Scleral Contact Lens Fitting
Corey B. Dickson
Peter R. Kastl
Scleral lens design with Poly(methyl methacrylate) PMMA was once considered antiquated and unpractical with the development of smaller lenses that allowed for better corneal metabolism. Although almost nonexistent in practices for years, there has been a steadily growing need for this lens, especially for patients with conditions affecting larger areas of the cornea, sclera, and scleral conjunctiva. In addition, the large population of failed rigid lens fits due to poor comfort, fit, or visual outcome are prime candidates for this lens design. It was not until the development of new lens materials allowing high oxygen permeability that scleral lenses would be accepted.1,2,3,4,5,6,7,8 The nomenclature of rigid gas permeable (RGP) lenses has been covered previously and will not be revisited in this chapter; however, most terminology for RGPs also applies to scleral contact lenses. There will be an attempt to explain the terminology of scleral lenses in this section, and it is the authors’ intent to give practical fitting information and guidance for successful fitting. Upon the completion and studying of this section, the reader should be able to analyze and fit scleral contact lenses.
TERMINOLOGy
The most confusing part of scleral lens fitting is in the terminology. Anywhere in the world the reader might find practitioners defining the same basic lens design in various ways. Some identify various lens types by its overall chord diameter (Fig. 54A.1). For example, a scleral lens with a chord diameter of 12.5 to 15.0 mm might be called a “semi-scleral.” A lens with diameters of 15 to 18 mm may be named “miniscleral,” and lenses with diameters 18 to 24 mm “large” or “full-sclerals.”2,3,4 These semantics are confusing and offer little understanding to the fitting process. It is the authors’ opinion that when dealing with any contact lenses, including scleral lenses, a name should identify a fitting relationship: a corneal lens is a lens that fits and rests solely on the cornea, and semi-scleral or corneoscleral lenses are those that share a relationship between the cornea and the sclera, and a scleral lens is one that rests solely on the sclera with no corneal interaction (Fig. 54A.2). Basically, a scleral lens, whether mini, large, or full, is a lens whose haptic rests entirely upon the sclera (scleral conjunctiva).1,2,3,4,5,6,7,8 When describing scleral lenses, the term haptic as mentioned may or may not be used when describing the part of the lens that makes contact with the eye. Do not let this cause confusion with the haptics of intraocular lenses (IOLs). Remember that the true definition of a haptic in optics is the load bearing part of the lens or the part of the lens that makes contact with the eye. This is the main reason that the early name for a scleral lens was also a haptic lens. Haptic, therefore, is not a term solely for the description of IOLs. Aside from being able to identify a lens based on its fitting relationship to the eye, all rigid lens terminology as previously discussed applies to scleral lenses.
When describing and analyzing the fit of a scleral lens, the fitter must pay close attention to three “zones.”2,5 These are called the corneal, limbal, and scleral zones (Fig. 54A.3). The corneal zone contains the optical zone (OZ) of the lens. This part of the scleral lens gives the desired optical correction while the back surface, theoretically, has a mirror image shape of the front of the cornea. The limbal zone makes the transition or bridge from the corneal zone to the scleral zone (haptic). It serves two main purposes: it vaults the limbus and sets the sagittal depth of the lens.2,5 The scleral zone, as previously mentioned, is the part of the lens that actually makes contact with the eye and supports the weight of the lens. When analyzing a fit, the fitter must pay attention to each zone, from the center to the edge (corneal zone to scleral zone), before making any changes in the lens design.
 FIG. 54A.1 Chord diameter is the total diameter measured from lens edge to lens edge. |
 FIG. 54A.2 Notice the haptic gently rests on the sclera and supports the weight of the lens. |
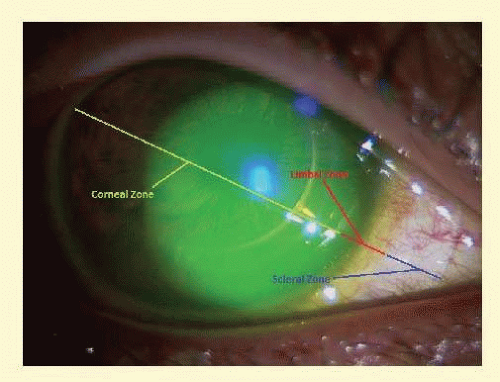 FIG. 54A.3 Although not clearly marked by the lens, the three fitting zones can be determined by the underlying anatomy of the eye. |
INDICATIONS
Many of the same indications for fitting a rigid corneal lens on an eye apply to scleral lenses. Scleral lenses will usually be indicated when corneal lenses fail in fit, comfort, or vision. Other indications of scleral lenses include intermittent wearing schedules, exposure problems, or eyes that will benefit from minimal cornea/lens interaction. This lens modality is quite impressive because of its ability to accommodate a wide array of problems including advanced keratoconus, advanced pellucid marginal degeneration, basement membrane dystrophies, severe dry eye, and neurotrophic corneas.1,2,3,4,5,6,7,8 The only eye onto which a scleral lens cannot be fit is one with a bleb, glaucoma valve, or highly irregular sclera/scleral conjunctiva. Another less common indication for scleral lenses is sporting activities. Because of the large size of the lens, the edges will usually stay tucked under the palpebral fissures, preventing the lens from falling out, making this option ideal for someone involved in high-impact sports (Fig. 54A.4).
OCULAR SURFACE ANATOMy AND SCLERAL LENSES: BASIC CONCEPTS
Appropriate scleral lens fitting will be achieved with a good understanding of some basic ocular anatomy. We know from various texts that the insertion of eye muscles occurs at about 6 to 7 mm on average from the limbus. Nasally, however, the insertion is about 5 mm from the limbus.2,6 As the average cornea is roughly 12 mm in diameter, one can conclude that the largest successful scleral lens will be about 22 to 24 mm in chord diameter without interfering with the nasal area of muscle insertion. The reason for avoiding interference of this area is that the medial rectus muscle loosens from the eye with medial movement.2,6 Having a contact lens present at this junction can cause restriction of eye movement and even cause the lens to lift off the eye. This can be problematic because comfort will be reduced, and the tendency for trapping bubbles under the lens will be greatly increased. The authors find lenses with chord diameters of 15 to 18 mm to be very effective at achieving most fitting goals, including exposure issues. Therefore, one should be cautious before approaching diameters of over 20 mm.
 FIG. 54A.4 Notice that exposing the lens edge is possible only by pulling the lids away from the eye. |
Another thing to consider is the type of tissue that a scleral lens actually interacts with. When fitting the lens, remember that the lens is resting on bulbar conjunctiva. This vascular tissue is made up of coarse collagen fibers and is loose and transparent. The shape of the bulbar conjunctiva will take the shape of the sclera, but remember that the thickness and laxity of this tissue can vary greatly between patients.2 How this affects the fit of the scleral lens will be discussed later in this section.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


