Fig. 6.1
Sebaceous gland carcinoma arising in left upper eyelid – a firm, sessile subcutaneous round nodule fixed to the tarsus (Courtesy of Dr. Santosh Honavar)
6.5.2 Diffuse Thickening of the Eyelid
Unilateral diffuse thickening of the eyelid is the second most frequent presentation of SGC. The diffuse tumor may extend into the epithelium of the forniceal or bulbar conjunctiva, and even the cornea (Fig. 6.2). Rarely, SGC arising from the glands of Zeis can become pedunculated, keratinized, and even appear as a cutaneous horn. When SGC develops in the caruncle, it appears as an irregular yellow mass that usually is not fixed to adjacent structures [1, 11].

Fig. 6.2
Diffuse involvement of the eyelids by sebaceous gland carcinoma causing loss of cilia (Courtesy of Dr. Santosh Honavar)
6.6 Histopathologic Features
6.6.1 Pathogenesis
Periocular SGC arises from the sebaceous glands in the ocular region, including meibomian glands in the tarsus, glands of Zeis of the cilia, pilosebaceous glands of the caruncle, and from the conjunctival epithelium [1]. It may exhibit multicentric origins [12, 13]. Most SGC appear to arise de novo and not from a preexisting sebaceous adenoma, sebaceous hyperplasia, or sebaceous (organoid) nevus [1].
6.6.2 Light Microscopic Features
Histopathologically, SGC is an unencapsulated infiltrating mass composed of cells with finely vacuolated, frothy cytoplasm, pronounced nuclear pleomorphism, and usually high mitotic activity (Fig. 6.3) [1]. The presence of lipid can be demonstrated with the oil red-O stain (Fig. 6.4). This lipid can incite a foreign body giant cell reaction. SGC is associated with a chronic inflammatory response that is less intense than in BCC [1, 13].
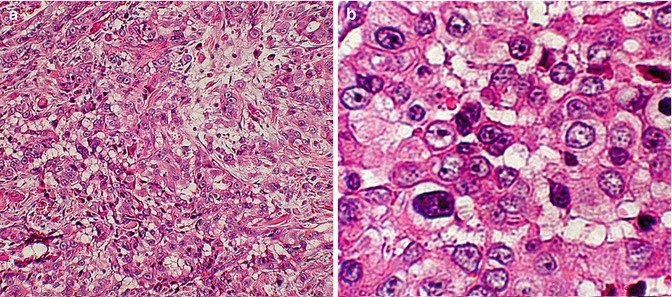
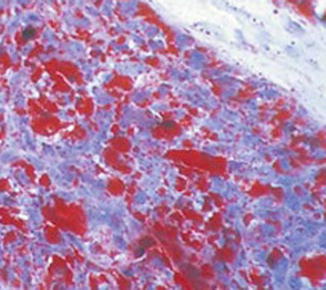
Fig. 6.3
Histopathologically sebaceous gland carcinoma is an unencapsulated infiltrating mass (a, hematoxylin–eosin ×100). The tumor is composed of cells with finely vacuolated, frothy cytoplasm and pronounced nuclear pleomorphism (b, hematoxylin–eosin ×400)
Fig. 6.4
Accentuation of the lipid using oil red-O stain. The lipid globules have a red color (Frozen section, oil red-O ×250)
6.6.3 Pagetoid Spread
6.6.4 Immunohistochemistry
The histopathologic diagnosis of SGC can usually be made readily on routine light microscopy. However, immunohistochemistry replaces the need for fat stains on frozen sections and may help to differentiate SGC from basal and squamous cell carcinoma. The central foamy cells of SGC express human milk fat globulin-1 (HMFG1) and epithelial membrane antigen (EMA), but not cytokeratins, whereas the small peripheral basal and duct cells generally express cytokeratin but not HMFG1 or EMA. SGC also expresses Cam 5.2 and BRST-1, whereas BCC expresses neither EMA nor BRST-1, and SCC expresses EMA but not Cam 5.2 (Table 6.1) [1, 14]. Androgen receptor reactivity (AR) was also found as a sensitive marker for SEB, especially in less differentiated tumors. Along with other markers and morphologic features, AR can be helpful in the diagnosis of SEB and its differentiation from SCC and BCC [15].
Table 6.1
Immunohistochemistry profile of common malignant eyelid tumors
Tumor antibody | Tumor type (% positive cases) | ||
|---|---|---|---|
Sebaceous gland carcinoma | Basal cell carcinoma | Squamous cell carcinoma | |
EMA and BRST-1 | 64 | 0 | 36 |
EMA and Cam 5.2 | 73 | 6 | 0 |
EMA and Cam 5.2 | 55 | 0 | 0 |
6.6.5 Histopathological Classification
In addition to being well, moderately, or poorly differentiated [1], SGC can be readily classified into one of four patterns: lobular, comedocarcinoma, papillary, and mixed [1].
6.6.5.1 Lobular Pattern
Lobular pattern is the most common and has architecture similar to that of a normal sebaceous gland, with fewer differentiated cells peripherally and more differentiated lipid-producing cells located centrally.
6.6.5.2 Comedocarcinoma Pattern
A large necrotic central core surrounded by viable cells characterizes the comedocarcinoma pattern.
6.6.5.3 Papillary Pattern
Papillary pattern which occurs frequently in small conjunctival lesions is distinguished by papillary projections and areas of sebaceous differentiation.
6.6.5.4 Mixed Pattern
Mixed pattern exhibits any combination of these three patterns.
6.7 Diagnostic Evaluation
Full-thickness excisional or incisional biopsy of the eyelid is the preferred method of confirming the suspected clinical diagnosis of SGC. When diffuse involvement of eyelid and conjunctiva is suspected, multiple conjunctival map biopsies should be performed to determine the extent of the disease [1, 7]. Fine-needle aspiration biopsy and impression cytology have been used in the early diagnosis of SGC [16, 17] and to detect conjunctival spread, but these methods are generally not advisable because of the limited amount of tissue obtained. However, fine-needle biopsy may be acceptable for the diagnosis of regional lymph node metastases [1]. Only in cases with suspected diffuse involvement of the eyelid and conjunctiva is orbital imaging indicated, either before or after the initial biopsy, to rule out posterior extension [1].
6.8 Differential Diagnosis
SGC is notorious for its variable clinical presentation and its ability to masquerade, both clinically and histopathologically, as common benign or less invasive conditions, resulting in delayed diagnosis and treatment [1, 2, 7].
6.8.1 Chalazion
In the early stages SGC of the eyelids can be very similar to chalazion. However, in contrast to SGC, chalazion generally occurs in younger individuals, is more circumscribed and painful, and is usually not associated with loss of cilia. However, recurrent chalazia, as well as chalazia in older patients, should undergo a biopsy to rule out SGC.
6.8.2 Inflammatory Conditions
Virtually any inflammatory condition of the eyelid and the conjunctiva must be included in the differential diagnosis of SGC. These include unilateral blepharitis, conjunctivitis, meibomitis, superior limbic keratoconjunctivitis, papillary conjunctivitis, cicatricial pemphigoid, conjunctival granuloma, and sarcoidosis. Thus, SGC should be suspected in every middle-aged or older patient with a diagnosis of unilateral blepharitis or other inflammatory conditions that do not respond to usual therapy [1].
6.8.3 Benign and Malignant Tumors
Several benign and malignant tumors can have a clinical appearance similar to that of SGC. These include BCC, SCC, melanoma, Merkel cell carcinoma, lymphoma, sweat gland neoplasm, junctional squamous papilloma, hereditary benign intraepithelial dyskeratosis, metastatic carcinoma, and other rare tumors [1].
6.8.3.1 Basal Cell Carcinoma
The nodular BCC is more common on the lower lid and is white rather than yellow. BCC is also more likely to become ulcerated than SGC. Although diffuse sclerosing BCC may closely simulate SGC, it very rarely exhibits diffuse invasion of the conjunctiva. Histologically, BCC typically shows peripheral palisading of nuclei and retraction artifact that are not seen in SGC.
6.8.3.2 Squamous Cell Carcinoma
SCC is more superficial and lacks a yellow color. Conjunctival intraepithelial neoplasia can be very similar to diffuse epithelial invasion by SGC, except for eyelid involvement, which is less likely to be present in SGC. Histopathologically, SCC is the lesion most often confused with SGC [7, 18, 19]. Unlike SGC, SCC cells have more abundant eosinophilic cytoplasm, lack lipid vacuoles, and demonstrate eddy formation and keratin cysts.
6.8.3.3 Melanoma
Nodular or diffuse cutaneous melanoma in the eyelid or conjunctiva can usually be distinguished from SGC by its black or brown pigmentation, but amelanotic melanoma can resemble SGC.
6.8.3.4 Other Tumors
Merkel cell carcinoma of the eyelid is distinguished by its red or red-blue color. Lymphoma of the eyelid arises from deeper layers than does SGC, and in the conjunctiva it has a characteristic “salmon patch” color. Moreover, inflammatory signs that are commonly associated with SGC are lacking in lymphoma.
6.9 Treatment
6.9.1 Surgery
The most acceptable management of periocular SGC is complete surgical removal [20]. Excisional biopsy of a small lesion is recommended even before histopathologic verification of the diagnosis [1]. Either frozen section control or Mohs’ microsurgery is usually used at the time of tumor excision, to evaluate the margins, and the resection is continued until the margins are histopathologically clear.
However, there is controversy as to which is preferable and whether either technique is better than waiting for permanent sections, because of the difficulty in diagnosing SGC in frozen sections [1, 21, 22]. It has been suggested that wide margins, of at least 5 mm, should be taken in order to prevent recurrence. Orbital exenteration is currently performed less often but is still indicated for advanced and diffuse SGC with orbital invasion in the absence of metastasis [1].
6.9.2 Cryotherapy
As the removal of wide margins is not possible in the case of conjunctival lesions, supplemental treatment by double freeze-thaw cycle cryotherapy is indicated. Combination therapy with cryotherapy, topical chemotherapy [23–25], and radiotherapy [26] can also be used in advanced cases [1].
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


