Rheumatology
Alex V. Levin
Thomas W. Wilson
David Rootman
Rheumatologic diseases include the collagen vascular disorder, systemic vasculitides, and other related disorders. These diseases often have an immunologic pathophysiology. Arthritis may or may not be a key feature. The most commonly involved ocular tissue in rheumatologic diseases is the uvea: the iris, ciliary body, and choroid. Manifestations include any combination of anterior uveitis, posterior uveitis, vitreitis, paras planitis (intermediate uveitis), papillitis, or panuveitis. Complications from chronic uveitis include glaucoma, cataract, band keratopathy, and cystoid macular edema. Significant visual loss and amblyopia are common in undertreated patients and those with chronic ocular involvement. Treatments of systemic rheumatoid diseases will often have toxic effects on the ocular tissues. Systemic steroids may cause posterior subcapsular cataracts and steroid-induced glaucoma. Hydroxychloroquine may cause retinal toxicity with long-term use.
The ophthalmologist plays several roles in the care of children with rheumatologic disease. Some disorders, such as juvenile idiopathic arthritis, require periodic screening to detect the first signs of ocular involvement. Other patients with chronic rheumatologic disease will present to their rheumatologist or pediatrician with an ocular complaint that prompts referral to the ophthalmologist. Lastly, the ophthalmologist may make a diagnosis of an ocular manifestation of an underlying rheumatologic disorder that has not yet been diagnosed. The classic example is the onset of iritis prior to the development of the joint manifestations of juvenile idiopathic arthritis, a sequence that occurs in approximately 10% of affected patients.
Collaboration between the pediatrician or rheumatologist and the ophthalmologist is essential for the management of ocular manifestations of rheumatologic disease. In addition to the diagnostic collaboration, the nonophthalmologist is often the key physician in the management of systemic medications such as prednisone, methotrexate, antitumor necrosis factor agents, or other immunosuppressants. Likewise, the ophthalmologist often provides the screening that is required to ensure that patients do not develop systemic side effects of these medications.
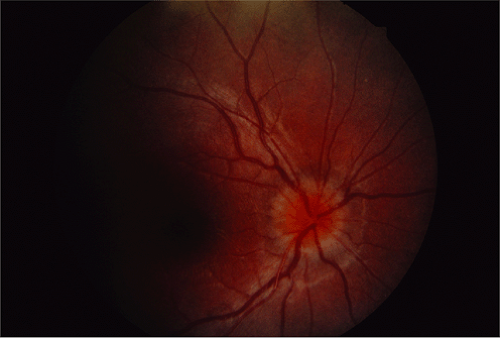 Figure 27.1 Juvenile Idiopathic Arthritis—Papillitis Juvenile idiopathic arthritis (also known as juvenile rheumatoid arthritis or juvenile chronic arthritis) is the most common rheumatologic disease of childhood and the most common identifiable cause of iritis. The iritis is usually granulomatous and the response to steroids may be variable. The iritis may be a single acute event, recurrent, or chronic. Pauciarticular and polyarticular forms occur with some patients starting as the former and evolving into the latter. At younger ages, antinuclear antibody–positive, rheumatoid factor–negative, pauciarticular girls are more commonly affected. There is no correlation between severity or activity of the joint and eye disease. Although an uncommon manifestation, this photograph shows papillitis with hyperemia and swelling of the optic nerve, which portends a poor visual outcome. |
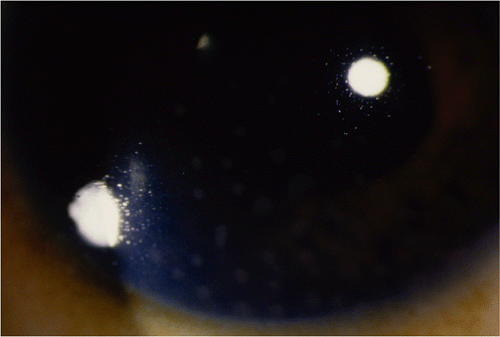 Figure 27.2 Juvenile Idiopathic Arthritis—Granulomatous Uveitis Approximately 20% of patients with juvenile rheumatoid arthritis will develop anterior uveitis. The severity of uveitis can range from mild anterior chamber reaction to severe chronic uveitis. Granulomatous uveitis with “mutton fat” keratoprecipitates is an uncommon presentation. Even hypopyon may rarely be seen as well as vitritis, pars planitis (Fig. 27.17), or panuveitis. Initial treatment would include high-dose topical prednisolone and a mydriatic agent. Following the resolution of the uveitis, the steroids should be tapered slowly over several weeks or months as tolerated. Adjunct interventions may be required including sub-Tenon depot steroid injections, methotrexate, antitissue necrosis factor agents, or, less commonly, immunosuppressive agents such as cyclosporine or azathioprine. |
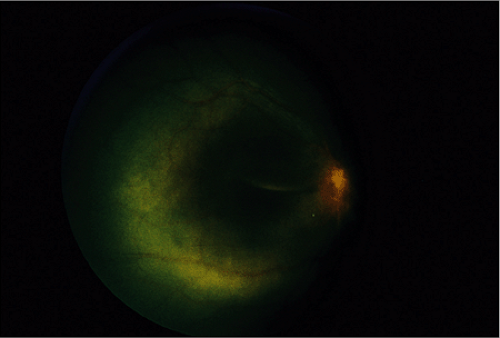 Figure 27.3 Juvenile Idiopathic Arthritis—Serous Retinal Detachment The serious retinal detachment in this photograph is an uncommon manifestation of juvenile rheumatoid arthritis. It is usually confined to those cases with severe chronic uveitis and often optic nerve involvement as well. There is often an overlying vitritis. With aggressive treatment of the uveitis and vitritis, the detachment may settle although the visual prognosis is very guarded, particularly if cystoid macular edema has occurred. |
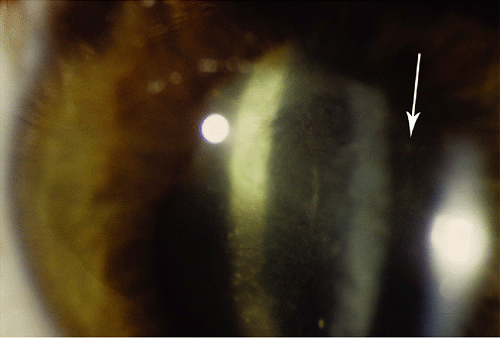 Figure 27.4 Juvenile Idiopathic Arthritis—Vitritis Decreased vision in juvenile rheumatoid arthritis can be secondary to amblyopia, cataract, vitreitis, band keratopathy, cystoid macular edema, and glaucoma. This photograph shows significant vitreous involvement (arrow), an uncommon but significant ocular complication indicating the need for medical interventions beyond topical therapy. Cystoid macular edema and posterior subcapsular cataract are likely to form in this setting. Note also the posterior synechiae and early cataract, which characterize this disorder. |
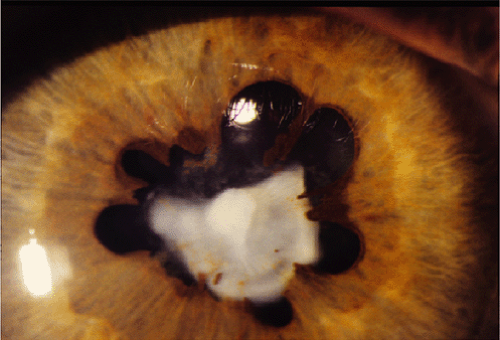 Figure 27.5 Juvenile Idiopathic Arthritis—Cataract This image is the most common appearance of chronic complicated anterior uveitis due to juvenile idiopathic uveitis. Note the severe posterior synechia and total white cataract. Significant synechia formation can lead to iris bombe (Fig. 27.6) with secondary glaucoma. The cataract may have started as the typical posterior subcapsular cataract, which then progresses to a total white cataract, often acutely, and sometimes with intumescence of the lens and shallowing of the anterior chamber. Phacomorphic and phacolytic glaucoma can occasionally occur. When possible, cataract surgery should be deferred until there is iritis control and a decline in visual function.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|