their 14 patients had signs or symptoms suggestive of intrinsic inflammatory rhinosinusitis. The authors hypothesized that this phenomenon may have been caused by bone remodeling in the maxillary sinus secondary to ostial obstruction in the setting of “hormonal and local influences” in an attempt to explain the findings of a contracted maxillary sinus without symptoms in younger adults. This publication began to give both credence to, and a more concrete definition for, the clinical entity of SSS. There is some controversy in the literature over whether silent sinus syndrome is a distinct condition or a late manifestation of a process termed chronic maxillary atelectasis. The latter condition involves a similar presentation to that seen in SSS, with the exception of associated facial pain, pressure, and nasal congestion in patients diagnosed with chronic maxillary atelectasis. A staging system has been proposed that attempts to annotate the so-called membranous, bony, and clinical progression of deformities in chronic maxillary atelectasis.5 Brandt and Wright recently performed an exhaustive analysis of the available reports in the otolaryngology and ophthalmology literature on chronic maxillary atelectasis and SSS.6 They concluded that these two disorders should be considered clinically indistinguishable, and might better be characterized under a single diagnosis. Although these authors proposed that chronic maxillary atelectasis is a more encompassing, umbrella name for the constellation of findings of SSS, this is not a generally accepted term in the rhinology or otolaryngology community at this point. We will therefore use the term silent sinus syndrome and maxillary atelectasis interchangeably in this chapter. Silent sinus syndrome results from atelectasis of the maxillary sinus, and is generally believed to arise as an unusual consequence of obstruction of the maxillary sinus ostium. Initial hypotheses to address the mechanism for this process suggested silent sinus syndrome may arise in the setting of congenital maxillary sinus hypoplasia. However, this theory has been largely discredited by reports of several patients with normal anatomic relationships of the ostiomeatal complex (OMC) and orbit on CT imaging, who later went on to develop SSS.7–9 These data support the principle that SSS is an acquired condition. The current paradigm is that obstruction of the OMC of the paranasal sinuses leads to hypoventilation of the maxillary sinus. This enclosed cavity in certain settings is thought to develop air resorption, thus creating a suction effect of negative pressure within the maxillary antrum.10–12 The development of a negative pressure vacuum within the sinus, in turn, results in the accumulation of mucous into the antrum, subclinical inflammation, and eventual collapse of the maxillary sinus through attenuation of the bony side walls of this structure. There are experimental reports that provide evidence in support of this theory of the pathophysiology underlying SSS. One study measured inspiratory and expiratory pressures within the maxillary sinus in anesthetized rabbits. The investigators demonstrated that patent, unperturbed ostia had isobaric pressure readings in these animals, but that transient blockade of the maxillary sinus os first produces a spike in elevated antral pressures, followed by a protracted period of measurable negative pressure (>–20 cm H20) within the sinus.13 The development of negative pressure was attributed to the absorption of respiratory gases into the rich capillary network of the sinonasal mucosa within the occluded sinus at this site. A corollary to this work is a report by Kass et al who introduced pressure-sensitive transducers through the membranous posterior fontanelle of patients with maxillary atelectasis. They compared their measurements to the pressures found in the contralateral, unaffected maxillary antrum in the same patient versus a separate cohort of patients with inflammatory rhinosinusitis. This group documented negative pressures (–8.4 cm H20) in the maxillary sinuses of five patients with SSS, compared with isobaric pressure measurements in maxillary sinuses unaffected by SSS.14 This result was later supported by an isolated report of manometric recordings from a patient undergoing endoscopic sinus surgery for silent sinus syndrome. The pressure in the maxillary sinus was found to be –23 mm Hg.11 An overlying principle in the clinical presentation of silent sinus syndrome is that patients with this disorder essentially do not have complaints with regard to their maxillary, or other, paranasal sinuses. Hallmark symptoms of maxillary sinusitis such as infraorbital facial pressure, pain, nasal congestion, and purulent rhinorrhea are notably absent in this patient population. Instead, pathognomonic of SSS is spontaneous enophthalmos and hypoglobus resulting from ipsilateral attenuation of the walls of the maxillary antrum in the distinct absence of clinically evident maxillary sinusitis (Table 10.1). With regard to the orbit, patients with SSS will have normal ocular motility and visual acuity, but the majority of patients will complain of some degree of diplopia.
 Historical Perspective
Historical Perspective
 Terminology
Terminology
 Pathophysiology
Pathophysiology
 Clinical Evaluation and Assessment
Clinical Evaluation and Assessment
Clinical findings of silent sinus syndrome: |
Spontaneous, gradual enophthalmos (eye recession into globe) |
Spontaneous, gradual hypoglobus (inferior descent of eye) |
Ocular asymmetry |
Absence of sinus-related symptoms |
Radiographic findings of silent sinus syndrome: |
Ipsilateral contraction of affected maxillary sinus with volume loss |
Inferior displacement of ipsilateral orbital floor |
Partial to complete opacification of affected maxillary sinus |
Increased orbital volume on affected side |
In addition to the clinical features described above, radiographic evaluation for characteristic changes to the orbit and the paranasal sinuses via CT imaging is required to confirm the diagnosis of SSS.8,15 CT is the gold standard imaging modality for the diagnosis of SSS, although magnetic resonance imaging (MRI) is sometimes utilized.16 The classic CT finding in SSS is the inward retraction of the medial and superior walls of the maxillary sinus associated with a decrease in the maxillary antral volume (Fig. 10.1). Additional imaging findings in SSS typically include a well developed, but opacified, maxillary sinus, occlusion of the maxillary infundibulum due to retraction of the uncinate process, and an expanded middle meatus with increased orbital volume (Fig. 10.2A).
On external physical examination, patients with SSS will have orbital asymmetry due to unilateral enophthalmos and hypoglobus (Fig. 10.2B). This gradual alteration in facial appearance is very commonly the presenting concern for these patients.17 In tabulating past articles of SSS, one group determined that the average reported orbital recession is 2.96 mm (±0.16 mm) and 53% of those patients presented with hypoglobus with an average orbital decline of 2.78 mm (±0.25 mm).6 This concurs with the previously discussed landmark publication by Soparkar et al, showing an average enophthalmos of 3 mm, and average hypoglobus of 3.4 mm.4 Other physical examination findings may include eyelid retraction, narrowing of the palpebral fissure, and lagophthalmos.6,18 On nasal endoscopic examination, patients may have a normal appearance to the nasal cavity on the affected side, or may have subtle alterations such as a widened middle meatal cavity with inward retraction of the uncinate process. Alternatively, the middle meatus may be obscured on endoscopy due to lateral displacement of the middle turbinate toward the uncinate process.15
SSS most commonly presents in the third to fourth decades of life, and appears to affect both genders equally with the exception of one small case series that demonstrated an increased incidence in males.6,10,15 SSS also has a similar incidence in the left and right maxillary sinuses. The average duration of the progressive, characteristic orbitopathies until presentation is 3 months (range 10 days–2 years).4

Fig. 10.1 Coronal computed tomography scan of a patient with silent sinus syndrome. Classic imaging findings seen here include atelectasis of right maxillary sinus walls compared with the left side, reduced right maxillary antral volume and opacification, and increased right orbital volume with clear descent of orbital floor.
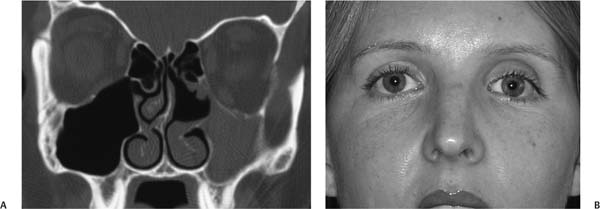
Fig. 10.2 (A) Atelectatic uncinate process. In addition to other classic imaging findings of silent sinus syndrome (SSS), this computed tomography scan demonstrates a retracted left uncinate process that is often found on imaging of the maxillary sinus. (B) Clinical presentation of the same patient presented in Fig. 10.2A with left SSS. Especially notable is this young adult’s facial asymmetry and hypoglobus of the left orbit compared with the right.
Although the vast majority of patients with SSS present as adults, it should be noted that there have been a limited number of case reports of this disorder in children. There are isolated case reports of SSS with classic findings of facial asymmetry and enophthalmos in teenagers presenting with findings suggestive of SSS.19–21 The above reports indicate that, although quite rare, SSS may occur in pediatric patients and should be considered when treating a young patient with facial asymmetry or enophthalmos.
The fact that SSS is an uncommon entity should prompt clinicians and surgeons alike to consider a wide range of disease processes in the evaluation of a patient presenting with enophthalmos and hypoglobus. The differential diagnosis for SSS includes relatively common clinical causes of enophthalmos such as trauma to the orbit (especially blowout fracture of the orbital floor), chronic sinusitis, osteomyelitis, Wegener granulomatosis, orbital metastasis, human immunodeficiency virus (HIV) lipodystrophy, and prior orbital radiation therapy. Several exceedingly rare disorders in the differential include orbital fat atrophy, Recklinghausen disease (absence of the sphenoid wing), linear scleroderma, Parry–Romberg syndrome (progressive hemifacial atrophy), and pseudoenophthalmos.10,18
As we have noted previously, there will be a subset of patients who have classic orbital findings of SSS, but in fact also suffer from symptoms of nasal congestion, rhinorrhea, facial pain, and facial pressure. These patients have, by convention, been considered to have chronic maxillary atelectasis. Except for nomenclature, these patients possess the cardinal signs and symptoms of SSS, and would be treated in the same fashion as SSS. Again, the distinction between SSS and chronic maxillary atelectasis has been largely refuted by recent reports. The finding of sinus symptomatology in the presence of the ocular and radiologic findings discussed should not alter the assessment or interventions employed for patient care.6,22
 Treatment
Treatment
Treatment of SSS is focused on correcting the causative problem that has produced SSS (i.e., maxillary sinus negative pressure leading to structural collapse). Historically, SSS was treated using a Caldwell–Luc approach to enter the anterior face of the affected maxillary sinus. However, as the techniques and technology employed in endoscopic sinus surgery have been refined, this has clearly become the primary treatment modality for SSS.6,10 Key principles of endoscopic surgery in the treatment of SSS are summarized in Table 10.2.
When treating SSS via endoscopic techniques (see Video 10.1), it is critical to first obtain detailed preoperative CT scans to best assess the anatomic relationships present to reduce the possibility of unintended orbital entry during surgery. The surgeon should plan to perform a complete uncinectomy with a wide maxillary antrostomy to expose the entire maxillary sinus to prevent recurrence. The surgeon must be mindful during any endoscopic instrumentation of the uncinate and maxillary sinus in patients with SSS, due to the inferior displacement of the orbital contents in this disorder. With an atelectatic uncinate process lateralized to the medial orbital wall, there is an elevated risk of inadvertent entry into the orbit. Traditional uncinectomy techniques such as the use of a sickle knife to incise the uncinate at its anterior attachment to the lacrimal bone is discouraged in SSS because this practice may result in penetration through the lamina papyracea. A safer technique is to insert endoscopically a ball-tip probe posterior to the free margin of the uncinate and anterior to the lamina papyracea. By dissecting in a location anterior to the lamina papyracea, the uncinate process can be reflected forward and away from the orbit, thereby allowing for safe resection with the use of cutting instruments or a microdebrider. In isolated maxillary sinus involvement, an anterior ethmoidectomy procedure is usually warranted to further expose the landmark of the medial orbital wall, and to liberate the hiatus semilunaris region of the middle meatus from obstruction.
Preoperative review of computed tomography (CT) scan imaging to determine relationship of uncinate and maxillary os to affected orbit |
Preoperative CT scan obtained using image-guidance protocol |
Complete uncinectomy with wide maxillary antrostomy |
Anterior ethmoidectomy for added exposure of hiatus semilunaris and medial orbital wall |
Inferior meatal antrostomy with possible endoscopic medial maxillectomy in select cases |
A notable concern arises during endoscopic sinus surgery if the inferior displacement of the orbit is significant, or more likely, if the acquired atelectasis in the maxillary sinus has precluded safe uncinectomy due to scarring and edema between the uncinate and medial orbital wall/lamina papyracea. In this predicament, the surgeon may need to consider safely exposing the maxillary antrum through an inferior meatal antrostomy, and converting to an endoscopic medial maxillectomy procedure to halt progression of the SSS disease process, ensure a safe sinus, and allow for optimal postoperative examination and debridement in the office setting.
Studies have confirmed the superiority of an endoscopic approach in the treatment of other forms of sinus disease, and the majority of case reports on silent sinus syndrome have indicated good outcomes using endoscopic techniques.6 Complications are essentially the same as would be expected for routine endoscopic sinus surgeries and include infection, bleeding, unintended entry into the orbit with injury to the orbital musculature and/or optic nerve.
In addition to relieving the obstruction of the maxillary sinus ostium, a second surgical procedure to restore the height of the orbital floor may need to be entertained. The indication for this surgery would be persistent orbitopathy after endoscopic maxillary antrostomy and uncinectomy, to restore orbital volume and symmetry. There is some debate regarding whether a one-stage or two-stage surgical approach should be utilized in the treatment of SSS. Vander Meer et al describe successful orbital correction of a series of four patients who received simultaneous endoscopic sinus surgery and orbital floor repair using Medpor malleable mesh (Porex Technologies, Fairburn, GA).9 Preoperative enophthalmos by Hertle exophthalmometry ranged between 1 to 4 mm for these patients. Rose et al followed 14 patients with SSS (termed imploding antrum syndrome in this work), and found that several patients progressed in severity of enophthalmos over time without surgery.16 Six patients eventually underwent silicone block placement to restore orbital floor height. Unfortunately, this group did not document the degree of enophthalmos using standardized measurement criteria, and it is unclear how many of these patients received endoscopic sinus surgery prior to open orbital surgery.
In contrast, Thomas et al followed four patients with SSS, each with a preoperative enophthalmos of 3 mm by Hertle exophthalmometry.23 Two of these patients developed spontaneous resolution of their enophthalmos after endoscopic sinus surgery, to a final displacement of 1 mm over a 6-month period. The latter patients were reportedly content with the resolution in their facial asymmetry, and did not require corrective surgery for the affected orbital floor. In contrast, the remaining two patients in this report each had a residual, persistent enophthalmos of 2 mm after a similar 6-month postoperative interval, and orbital floor reconstruction through placement of an implant was undertaken in a second procedure. For one of these same two patients, volumetric calculations using CT scans were performed with spontaneous resolution of enophthalmos, showing a rebound recovery from 16.9 to 19.6 cubic millimeters of maxillary sinus volume 6 months after endoscopic surgery alone. These data provide objective evidence that after an endoscopic approach for SSS, some patients have natural, progressive improvement in orbital ptosis and maxillary sinus characteristics, thus obviating the need for corrective orbital floor surgery. The benefit of avoiding orbital correction for this disease process has been shown in several other case series as well.24,25
We advocate a two-stage approach; that is, to delay any intervention for augmentation of the orbital floor for at least 6 to 12 months after endoscopic sinus surgery for SSS. This allows for full resolution of any possible infectious agents found in the operated antrum prior to placement of a foreign material implant, and also allows for the possibility of natural resolution of orbital findings and subjective complaints.
The approaches and materials optimal for repair of the orbital floor are beyond the scope of this chapter, but are well described by others.18 Complications resulting from the orbital floor repair include persistence or worsening of diplopia, under- or overcorrection of enophthalmos and a foreign body reaction to materials used in the reconstruction of the orbital floor.
 Conclusion
Conclusion
Silent sinus syndrome is a rare condition in which patients present with enophthalmos and hypoglobus due to subclinical disease of the maxillary sinus. Patients with SSS usually present with facial asymmetry and visual disturbances and, by definition, lack subjective complaints associated with acute or chronic sinus disease. The physical examination of a patient with SSS will demonstrate enophthalmos and hypoglobus, and may have subtle findings of asymmetry on nasal endoscopy. The diagnosis of SSS can be stamped after appropriate CT imaging studies confirm atelectasis of the ipsilateral maxillary sinus. Silent sinus syndrome is effectively treated using endoscopic sinus surgical techniques and image guidance without simultaneous repair of the affected orbital floor. It is important for ophthalmologists, radiologists, oromaxillofacial surgeons, and otolaryngologists to be aware of this condition and its characteristics to make an appropriate diagnosis and offer patients salient options for intervention.
• SSS is a clinical entity characterized by progressive, spontaneous changes to the ipsilateral maxillary sinus and orbit in the absence of typical symptoms of maxillary sinusitis.
• Presenting complaints in SSS typically involve the affected orbit, and include diplopia, enophthalmos, and hypoglobus.
• Several reports lend support to the hypothesis that negative pressure within an obstructed maxillary sinus eventually produces antral atelectasis and orbital floor descent in SSS.
• To confirm the diagnosis of SSS and assist with possible surgical planning, CT is required.
• Endoscopic sinus surgery is a safe and effective strategy to treat the pathophysiologic disease process in SSS appropriately.
• Orbital floor reconstruction can be considered at a separate future surgery if the affected sinus and orbital floor in SSS remain collapsed, and/or if the patient’s orbital complaints persist after confirmed endoscopic surgical correction of the underlying disease.



