Fig. 11.1
Preoperative lymphoscintigraphy in a patient with a lower eyelid melanoma (a). The area of injection and the draining nodes are seen. SPECT/CT scan in the same patient (b). The area of injection of technetium (in blue) in the lower eyelid is seen (c). The draining sentinel lymph node (in blue) in the right parotid area is seen with much higher anatomic resolution compared with the standard lymphoscintigraphy image
One key factor in optimal lymphoscintigraphy is the imaging method. A cobalt 57 source behind the patient is useful for anatomical delineation of drainage along with lateral views [10]. In the past 5 years, use of single-photon emission computed tomography-computed tomography (SPECT/CT) in addition to traditional lymphoscintigraphy has been advocated to help identify additional SLNs and drainage locations (Fig. 11.1b) [11, 12]. SPECT/CT is a system with a dual-head gamma camera and CT scanner. This system allows high-resolution anatomical images to be fused with functional images from the radioactive tracer.
The other key factor in optimal lymphoscintigraphy is tracer characteristics. The smaller the tracer, the faster its drainage. Tracer smaller than 5 nm can penetrate the capillary membrane and enter the bloodstream, whereas tracer larger than 500 μm may be unable to migrate from the injection site [10]. The types of radioactive compounds used can be categorized as radiocolloids, radiolabeled molecules, and radiolabeled macromolecules. Colloids are phagocytosed by macrophages in lymph nodes and thus have a longer resident time in the lymph nodes than noncolloidal macromolecules such as human serum albumin. Antimony sulfide colloid is the most widely used colloid because of its ideal size, 3 nm to 25 nm, and its clearance rate of 40 % over 4 h [13]. Colloids can be filtered to select for smaller particles, which will have shorter transit times. An example of a filtered colloid is filtered technetium Tc 99 m sulfur colloid.
Many different technetium Tc 99 m-labeled compounds have been tried for lymphoscintigraphy in cutaneous melanoma, including sulfur colloid, tin colloid, phytate, and human serum albumin. 99mTc-labeled human serum albumin has also been used commonly in melanoma involving the trunk. When 99mTc-labeled human serum albumin is injected intradermally, it drains rapidly; some would argue that this radiotracer is associated with better definition of the lymphatic system and better reproducibility of results than sulfur colloid [14].
11.4 Technical Considerations in SLN Biopsy for Eyelid Tumors
11.4.1 Preoperative Lymphoscintigraphy
Preoperative identification of the SLN through lymphoscintigraphy aids in surgical planning and preoperative patient counselling. For SLN biopsy of the eyelid, most authors to date have performed preoperative lymphoscintigraphy using filtered 99mTc-labeled sulfur colloid. The lymphoscintigraphy procedure is usually done 1–2 days before the SLN biopsy procedure as described in the following paragraphs.
Filtered 99mTc-labeled sulfur colloid is injected intradermally 1–2 mm around the eyelid tumor or, in the case of conjunctival tumors, in the subconjunctival space at two to four spots around the tumor. The dose of 99mTc-labeled sulfur colloid used is from 0.3 to 0.4 mCi in a volume of 0.2 mL [15, 16]. It is important to ensure that the injection is in the area immediate surrounding the tumor of interest so that the lymphatic drainage mapped reflects the pattern of lymphatic drainage form the tumor site.
At 15 min after radiotracer injection and every 5 min thereafter, a gamma camera is used to take dynamic photos at 30 seconds per frame (Fig. 11.1a). Transmission images are also taken with a low-activity cobalt 57 sheet source every 3 min. It is important to obtain lateral images with and without transmission images. Anatomical markers with cobalt 57 disks are also taped at the thyroid cartilage and suprasternal notch for reference [15, 16].
To allow more precise anatomical delineation, SPECT/CT has been utilized in conjunction with preoperative lymphoscintigraphy [17]. In this approach, SPECT images are acquired with a matrix size of 128 × 128 pixels, at 22 seconds per view over 180°. Axial CT images are used for classification of lymph node level, but the parameters for CT acquisition depend on the CT scanner used and site-specific protocols. Figure 11.1b, c shows the specific identification of an SLN in a patient with conjunctival melanoma using SPECT/CT and traditional lymphoscintigraphy.
A study of 403 patients with cutaneous melanoma in which 149 (37 %) patients had preoperative SPECT/CT found that lymphoscintigraphy plus SPECT/CT identified more SLNs per patient than lymphoscintigraphy alone: a median of 0.34 SLNs versus 0.32 SLNs [12]. The increase in the number of SLNs per patient with SPECT/CT compared to lymphoscintigraphy alone was particularly pronounced in patients who were obese (body mass index of 30 kg/m2 or higher): 25 % of such patients had SLNs detected with SPECT/CT, and only 9.1 % had SLNs detected with lymphoscintigraphy alone. Furthermore, univariate and multivariate analysis showed the use of SPECT/CT to be significantly correlated with better disease-free survival.
11.4.2 Intraoperative SLN Detection
In the preoperative holding area, approximately 1–1.5 h prior to planned surgery, 99mTc-labeled unfiltered sulfur colloid (0.3 mCi in 0.2 mL) is injected in the same fashion as described above for preoperative lymphoscintigraphy. Intraoperatively, the surgeon passes a handheld gamma probe (Fig. 11.2a) over the skin in the area where SLNs were identified on preoperative lymphoscintigraphy, using the lymphoscintigram as a guide. Once the area of high radioactivity is identified, an incision is made directly over this area (Fig. 11.2b). The SLN is then carefully dissected and sent for histopathologic evaluation (Fig. 11.2c).
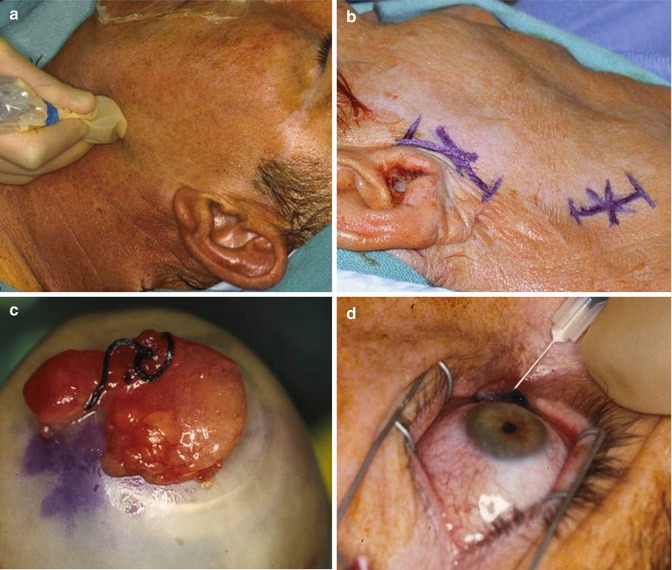
Fig. 11.2
Steps involved in sentinel lymph node biopsy for a conjunctival melanoma are outlined. (a) Intraoperative photograph of the gamma probe which detects the area of increased radioactive uptake (of technetium) corresponding to the draining sentinel lymph nodes based on the preoperative lymphoscintigraphy or preoperative SPECT/CT scan. (b) This photograph shows small skin incisions that are made directly overlying the areas of increased uptake in the draining lymphatic basins to facilitate biopsy of the sentinel lymph nodes. (c) The photograph shows a sentinel lymph node that has been removed from its lymphatic basin. The amount of radioactivity in the sentinel node is checked compared with background to insure it represents the draining lymph node from the primary eyelid or conjunctival lesion. (d) Subconjunctival injection of blue dye can be done using a 30-gauge needle, but given the very small volume that would be required to avoid nonspecific spread of the blue dye in the subconjunctival space, the yield of “blue nodes” was so low in our early experience that the use of the blue dye was abandoned after the first 16 patients who had SLN biopsy for conjunctival tumors as part of the prospective clinical trial at MD Anderson. We now use technetium only as the tracer for sentinel lymph node biopsy for conjunctival and eyelid tumors and find excellent identification rate of the sentinel lymph nodes using technetium alone (This figure is from Esmaeli [58], with permission of Wolters Kulwer Health)
Some authors have injected isosulfan blue dye (Fig. 11.2d) in addition to technetium Tc 99 m sulfur colloid to facilitate visual identification of SLNs in patients with eyelid and conjunctival tumors, but this technique has proven to be of no additional value. One possible reason for the lack of benefit is the fast transition in the head and neck region. Another possible reason is that in the case of conjunctival melanoma, the volume of blue dye injected is smaller (0.2 cc) than for tumors at other anatomic sites in order to avoid diffuse infiltration of the blue dye in all conjunctival quadrants and thus inaccurate and nonspecific drainage [15]. This small volume of blue dye used for conjunctival tumors is probably not large enough to make the SLN blue.
11.4.3 Histopathologic Processing
The histologic evaluation of SLNs is one of the most important aspects of SLN biopsy and can significantly impact the rate of detection of micrometastases. In the past, SLNs were bisected through the hilum, which contains a number of lymphatic vessels, and then cut into 5- to 7-μm-thick sections. However, this method can be inconsistent when the nodes are small and can leave areas of the capsule unexamined. It is therefore better to slice the SLN perpendicular to the long axis from one end of the node to the other to yield 1- to 2-mm-thick slices, a technique sometimes referred to as “bread loafing the SLN.” Each slice is then cut into 5- to 7-μm-thick sections, which are stained with hematoxylin-eosin in the usual fashion. The bread-loafing technique allows for better evaluation of the capsule but may miss the hilum. If the initial section is negative, deeper sections of the block are cut [18]. Using careful serial sectioning of the sentinel lymph nodes can lead to detection of very small foci of microscopic metastasis that are well below the resolution of even the most sophisticated imaging studies (Fig. 11.3).
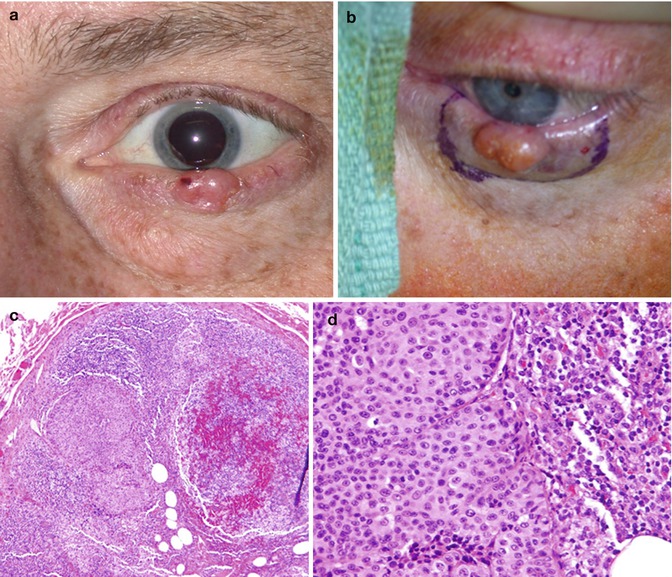
Fig. 11.3
(a) External photograph of a lower eyelid amelanotic melanoma (Breslow thickness 3.8 mm, Clark level IV). The patient had a negative systemic work-up including a negative MRI of head and neck and a negative ultrasound of the parotid area prior to undergoing sentinel lymph node biopsy. (b) Wide surgical excision of the lesion was carried out along with sentinel lymph node biopsy. One positive lymph node was detected in the parotid tail. (c) Histologic section through the parotid sentinel lymph node shows a very small focus of metastatic melanoma that measures 0.8 × 0.5 mm with no extracapsular extension. (d) High-power magnification of the microscopic melanoma metastasis in the sentinel lymph node. This patient subsequently underwent completion neck dissection and parotidectomy which did not reveal any additional positive lymph nodes (Figure from Sanchez et al. [59], with permission from Wolters Kluwer Health)
Immunohistochemical staining is done if hematoxylin-eosin staining of the bread-loafed sections is negative for metastasis or when there are areas of suspicious morphology. Immunohistochemical stains used to evaluate SLNs include anti-S100, HMB-45, anti-MART1, and anti-tyrosinase for melanoma [18]; cytokeratin 20, chromogranin, and antibodies to Cam5.2 for Merkel cell carcinoma [19] and sebaceous carcinoma; and anti-adipophilin and anti-perilipin antibodies for sebaceous carcinoma [20].
11.5 Indications for SLN Biopsy for Eyelid Tumors
Accurate determination of regional lymph node status in patients with eyelid and conjunctival neoplasms not only is important for staging disease and estimating prognosis but also may increase survival through early detection of microscopic metastasis. Here, we discuss the rationale for and indications for SLN biopsy for the major types of eyelid and conjunctival neoplasm.
11.5.1 Melanoma
Experience with SLN biopsy for cutaneous malignancy started with melanoma, and most of the research to date on SLN biopsy for cutaneous malignancy has been done in patients with this disease. In a series of 612 patients with cutaneous melanoma at least 1.0 mm thick, Clark level IV or ulceration, and no clinical evidence of regional or distant metastasis who underwent SLN biopsy, SLN status was a significant predictor of disease-free survival and disease-specific survival in both univariate and multivariate analyses [21]. The 3-year disease-free survival rate was 88.5 % in patients with negative SLNs versus 55.8 % in patients with positive SLNs. In multiple covariant analysis, SLN status was a stronger predictor of disease-free survival than tumor thickness, Clark level, or ulceration. Another series of more than 670 consecutive patients with melanoma found that patients who had SLN biopsy had a significantly better recurrence-free survival, distant metastasis-free survival, and overall survival compared with patients with similar characteristics who did not have SLN biopsy. 5-year melanoma-specific survival rate with Kaplan-Meier analysis was 84.8 % in patients with SLN biopsies versus 80.3 % without [22].
Based on a study of 44 patients with eyelid skin melanoma, the Collaborative Eyelid Skin Melanoma Group concluded that melanoma of the eyelid has a regional nodal metastasis rate of 11 % and a distant metastasis rate of 7 %, with a mean follow-up of 34 months [23]. Another study, of 29 patients with eyelid skin melanoma from Australia, found that 17 % of patients experienced local recurrence and 7 % (2 of 29 patients) of patients died of metastatic melanoma [24]. Several studies have demonstrated that the risk of nodal metastasis increases with increasing tumor thickness [23, 25]. In the largest series to date of SLN biopsy for ocular adnexal melanomas, 30 patients with conjunctival and/or eyelid melanoma had SLN biopsy. Risk factors associated with a positive SLN included tumor thickness greater than 2 mm and presence of ulceration (Fig. 11.4) [25].
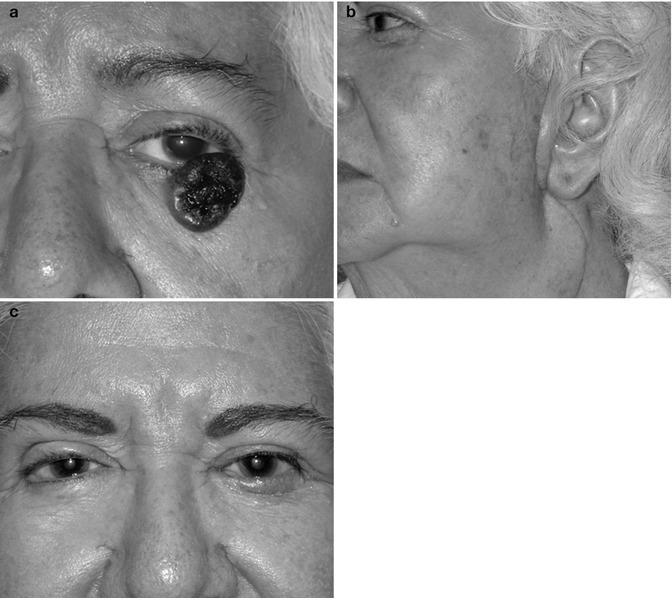
Fig. 11.4
(a) Left lower eyelid melanoma (Breslow thickness 7.2 mm with histologic ulceration, Clark level II) with no palpable lymph nodes, with a negative ultrasound and MRI of the regional lymph nodes. The patient underwent surgical removal of the melanoma simultaneous with sentinel lymph node biopsy which demonstrated one positive sentinel lymph node in the parotid gland. (b) The patient subsequently had completion neck dissection and parotidectomy which showed two additional positive nodes (in addition to the previous positive sentinel lymph node). The photograph shows the incision for the parotidectomy/neck dissection which is much larger than the incisions needed for the sentinel lymph node biopsy; parotidectomy and completion lymph node dissection only become necessary in patients who have a positive sentinel lymph node. (c) This patient was doing well without evidence of disease at last follow-up 3 years after removal of her eyelid melanoma and additional treatments for her positive sentinel lymph node (Figure from Savar et al. [25], with permission from Elsevier, Inc.)
11.5.2 Squamous Cell Carcinoma
Although it accounts for only 9 % of eyelid tumors, squamous cell carcinoma is the second most common eyelid malignancy after basal cell carcinoma [26]. Squamous cell carcinoma has a higher rate of local recurrence than basal cell carcinoma, and squamous cell carcinoma, unlike basal cell carcinoma, has the potential for regional nodal metastasis. In a series of 111 patients with advanced eyelid squamous cell carcinoma treated in a head and neck surgery department at a tertiary cancer center, local recurrence occurred in 41 patients (36.9 %), and regional nodal metastasis occurred in 27 patients (24.3 %) [27]. Distant metastasis occurred in only seven patients, but five of them died of the metastatic disease. In patients with squamous cell carcinoma of the eyelid with high-risk features such as lesion wider than 2 cm, locally recurrent disease, or perineural invasion, SLN biopsy should be considered.
Maalouf et al. reported their experience with SLN biopsy in nine patients with squamous cell carcinoma of the eyelid and conjunctiva with a median follow-up of 22 months. SLNs were successfully identified in all nine patients, and one of the nine patients had a positive SLN [28]. There were no local recurrences or deaths in their series.
11.5.3 Sebaceous Carcinoma
Sebaceous carcinoma is often associated with a delay in diagnosis because it can mimic benign lesions such as chalazion and blepharoconjunctivitis. In a series of 60 patients with sebaceous carcinoma of the eyelid, 11 patients (18 %) had local recurrence, and 5 patients (8 %) had clinical nodal metastasis. Of the patients with clinically palpable nodal metastasis, 4 patients (80 %) died of metastatic disease [29]. A recently published study demonstrated that lymph node metastasis was correlated with American Joint Committee on Cancer T category in patients with eyelid sebaceous carcinoma [30]. This study showed nodal metastasis only in patients with tumors at least 9 mm in greatest diameter. The study also showed that patients with T category of T3b or worse at presentation had poorer disease-specific survival.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


