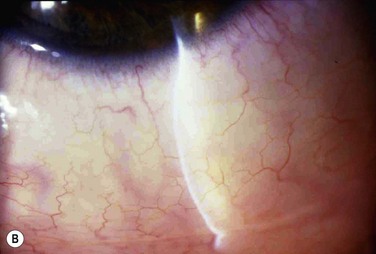
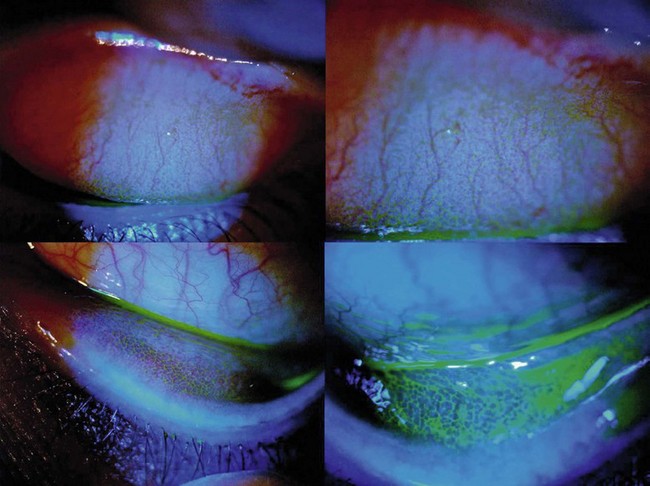
13 Seasonal allergic conjunctivitis (SAC) and perennial allergic conjunctivitis (PAC) are the common and mild acute forms of ocular allergy, usually accompanied by seasonal allergic rhinitis,1 with SAC comprising 25% to 50% of the total cases of allergic conjunctivitis.2 Several authors have emphasized that ocular allergies, especially SAC, are underdiagnosed, thus underestimating their true prevalence.3 Although SAC and PAC are relatively mild conditions, rarely causing permanent visual impairment, their effects on the quality of life can be profound, with significant morbidity.4 The seasonal incidence of SAC is closely related to the cycles of released plant-derived airborne allergens, or aeroallergens. The allergens that produce SAC vary from one geographic area to another, but tree, grass, and ragweed pollens are the most common encountered allergens. PAC is more likely to occur year-round, although about 79% of patients may still have seasonal exacerbations. Some have theorized that warming trends, accompanying long-term climate change, may cause greater exposure times to seasonal allergens, with subsequent effects on allergic eye disease prevalence.5 The majority of PAC and SAC affect both young and middle-aged people of both sexes.6 Both SAC and PAC are type I (immediate) immunoglobulin E (IgE)-mediated hypersensitivity reactions, due to environmental airborne allergens, divided into two phases, with the mast cell (MC) playing a central role. A reaction occurs when a sensitized individual is exposed to a specific antigen. IgE has a strong affinity for MCs, predominantly MCTC phenotype, triggering its degranulation. The number of MCs present within the conjunctiva stroma may be increased up to 60% in patients with SAC compared to normal patients.7 The reaction involves a very complex series of immunological events, coordinated by various mediators, initiated by the allergen. An allergen such as pollen reacts with specific IgE antibodies bound to a sensitized MC, triggering cross-linkage of the IgE molecules and an influx of calcium ions into the MC. This causes the MC to degranulate and release preformed inflammatory mediators, such as histamine, which causes the signs and symptoms associated with the early-phase response in sensitized individuals. There are two components of MC activation. The first is the release of preformed mediators, including histamine. The second is the synthesis of arachidonic acid and the subsequent metabolic cascade, resulting in the production of prostaglandins and leukotrienes. The released histamine binds H1 and H2 receptors on the target tissue cell surfaces. Binding to the H1 receptor results in the primary allergic symptoms of itching, burning, and stinging sensation and tearing, while binding to the H2 receptor releases leukotrienes and prostaglandins, stimulating mucus production and also increasing vascular permeability.7 This early-phase response is immediate and lasts clinically for 20–30 minutes. MC degranulation also initiates a series of cellular and extracellular events, which lead to the late-phase response, including production of prostaglandins, thromboxanes and leukotrienes derived from arachidonic acid.8 MCs also release cytokines and chemotactic factors which induce the production of IgE from B cells, enhance production of Th2 lymphocytes, attract eosinophils and activate vascular endothelial corneal and conjunctival cells to release chemokines and adhesion molecules. The chemokines and adhesion molecules mediate the infiltration of eosinophils, basophils, neutrophils and Th2 lymphocytes to the site of inflammation, coupled with the newly formed mediators and sustained MC activation, resulting in the late-phase response. This may occur 3–12 hours after the initial reaction, and symptoms can continue up to 24 hours.9 After the MCs are activated, cytokines are released. These cytokines attract eosinophils, lymphocytes, and neutrophils. Eosinophil infiltration of the conjunctiva is present in about 43% of patients with SAC, and about 25–84% of patients with PAC. Degranulating eosinophils release toxic proteins, including eosinophil major basic protein and eosinophil cationic protein. These proteins have cytotoxic effects and further enhance MC degranulation. These products of eosinophils are toxic to the corneal epithelium and, if present chronically, may result in ulceration. The late-phase response is characterized by an influx of multiple inflammatory cells, including eosinophils, basophils, neutrophils, and macrophages, along with CD4+ and CD8+ cells. Conjunctival epithelial cells may also prolong the allergic inflammatory response by releasing chemotactic mediators. The year-round symptoms associated with PAC are the result of chronic MC activation and Th2 lymphocyte infiltration.10,11 In summary, acute allergy is caused by IgE-mediated MC degranulation, whereas chronic allergies are also associated with continuous activation of MC but with predominance of mediators, such as eosinophils and Th2-generated cytokines.12 Individuals with SAC typically have symptoms of acute allergic conjunctivitis for a defined period of time, usually of short duration, that is, when the predominant airborne allergen is present. Typically, persons with SAC are symptom-free during the winter months in cooler climates because of the decreased airborne transmission of some allergens, such as pollen. Molds, house dust, and animal dander may also participate in the disease process. The severity of symptoms varies depending on the type of allergen, its concentration, and time of exposure.4 Dry eye facilitates allergen contact with the ocular surface since the capability of the tears to ‘wash away’ the allergen is usually compromised.13 The most significant symptom in SAC is itching. Patients usually complain of intense itching of the eyes, sometimes along with a burning sensation and tearing.14 Discharge is usually serous, clear and watery, but with a ropy characteristic. Signs in SAC include lid edema, conjunctival hyperemia and injection, and chemosis. Chemosis may be apparent in the bulbar and lower tarsal conjunctiva, giving to it a ‘milky’ or pale pink appearance. Some patients refer to a dramatic unilateral bulging of the conjunctiva, frequently described as the acute formation of a ‘bubble’ in the eye, mainly when patients rub their eyes. In reality, the conjunctiva balloons, due to intense and acute infiltration of cells and fluids, causing the chemosis (Fig. 13.1). The conjunctival chemosis can be very intense and may even cause unstable tear film and consequently corneal dellen (Fig. 13.2). These conditions tend to disappear with the resolution of the chemosis. Rarely, SAC and PAC affect the cornea, but the presence of punctate keratitis or dellen might lead to symptoms of pain, photophobia and blurred vision. SAC and PAC usually result in few to no sequelae.15 PAC is less common than SAC and, as patients are chronically exposed to allergen, symptoms and signs occur year-round. The most common triggers are mold spores, animal dander, and dust mites usually found in the household. Patients may also be sensitive to seasonal allergen with a superimposed offender to their symptoms. Symptoms and signs in PAC are similar to those in SAC but are usually milder and with longer duration. Because of the prolonged exposure, the conjunctiva may become boggy, chronically red, and irritated. Papillary hypertrophy along the tarsal conjunctival surface (Fig. 13.3) may occur with chronic exposure to allergens in PAC. The discharge is whitish but thick, and even stringy.4 The diagnosis of SAC and PAC is generally based on clinical history and careful biomicroscopic examination.16 Important features of the history include a personal or family history of atopic disease, such as allergic rhinitis, bronchial asthma, and/or atopic dermatitis. As cited earlier, patients with PAC are more likely to also have perennial rhinitis.1 Perhaps the most important symptom is itching. Without itching, the diagnosis of allergic conjunctivitis is suspect. With the intense itching, the diagnosis of SAC and PAC is very likely, but one should also consider dry eye, toxic conjunctivitis, contact dermatitis, blepharitis, and other forms of allergic conjunctivitis in the differential diagnosis.17 In these other disorders, itching is usually mild and occasional. It is worthwhile to pinpoint the location of itching. For example, patients who complain of ocular itching may be describing symptoms related to the skin of their eyelids. Careful questioning can distinguish itching of the conjunctiva from itching of the eyelid skin. Moreover, patients with dry eye tend to have mild itching located in the nasal inner part of the bulbar conjunctiva, due to allergen accumulation in the area of tear drainage.13 Superficial conjunctival scrapings may help to establish the diagnosis by revealing characteristic eosinophils (Fig. 13.4
Seasonal and Perennial Allergic Conjunctivitis
Introduction
Pathophysiology
Clinical Findings of SAC and PAC
Diagnosis of SAC and PAC
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine