Mucoepidermoid Carcinoma
Mucoepidermoid carcinoma is the most common malignant neoplasm of the salivary glands. It presents most frequently in the parotid gland, for which it is the most common malignant tumor. It is the second most common malignant tumor of the submandibular gland. Mucoepidermoid carcinoma constitutes approximately 30% to 35% of all malignant tumors of the salivary glands (
19,
20). This is a cancer that usually occurs between the third and sixth decades of life with a slight predominance in women.
Mucoepidermoid carcinomas are usually classified as low-grade or high-grade tumors. However, some pathologists also include an intermediate grade. Low-grade tumors have a higher proportion of mucous cells to epidermoid cells. These lesions behave more like benign neoplasms but in rare cases are capable of local invasion and metastasis. High-grade tumors have a higher proportion of epidermoid cells and may be difficult to differentiate from squamous cell carcinoma. High-grade lesions are aggressive tumors with a high propensity for metastasis. Intermediate-grade lesions have been found to behave like high-grade tumors. Thus, the grade and stage of these neoplasms are important prognostic variables (
21).
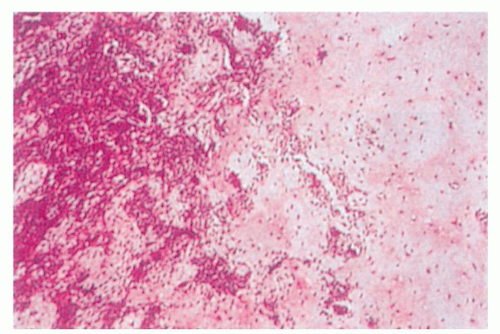
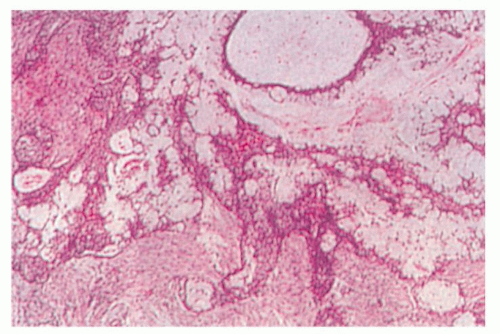
Low-grade tumors are usually small and partially encapsulated. High-grade neoplasms are usually larger and locally invasive. On cut sections, low-grade mucoepidermoid carcinoma may contain mucinous fluid, whereas high-grade tumors are typically solid. Microscopically, low-grade mucoepidermoid carcinoma demonstrates aggregates of mucoid cells separated by strands of epidermal cells (
Fig. 115.5). High-grade tumors have few mucoid elements, and the epidermoid cells predominate (
Fig. 115.6).
The treatment of this cancer depends on the grade and stage of the tumor. For small, low-grade cancers, complete surgical resection is recommended. Elective treatment of the neck is not recommended for in the clinically N0 neck because of the incidence of occult nodal involvement is very low (
21). If the surgical margins are clear and there are no adverse pathologic features, adjuvant radiation therapy is not recommended. Prognosis for this cancer is excellent with locoregional recurrence rates of 10% and 5-year overall survival of 97% (
22).
For high-grade tumors, the treatment is tailored to the extent of the disease. As in low-grade disease, complete surgical resection of the primary site is recommended. If the tumor involves the parotid gland, the facial nerve is spared, if possible. Cervical nodal metastases are managed by a comprehensive neck dissection at the time of the resection of the primary. Occult metastases rates have been shown to be approximately 21%; therefore, an elective neck dissection can be considered in a patient with a clinically N0
neck (
22). In most cases of high-grade mucoepidermoid carcinoma, adjuvant radiation therapy is recommended to improve locoregional control (
23). High-grade mucoepidermoid carcinoma is an aggressive tumor with a poorer prognosis than the low-grade variant. Locoregional recurrence has been shown to occur 43.5% of the time with 3-year disease-free survival reported to be 55% and 5-year disease-free survival at 30% (
21,
24).
Adenoid Cystic Carcinoma
Adenoid cystic carcinoma accounts for approximately 10% of all salivary gland neoplasms. It is the second most common malignancy of the parotid gland but is the most common malignancy of the submandibular and minor salivary glands (
25). Adenoid cystic carcinoma occurs with equal frequency in men and women, usually in the fifth decade of life. Facial paralysis and pain occur as initial symptoms in a small proportion of patients.
Adenoid cystic carcinoma has a contradictory clinical course. The tumor is slow growing, but its clinical course is relentless. Multiple local recurrences can occur despite adequate surgical intervention, and although regional metastatic spread is uncommon, distant spread, especially to the lungs, is common.
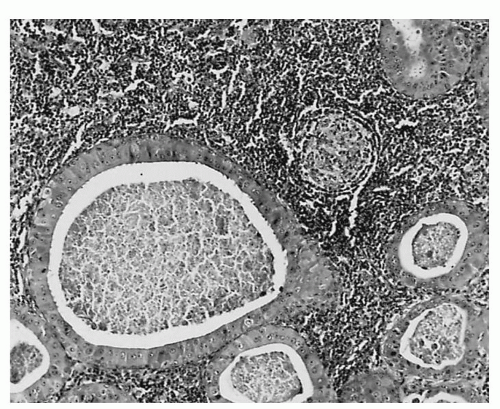
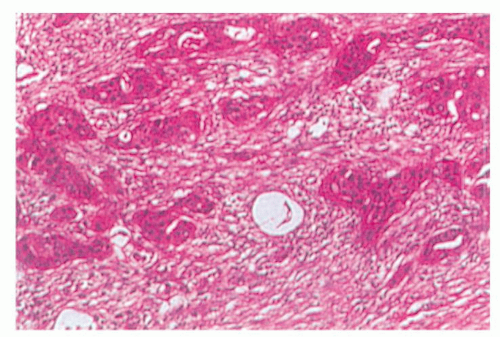
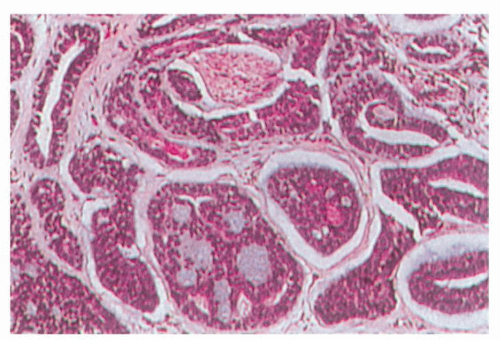
Grossly, the tumor is usually monolobular and either nonencapsulated or partially encapsulated. The mass often demonstrates infiltration of surrounding normal tissue. Microscopically, adenoid cystic carcinoma has a basaloid epithelium arranged in cylindric formations in an eosinophilic hyaline stroma (
Fig. 115.7). Different histologic patterns have been identified including cribriform, solid, and tubular. The solid histologic pattern appears to have a worse prognosis in terms of distant metastases and long-term survival (
26).
Perineural invasion is a typical feature of adenoid cystic carcinoma. This explains the difficulty in tumor eradication despite the appearance of complete tumor removal. Complete surgical excision and postoperative radiation therapy is recommended for the management of this tumor (
27). For select small tumors that are completely excised, however, postoperative radiation therapy may not be needed (
28).
There is evidence that fast neutron radiotherapy may be more effective than conventional photon radiation therapy as primary therapy for select adenoid cystic carcinomas that are not amenable to surgery (
29,
30).
Long-term follow-up is mandatory for these patients because of the slow, relentless disease progression. Recurrences have been shown to occur at an average of 63 months from the time of initial treatment (
31). Thus, 5-year survival is not adequate to detail the outcomes of this malignancy. Ten-year overall survival has been reported to be from 55% to 64%. Recurrence rates can be broken down as 42% with distant metastases only, 39% with locoregional recurrences only, and 19% with both locoregional and distant disease (
27,
31).
Because of the low incidence of occult metastases, elective neck dissection for the N0 neck is not usually performed. However, the presence of nodal metastases at the time of diagnosis is an important prognostic factor because overall survival is significantly lowered when metastases are present (
31).
Acinic Cell Carcinoma
Acinic cell carcinoma constitutes approximately 17% of all salivary gland cancers. Up to 98% of these occur in the parotid gland. It affects women more often than men and occurs in the fourth to sixth decade of life. The tumor can be multicentric in 2% to 5% of cases, and it can involve both parotid glands (
32,
33).
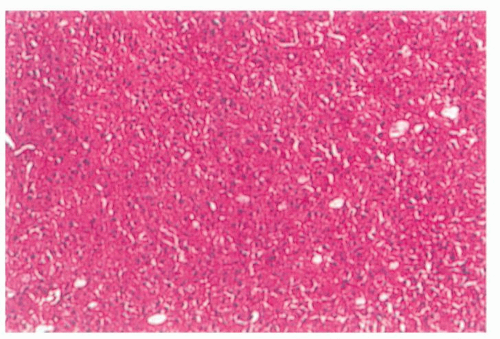
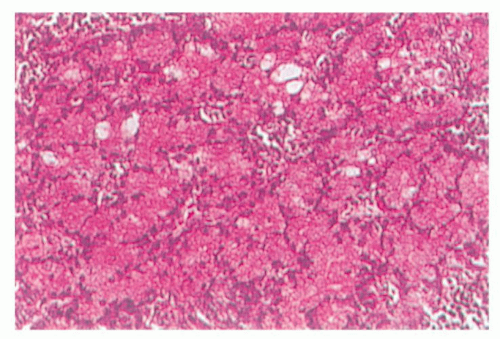
Grossly, this well-circumscribed tumor often has a fibrous capsule. There are two populations of cells: those resembling serous acinar cells of the salivary gland and those with a clear cytoplasm. Tumors occur in several configurations, including cystic, papillary, vacuolated, or follicular. There is often a lymphoid infiltrate, and cells are characteristically positive on periodic acid-Schiff staining (
Fig. 115.8).
Treatment consists of complete surgical resection with adjuvant radiotherapy reserved for indicators of a poor prognosis (e.g., facial nerve involvement, neck metastases, and skin involvement). Elective treatment of the neck is indicated for high-grade cases of acinic cell carcinoma (
32). Although acinic cell carcinoma is typically categorized as an indolent, slow-growing tumor, the average rate of recurrence has been found to be about 35% (
32,
33). Long term follow-up is mandatory because late local recurrences have been shown to occur many years after initial treatment. For low-grade lesions, 5- and 10-year disease-free survivals have been reported to be approximately 91% and 88%, respectively (
34). Five-year overall survival for high-grade acinic cell carcinoma is much poorer at 33% (
33).
Adenocarcinoma
Adenocarcinoma most commonly occurs in the minor salivary glands followed by the parotid gland. This neoplasm represents approximately 12% of malignant parotid neoplasms (
35). Adenocarcinomas occur equally in both sexes and usually present as a palpable mass. They behave aggressively with a strong propensity to recur and metastasize.
Grossly, adenocarcinoma is firm or hard and attached to the surrounding tissue. Microscopically, the cylindric cells of variable height form papillae, acini, or solid masses. Most neoplasms produce mucus, which can be detected by mucicarmine stain. Adenocarcinoma can be differentiated from mucoepidermoid carcinoma by the lack of keratin staining. The degree of glandular formation has been used as a means of grading these tumors.
Complete surgical resection with postoperative radiation therapy is the recommended treatment for this highgrade malignancy. Five- and ten-year overall survivals are 52% and 36%, respectively (
36).
Polymorphous Low-Grade Adenocarcinoma
Polymorphous low-grade adenocarcinoma (PLGA) occurs almost exclusively in the minor salivary glands. The neoplasm most commonly occurs in the palate, buccal mucosa, and the upper lip. Women are affected more commonly than men, and most of these neoplasms occur in the sixth decade of life. The typical presentation of this tumor is of a long-standing, asymptomatic mass on the palate (
37).
Histologically, PLGA demonstrates a variable tumor cell differentiation and organization. Mitotic figures and necrosis are unusual features. Tumors typically have an infiltrative growth pattern with frequent perineural invasion. Typical histologic patterns include solid, trabecular, glandular, cribriform, fascicular, cord-like, and papillary. Because of this, careful pathologic diagnosis is mandatory as this neoplasm can be mistaken for pleomorphic adenoma or adenoid cystic carcinoma. Immunohistochemical staining has not been helpful in differentiating adenoid cystic carcinoma from polymorphous low-grade adenocarcinoma (
38).
Treatment is wide local surgical excision. Cervical metastases are very uncommon, so a neck dissection is performed only for clinically positive nodes. In a recent review of the three largest series on PLGA, it was found that local recurrences occur anywhere from 10% to 33% of the time. These recurrences can occur up to 15 years after treatment. Even with recurrences, death from tumor progression is rare (
39). In general, adjuvant radiotherapy is not recommended for this cancer (
40).
Carcinoma Ex Pleomorphic Adenoma
Carcinoma ex pleomorphic adenoma represents a malignant tumor that has risen from a preexisting or recurrent pleomorphic adenoma. The malignant component and metastases from this tumor are purely epithelial in origin. This malignancy represents 2% to 5% of all salivary gland tumors. Rarely, the malignancy can take the form in which the tumor contains both mesenchymal and epithelial components.