Secondary Orbital Tumors
Jill S. Melicher Larson
Yian Jin Jones
Jeffrey A. Nerad
Secondary orbital tumors extend to the orbit from adjacent and contiguous structures, such as the periorbital sinuses, nasopharynx, bone, intracranial cavity, eyelids, conjunctiva, lacrimal sac, and globe. Orbital metastatic disease is carried by hematogenous spread of tumor from distant sites such as the breast, lung, and prostate. Primary orbital tumors, by definition, arise from structures within the bony orbit. Secondary orbital tumors are classified by location from which extension into the orbit occurs. In this chapter we will discuss some of the most commonly occurring tumors arising from the paranasal sinus, brain, eyelid, ocular structures, and globe. Given the complexity of medical and surgical management, a patient-centered, multidisciplinary approach involving specialists in ophthalmology, otolaryngology, neurosurgery, and oncology is preferred in the evaluation and treatment of secondary orbital tumors.
CLINICAL EVALUATION
Secondary orbital invasion of tumors may occur silently with orbital signs and symptoms not presenting until the tumor is fairly advanced. The approach to a patient with an orbital tumor centers on a thorough head and neck and ophthalmic evaluation, starting with a careful subjective history. The onset, duration, and progression of ocular signs and symptoms including changes in visual acuity, epiphora, diplopia, eyelid edema, ptosis as well as pain or paresthesias should be elicited. Other symptoms such as history of sinus infections, epistaxis, nasal discharge, or obstruction are very important in determining a sinonasal origin of the disease process. The seven “P” s of orbital history and physical examination is a systematic way to evaluate the orbit tumors.1
Seven “P’s of orbital history:
Past medical and surgical history
Pain
Progression
Proptosis
Palpation
Pulsation
Periorbital changes
Past medical and surgical history give important clues to the diagnosis of a secondary tumor invading the orbit. A history of basal cell carcinoma excision in a patient with orbital symptoms could lead to the suspicion for recurrent disease. The indolent and painless course and slow progression of many secondary orbital tumors contribute to the typically advanced presentations of patients with orbital invasion. However, pain and paresthesia were reported in 60% of cases of sinonasal tumors invading the orbit.2
Examination of globe position to determine axial or nonaxial displacement of globe provides clues to the etiology of disease process. Proptosis is a hallmark of orbital disease. Hertel exophthalmometry should be obtained to quantify proptosis. The average Hertel measurements are 20 mm for the white population, 18 mm in patients of Asian descent, and 22 mm in the black African American population. Nonaxial displacement of the eye is often seen in patients with secondary orbital tumors. If the eye is pushed downward and laterally, it may indicate frontal or ethmoid sinus disease. A maxillary sinus lesion produces upward displacement of globe. Rarely, medial displacement of the eye may occur, indicating a lacrimal gland tumor or temporal fossa mass.1,2
The consistency, size, shape, and mobility of a palpable mass should be noted when examining a patient with an anterior orbital mass. Palpation of the orbital rim and the superior and inferior fornix should be performed. Pulsation of the orbit is rare, especially in the context of secondary orbital tumors; however, should be noted. Malignant eyelid lesions of epithelial origin such as basal cell carcinoma and squamous cell carcinoma often present with one or more of the following characteristics:
Ulceration—Malignant tumor cells can outgrow their blood supply and cause ulceration and bleeding; however, they tend not to be tender or painful.
Induration—A hard lesion suggests malignancy.
Irregularity of margins—Due to the differential growth rates of tumor cells, lesions have irregular borders.
Telangiectasia—Focal telangiectasia on the borders of a tumor suggests malignancy.
Loss of eyelid margin architecture—Loss of lashes (madarosis) and destruction of eyelid margin are signs of malignancy.1
The physical examination assists in formulating a differential diagnosis. However, diagnostic imaging is the key in defining the extent and localization of orbital tumors and to narrow the differential diagnosis. Computerized tomography (CT) and magnetic resonance imaging (MRI) techniques are used to assess the degree of orbital involvement by invading tumors. Often the techniques are complementary and used together.
CT measures the absorption of X-rays and excels at the evaluation of fine bony detail. Because of the sharp radiodensity contrast between air and soft tissue versus bone, small erosion, remodeling, or expansion of the bony structures and subtle mucosal thickening can be better appreciated on CT. Dense bone in the orbital apex obscures detail on CT scans, however. MRI is used to evaluate lesions affecting the orbital apex. MRI is particularly useful in evaluating soft tissues by using pulse sequences to differentiate various tissue properties. In cases of aggressive lesions, MRI is best used to define the extent of invasion into surrounding soft tissue structures and is often used for tumor staging. MRI is also superior to CT in the detection of perineural spread.1,3
ANATOMIC CONSIDERATIONS
Understanding the anatomic relationship between structures is particularly important in secondary orbital tumors. The paranasal sinuses share common, thin walls with the bony orbit.
Orbital roof = floor of frontal sinus
Medial wall of orbit = lamina papyracea of the ethmoid
Medial orbital apex = anterolateral wall of sphenoid sinus
Orbital floor = roof of maxillary sinus
Neoplastic processes from the sinuses and brain have ready access to the orbit through preformed pathways, such as the anterior and posterior ethmoidal foramina within the frontoethmoid suture line, nasolacrimal duct, inferior and superior orbital fissure, optic canal, and so on. The infraorbital canal is separated by a thin plate of bone from the maxillary sinus mucosa, which opens posteriorly into the inferior orbital fissure and serves as a direct route of spread of maxillary sinus tumors.4
GENERAL MANAGEMENT PRINCIPLES
The treatment of secondary orbital tumors varies depending on site of origin, cell type, and extent of the lesion. Treatment can include one or a combination of the following: surgical excision, chemotherapy, and radiation. Preoperative radiation and neoadjuvant chemotherapy, a chemotherapeutic regiment given prior to surgical resection to achieve tumor reduction, have been advocated in certain tumors. Radiation and chemotherapy given after surgical debulking or excision have also been researched with some possible benefit to increase survival. Historically, orbital exenteration was considered necessary for improving survival in treating secondary tumors in the orbit. More recently, several studies have demonstrated that orbital preservation in selected patients does not adversely impact local control or survival.4,5,6,7
PERIOCULAR SKIN AND EYELID TUMORS
Periocular skin and eyelid malignancies account for most secondary orbital tumors and develop through local invasion.8,9,10 Ten percent of all cutaneous carcinomas arise in the periocular region.11 The most common malignant skin neoplasm invading the orbit is basal cell carcinoma, followed by sebaceous carcinoma, squamous cell carcinoma, and malignant melanoma. Primary cutaneous carcinoma may invade the orbit for any of the following reasons: (i) late presentation, (ii) multiple recurrences following incomplete excision, (iii) rapid and aggressive growth, and (iv) atypical or insidious onset resulting in delayed diagnosis.
BASAL CELL CARCINOMA
Basal cell carcinoma (BCC) arises from basal cells in the lower epidermis and accounts for 90% of malignant eyelid tumors in the United States. It is the most common epithelial malignancy of the eyelid. It most commonly involves the lower lid (50%–60%) and the medial canthus (25%–30%). Basal cell carcinoma has a male predilection and occurs in older individuals (40–80 years of age) with fair skin and a history of unprotected sun exposure.12,13,14 Basal cell carcinoma is usually slow growing, locally invasive, and rarely metastasizes but can lead to significant morbidity in the periocular region due to orbital invasion.
Clinical Presentation
Basal cell carcinoma usually presents as a mass lesion (Fig. 46-1). There are four morphologic forms: (i) nodular (including the subtypes micronodular and noduloulcerative), (ii) superficial, (iii) infiltrative (including the subtype morpheaform), and (iv) mixed (or basosquamous type). Nodular (including noduloulcerative) BCC is the most common form (50%–70%), appearing initially as small, firm, pearly papules or nodules with overlying telangiectasias. Nodular BCC may grow into a dome-shaped tumor with central ulceration (noduloulcerative). The micronodular subtype (15%) shows smaller tumor nodules (<0.15 mm by definition) and has a higher tendency for subclinical extension. Superficial BCC (15%) appears as a scaly erythematous patch or plaque and often occurs in multiples that may resemble chronic dermatitis. Nodular and superficial BCCs are the least aggressive forms. Infiltrative BCC (15%) is characterized by irregular tumor cell infiltration; the morpheaform subtype of infiltrative BCC (5%) may appear as a pale, indurated, slightly elevated lesion with ill-defined margins that tends to grow laterally beneath the epidermis.14
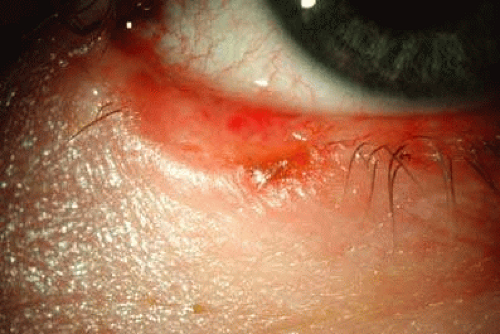 Figure 46-1. Infiltrative basal cell carcinoma of the lower eyelid. |
Orbital invasion of basal cell carcinoma is rare, with a reported incidence in less than 5% of cases, typically occurring secondary to neglected and long-standing primary tumors arising from the medial canthus.14 Medial canthal tumors are also more likely to be recurrent after initial resection secondary to less aggressive resection techniques in this region to minimize the difficulty in reconstruction of this region. Orbital invasion may also be seen in tumors with an aggressive histologic growth pattern.
The following are signs of orbital invasion with BCC:
Visible or palpable mass
Fixation of the tumor mass to adjacent bone
Limitation of ocular motility and presence of diplopia
Globe displacement
Eyelid ptosis
Epiphora
Skin fistula
Patients at risk for orbital invasion or where clinical suspicion exists should undergo appropriate imaging. Leibovitch et al14 showed a series where there were no specific signs of orbital invasion other than a palpable mass.
Risk Factors for Orbital Invasion
The following are risk factors for orbital invasion with BCC:
BCCs with infiltrative (morpheaform), mixed (basosquamous), and nodular (micronodular) histologic characteristics are at higher risk of subclinical extension, incomplete excision, recurrence, and orbital invasion.13 In a recent large series study, Leibovitch et al.14 reported that the most common type of BCC associated with orbital invasion was the infiltrative form.
Tumor factors:
Location: BCC arising in the medial canthus accounts for 56% of cases with orbital invasion (Fig. 46-2).14
Perineural invasion: Patients with presence of perineural invasion (PNI) are at high risk of tumor recurrence due to skip areas that make surgical margins difficult to assess. In the study of Leibovitch et al14, PNI was present in 19% of patients. Of these patients, 92% had tumor recurrence.
Treatment history: Long-standing, clinically neglected (Fig. 46-3), incompletely excised, recurrent, and histologically aggressive tumors are at high risk for orbital invasion. A study done by Richmond and Davie15 postulates that incomplete removal at the time of initial excision may contribute to tumor recurrence secondary to the formation of scar tissue, obscuring signs of clinical recurrence.
Patient factors: Older age, male sex, and immunosuppressed patients.
 Figure 46-2. Ulcerative basal cell carcinoma originating at the medial canthus with medial orbital invasion. |
 Figure 46-3. Long-standing, clinically neglected ulcerative basal cell carcinoma arising at the medial canthus with orbital invasion and trochlea involvement. |
Evaluation
Clinical Evaluation
Clinical assessment and careful history are helpful for the initial diagnosis, and imaging studies are the mainstay of evaluations of orbital invasion of eyelid basal cell carcinoma.
Imaging
Computed tomography scan (1–2-mm slices) with bone windows is used to evaluate the bony orbit. On CT, orbital invasion appears as a mildly enhancing, homogenous mass with irregular borders. One quarter of patient’s with orbital invasion will have bony destruction visible on CT.14,16,17 MRI will provide more detailed evaluation of orbital soft tissues. T1 gadolinium-enhanced, fat-suppressed MRI is the modality of choice for demonstrating soft tissue changes associated with orbital invasion from eyelid tumors.17 The T1-weighted MRI is characterized by a low signal intensity, homogenous, mildly enhancing mass with irregular borders.14
Biopsy
Biopsy can be carried out by open, incisional biopsy or in some cases fine-needle aspiration (FNA). FNA is used when a mass is visible or palpable and can be approached safely. Excision must be performed when the diagnosis is confirmed. Mohs micrographic surgery as an outpatient, or excision with frozen sections carried out in the operating room, allows the development of controlled surgical margins and identification of the posterior extent of the tumor. The more aggressive infiltrative form (morpheaform) makes up more than 80% of cases of orbital invasion in the Leibovitch study.14
Treatment
Treatment is based on clinical exam, imaging, and the patient’s overall systemic condition. In cases with anterior orbital involvement, the lesion may be locally resected. Careful pathologic examination of surgical margins is necessary at the time of initial resection.16 Cure rates with Mohs micrographic surgery are excellent. The Australian Mohs database reports the 5-year recurrence rate in periocular tumors of zero in primary basal cell carcinoma and 8% for previously resected basal cell cancers.18 Mohs micrographic surgery may be performed to obtain surgical margins around the tumor prior to surgical excision. This technique allows tissue-sparing excision and ensures the development of tumor-free margins (Fig. 46-4). In most cases with extensive orbital involvement, exenteration is necessary, which may be followed by radiotherapy. Exenteration was recommended for all patients in a series by Howard et al.16 and was recommended for 75% of patients in the study performed by Leibovitch et al.14 Factors limiting treatment with orbital exenteration include patients with only one good-seeing eye, unresectable tumor with intracranial invasion, and patient refusal of orbital exenteration.
 Figure 46-4. Long-standing, clinically neglected ulcerative basal cell carcinoma arising at the medial canthus with orbital invasion and trochlea involvement. Forehead and eyelid margins obtained with Mohs micrographic surgery technique prior to resection. |
Squamous Cell Carcinoma
Squamous cell carcinoma (SCC) is the second most common malignant eyelid tumor, accounting for 5% to 10% of all eyelid malignancies with an incidence of 0.09 to 2.42 cases per 100,0008,19,20,21 Squamous cell carcinoma arises from the prickle-squamous cell layer of the epidermis with the hallmark feature of extension into the underlying dermis. Squamous cell carcinoma occurs most frequently on the lower eyelid, followed by the medial canthus, upper eyelid, and lateral canthus.20 SCC appears to be related to a history of ultraviolet light exposure, occurring more frequently in fair-skinned, elderly individuals with a mean presentation in the seventh decade.19 Other risk factors include HPV, exposure to chemicals (including arsenic, hydrocarbons, and smoke), history of prior radiation, genetic disease (i.e., albinism, xeroderma pigmentosum), and immunosuppression following organ transplantation or in individuals with AIDS. Squamous cell carcinoma is uncommon in persons of African American, Asian, and Hispanic descent.19
Clinical Presentation
SCC often presents as a painless nodule or plaquelike lesion with irregular rolled edges, chronic scaling, fissuring of the skin, pearly borders, telangiectasia, and central ulceration, with a more rapid onset than basal cell carcinoma.21,22 It may arise de novo in normal skin or from a pre-existing lesion such as an actinic keratosis, Bowen disease, xeroderma pigmentosum, or following radiation therapy to the eyelid. Perineural infiltration (PNI) may facilitate spread into the orbit and may be the presenting feature of orbital involvement. In contrast to the typical indolent nature of basal cell carcinoma (BCC), eyelid SCC can be aggressive, invading not only the orbit, but also metastasizing to lymph nodes and distant sites, causing significant morbidity and mortality.19
Risk Factors for Orbital Invasion
Periocular SCC is the most common secondary epithelial neoplasm to invade the orbit.22,23 Adverse prognostic factors associated with orbital invasion are previous recurrence, late presentation or neglect, advanced age, large lesion size (Figs. 46-5A and B), poor histologic differentiation, history of immunosuppression, and presence of perineural invasion.23 Incomplete primary excision of lesions in the medial canthal region and moderate to poorly differentiated SCC are the main risk factors for recurrence (Fig. 46-6).24
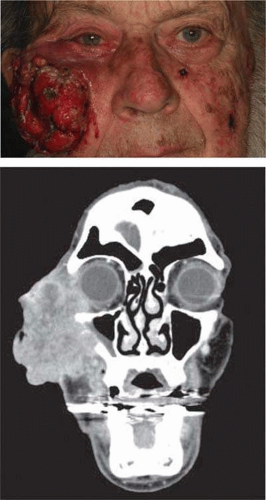 Figure 46-5. Periocular squamous cell carcinoma with orbital invasion. Long-standing, neglected tumor resulting in orbital invasion. |
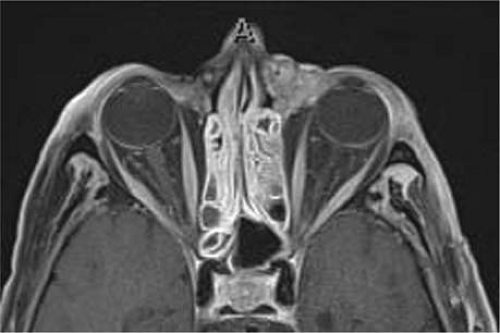 Figure 46-6. Recurrent squamous cell carcinoma with orbital invasion following previous medial canthal tumor excision. |
Signs of Orbital Invasion
Like BCC, signs of orbital invasion include visible or palpable lesion, fixation to bone, limitation of ocular motility, globe displacement, eyelid ptosis, epiphora, and fistula formation. Once the orbit is invaded, the tumor spreads along fascial and fatty tissue planes, resulting in difficulty with excision. Orbital invasion of SCC through perineural spread along the branches of the trigeminal, facial, or motor nerves of the extraocular muscles produces symptoms of pain, facial weakness, decreased or altered sensation, ptosis, ophthalmoplegia, and blindness. PNI facilitates spread to the orbit and subarachnoid space through a path of least resistance.25
Evaluation
Clinical examination
In addition to documenting the location, size, and character of the lesion, it is important to evaluate subcutaneous tissues for lesion depth and presence or absence of bony fixation, and also to palpate for preauricular, submandibular, and cervical lymphadenopathy.
Biopsy
Clinical presentation of SCC is variable. Prompt biopsy is critical to establish the diagnosis and direct treatment. Incisional biopsy is performed for large lesions; smaller lesions may be removed with excisional biopsy and margin control. Fine-needle aspiration may be performed for diagnosis of nodal metastasis.
Imaging studies
Magnetic resonance imaging is used to evaluate the depth of extension and presence of orbital invasion. Computed tomography is used to evaluate for presence of bony erosion. PET scan may be indicated to evaluate for metastatic disease.
Treatment
Surgical Excision
Complete surgical excision of periocular lesions without orbital extension and negative margins offers a cure rate of 99%.25 Mohs micrographic surgery and excision with frozen section or permanent section can be used to treat eyelid SCC with the highest cure rate and lowest frequency of recurrence.19,20,24 Mohs micrographic surgery is the preferred technique for surgical excision of SCC with relatively low recurrence rates reported at 3.6%, lower than other treatment modalities.26
Exenteration
Exenteration is reserved for patients with progressive disease that cannot be cured with wide surgical excision or in patients where excision would yield a defect not amenable to reconstruction, resulting in an uncomfortable or nonseeing eye. Involved bone may require excision or burring with removal of involved sinus mucosa or periorbita. Margin control in patients with perineural invasion can be difficult secondary to skip areas within the perineural spread. Confirmation of nodal metastasis can be made by FNA. Lymph node dissection is used for regional lymph node metastases. Dermal metastasis may also exist with skip lesions (Fig. 46-7). If the patient has advanced disease with involved margins or metastases, adjuvant radiotherapy may be required.20,21,23 Squamous cell carcinoma with orbital extension is often associated with advanced disease and may include intracranial extension. Adjuvant radiotherapy may be helpful to improve patient quality of life and prolong survival.
 Figure 46-7. Biopsy-proven dermal metastasis of squamous cell carcinoma. |
Radiotherapy
Use of radiation in the treatment of periocular tumors is limited by the presence of the surrounding radiosensitive tissue and the relative radio insensitivity of BCC and SCC. Radiotherapy can be used, albeit rarely, as primary treatment of eyelid SCC but is often used as adjunctive postsurgical treatment. Combined surgery and radiotherapy may improve local-regional control and outcome in high-risk SCC.19,23 Radiation may also provide palliative treatment of advanced tumors with orbital extension and distant metastases.19
Squamous cell carcinoma is an aggressive epithelial malignancy in the periorbital region due to the propensity for orbital and perineural invasion and regional nodal metastasis. Moderate to poor differentiation, large lesions, and the presence of perineural invasion increases the risk of orbital extension. Patients with high-risk characteristics should undergo clinical evaluation for nodal metastasis and orbital imaging with MRI. Treatment of squamous cell carcinoma amenable to local excision should be treated with Mohs micrographic surgery or wide surgical excision with frozen sections. If orbital invasion is present, orbital exenteration may be necessary. Adjunctive treatment with radiation postoperatively should be considered. These patients require close surveillance for recurrence.
Sebaceous Gland Carcinoma
Sebaceous glands are an epidermal appendage, generally associated with hair follicles. The malignant sebaceous gland carcinoma (SGC) most commonly arises in the periocular area, usually in the eyelid. The most common site of origin is the meibomian glands of the tarsal plate, followed by the glands of Zeis, and other sebaceous glands in the caruncle or eyebrow.27 Sebaceous gland carcinoma may be multicentric in origin. This tumor is more common in women and occurs most often in the seventh decade of life. There is a slight predilection for the upper eyelid. In the United States, sebaceous carcinoma accounts for 0.2% to 0.7% of all eyelid tumors and 5% of all malignant eyelid tumors.8,20,27,28,29,30 Sebaceous carcinoma of the orbit occurs as secondary invasion from the eyelid or bulbar conjunctiva.
Clinical Presentation
The clinical appearance of sebaceous carcinoma (SebCC) is highly variable. It may mimic benign conditions such as chronic blepharoconjunctivitis. SebCC is commonly misdiagnosed (>50%) initially with a median duration of symptoms to final diagnosis of 24 months. The presence of a diffuse unilateral thickening of the eyelid with papillary hypertrophy and prominent yellow streaks has been characteristically described as the tigroid appearance of sebaceous gland carcinoma (Fig. 46-8).30 In usual cases, the tumor may present as a painless, firm, round, yellowish, subcutaneous nodule that may vaguely resemble a chalazion secondary to the presence of lipid. Lesions at the eyelid margin can also show keratinization appearing as a cutaneous horn.28 Tumors invading hair follicles at the eyelid margin commonly cause loss of eyelashes (madarosis). The presence of lash loss helps to differentiate sebaceous gland carcinoma from benign lesions such as chalazia and blepharitis (Fig. 46-9).20
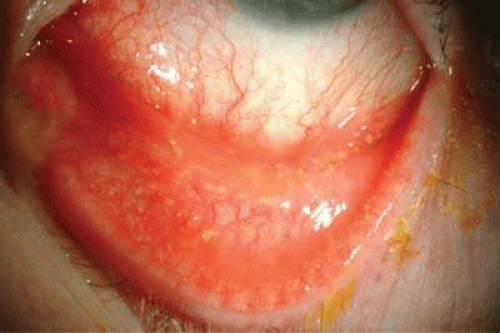 Figure 46-8. Papillary hypertrophy with yellow streaks illustrating the tigroid appearance of sebaceous gland carcinoma. |
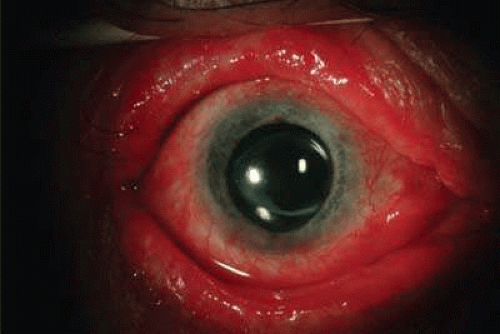 Figure 46-9. Madarosis and unilateral “blepharitis” suggest sebaceous gland carcinoma and full-thickness eyelid biopsy is recommended. |
Risk Factors for Orbital Invasion
SGC spreads by direct extension into adjacent structures including the orbit, paranasal sinuses, and the intracranial cavity. The tumor metastasizes through lymphatic channels to regional lymph nodes and uncommonly metastasizes to visceral organs. Factors associated with orbital invasion include the following: poorly differentiated, highly infiltrative SGC with multicentric origin, SGC arising in the caruncle, misdiagnosis or delay in diagnosis, large lesion size, diffuse involvement of both the upper and lower eyelids, and signs of intraepithelial or pagetoid spread.8,20,28,29,30 In a review of 52 cases of orbital exenteration for sebaceous carcinoma, Jakobiec and Albert.31 found that conjunctival epithelial involvement occurred in 100% of cases. Pagetoid spread is associated with a poorer prognosis.
Evaluation
Clinical evaluation
A comprehensive examination of the eyelid, conjunctiva, caruncle, and adjacent areas, especially lymph nodes, should be carefully performed. Clinical examination of regional lymph nodes should be performed. Sebaceous gland carcinoma can be associated with Muir-Torre syndrome. Muir-Torre is a genetic syndrome associated with mutations of MSH2 and MLH1 genes, resulting in multiple sebaceous gland carcinomas and visceral, typically colonic, malignancy. Screening colonoscopy is recommended in all patients with sebaceous cell carcinoma.30,32,33
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


