Sarcoidosis
Robert S. Weinberg
Sarcoidosis is a systemic granulomatous disease of undetermined etiology and pathogenesis.1 The diagnosis is established by a compatible clinical picture, together with laboratory or biopsy confirmation of the noncaseating granuloma, the pathologic hallmark of the disease. To the ophthalmologist, sarcoidosis must be considered in the differential diagnosis of almost any type of ocular inflammation, because sarcoidosis may affect any part of the eye or ocular adnexa. Because this systemic disease may present with ocular abnormalities, and because the ophthalmologist may be the first physician to suspect the presence of sarcoidosis, the ophthalmologist must be familiar with the general aspects of the disease.
Epidemiology
Sarcoidosis has a worldwide distribution, affecting all ages and races and both genders. Estimates of prevalence of the disease, all patients with the disease at a given time period, range from 1 to 40 per 100,000 population.2 Because some patients may be asymptomatic, prevalence data may be difficult to confirm. In the United States, the ACCESS study (A Case-Control Etiologic Study of Sarcoidosis) investigated the epidemiology of sarcoidosis.3 The incidence of sarcoidosis, the number of new cases in a given time period, is approximately three times higher in blacks (35 per 100,000) than in whites.4 The disease appears to be more common in Scandinavia and in Ireland than in other parts of the world.5 Women appear to have a slightly higher incidence of sarcoidosis.6 The disease affects all age groups but is rare in children, more common in adults under 40, and may occur in families.3,7
Etiology
The cause of sarcoidosis remains unknown. Many pathogenetic theories have been proposed including exposure to environmental stimuli, such as clay, metal dusts, or pine pollen; infection with various organisms, including Propionibacterium acnes, atypical mycobacteria, fungi, and viruses; autoimmunity; and a genetic predisposition to the development of the disease. A mycobacterial protein Mycobacterium tuberculosis catalase–peroxidase (mKatG) has been found in granulomatous tissue of some patients with sarcoidosis and may be a tissue antigen important in the molecular mechanisms involved in the pathogenesis of some cases of sarcoidosis.8 The response to antigen exposure with acquired cellular immunity against the antigen, and a nonspecific inflammatory response mediated by immune effector cells, leads to the development of the sarcoid granuloma. Activation of CD4+ T cells from interaction with antigen-presenting cells results in secretion of interferon γ, interleukin-2, and TNF-α production, with amplification of the cellular immune response.9,10 Finding the antigen or antigens that trigger the response is the first step in clarifying the etiology. Although no infectious agent has been proven, the demonstration of mycobacterial DNA in some sarcoid granulomas and of propionibacteria DNA and RNA in other sarcoid granulomas in a few patients suggests possible antigens.8,11,12
Genetics of Sarcoidosis
A genetic predisposition to sarcoidosis has been suspected, as there is an increased incidence of sarcoidosis in relatives of patients with the disease.13 HLA class II antigens, HLA-DQB1 and -DRB1, have been found in some patients with sarcoidosis.14,15 There may be specific susceptibilities by population group, as genome scans have demonstrated linkage signals on different specific chromosomes in differing population groups.16,17
Systemic Sarcoidosis
Multisystem granuloma formation is the characteristic disease process in sarcoidosis. Assessment of disease activity in sarcoidosis is difficult because the disease may be asymptomatic, persist without progression, and may not require treatment. Sarcoidosis may be a transient illness in many patients, but it can be a chronic disabling or fatal problem in others, particularly in African Americans.18 The clinician ought to remember that sarcoidosis is multisystemic and that intensity of inflammatory reaction in one organ does not necessarily imply general or systemic involvement. The lungs are most frequently affected, with pulmonary involvement in approximately 90% of patients.19 Pulmonary manifestations range from asymptomatic hilar adenopathy detected on routine chest radiograph to pulmonary fibrosis (Table 44.1). Up to 80% of patients with type 0 or I disease may improve spontaneously.19 Symptomatic extrapulmonary sarcoidosis occurs in the skin and in the lymphatic system in approximately 25% of patients and in the heart, liver, spleen, joints, bone, and nervous system in less than 10% of patients.2,7,19 Estimates of the incidence of ocular involvement ranges from 25% to 80% of patients with sarcoidosis.2,7,19,20
Table 44.1 Clinical Staging of Pulmonary Sarcoidosis Based on Chest Radiography at Time of Presentation | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
Ocular Sarcoidosis
Uveitis is the most common and most serious form of intraocular involvement in sarcoidosis. However, any part of the globe or ocular adnexa may be involved. The skin of the lids may have sarcoid nodules, which are accessible to biopsy. Conjunctival sarcoidosis appears as discrete yellowish nodules, usually smaller than 2 mm in diameter. (Fig. 44.1A). Although these nodules usually occur in the fornices or on the tarsal conjunctiva, they may also be present on the bulbar conjunctiva or on the conjunctiva overlying the lacrimal gland. If conjunctival nodules are present, they are easily biopsied (Fig. 44.1B). Conjunctival biopsy can be done at the slitlamp biomicroscope using only topical anesthesia. Blind conjunctival biopsy, that is, biopsy of an area of conjunctiva where no nodules are visible, is less likely to yield helpful information than is excisional biopsy of a visible nodule.
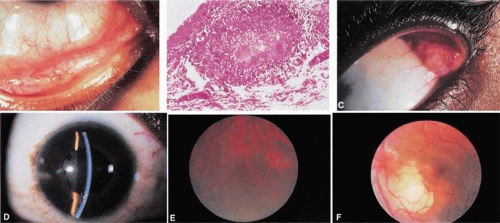 Figure 44.1. A. Conjunctival nodules in sarcoidosis. This 36-year-old black woman has yellow gelatinous conjunctival nodules characteristic of sarcoidosis. B. Biopsy of conjunctival nodules demonstrating giant cell and noncaseating granuloma compatible with a diagnosis of sarcoidosis. C. Enlarged prolapsable lacrimal gland in a 23-year-old black woman with sarcoidosis. With the patient looking down and to the right, the upper lid is retracted manually, thus allowing the lacrimal gland to prolapse. The glandular tissue itself has a nodular consistency. D. A 24-year-old black woman with sarcoid uveitis. There are medium and small keratic precipitates, anterior chamber reaction, and posterior synechiae. E. Peripheral so-called candlewax dripping in sarcoid uveitis. Yellow-white lesions are seen in the midperiphery of the fundus. These lesions are characteristic of sarcoidosis. F. Solitary choroidal granuloma in a black man with biopsy-proven systemic sarcoidosis.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|