Rhegmatogenous Retinal Detachment
Brian P. Connolly
Carl D. Regillo
Background
Rhegmatogenous retinal detachments (RRDs) occur when fluid from the vitreous cavity passes through a retinal break into the potential space between the retinal pigment epithelium (RPE) and the neurosensory retina. Although retinal breaks are present in between 5% to 10% of the general public, the majority of them never lead to an RRD.1,2,3,4,5,6 In the general population, the estimated incidence of RRD is one in 10,000.7 In contrast, for patients who have had an RRD in one eye, the risk of RRD is estimated to be 10% or higher in the fellow eye.8,9,10
Various characteristics of retinal breaks and the remaining ocular structures influence whether they will remain asymptomatic or lead to detachment of the retina. This chapter discusses the pathogenesis of RRD and the factors that predispose to this condition. The prophylactic treatment of retinal tears and the treatment of RRD are also addressed.
Pathogenesis
Posterior Vitreous Detachment
Many retinal breaks that lead to retinal detachments are precipitated by posterior vitreous detachments (PVD). As a person ages, biochemical changes in the matrix of the vitreous gel cause progressive liquefaction (syneresis) of the central vitreous.11,12,13 Liquefied cavities develop throughout the vitreous cavity and, ultimately, coalesce. In many patients, the posterior cortical vitreous develops breaks that allow liquefied vitreous to pass into the potential space between the posterior hyaloid face and the retina. Once this occurs, a partial PVD can progress rapidly to a complete PVD.11
The cortical vitreous adheres to the retinal surface at the peripheral vitreous base, the optic nerve, and along retinal vessels. This is also true at the margins of lattice degeneration. Vitreous traction at the posterior aspect of the vitreous base, areas of lattice degeneration, and along retinal vessels predisposes to retinal breaks at these locations (Fig. 27.1).14 When patients experience an acute PVD, they often describe the onset of new or increased numbers of “floaters.” These “floaters” are often shadows cast by remnants of glial tissue adherent to the posterior hyaloid face or red blood cells within the vitreous cavity.15 Up to one half of patients who experience an acute PVD note the onset of photopsias (flashes of light) in addition to the presence of floaters.16,17,18
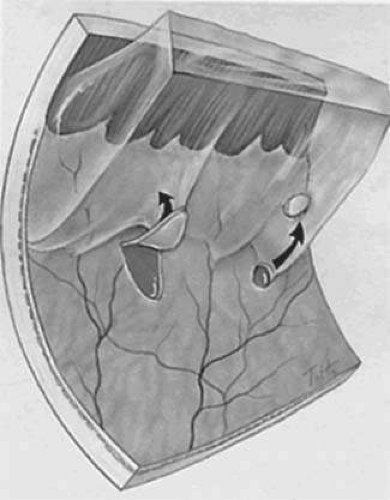 FIGURE 27.1. Vitreous traction at the posterior aspect of the vitreous base predisposes to retinal breaks at this location. Both flap tears (horseshoe tears) and operculated tears may occur. (Courtesy of Hilel Lewis and Allen Kreiger.) |
Retinal Breaks
The incidence of retinal tears following a symptomatic PVD is approximately 15%.18,19,20 Up to 20% of patients note the presence of a large number of small floaters, which usually correspond to a vitreous hemorrhage (VH).18,20 Such hemorrhages frequently result from a torn blood vessel on the surface of the retina or optic nerve. When a VH accompanies an acute PVD, the incidence or retinal tears is approximately 70%, whereas if VH is absent, only 2% to 4% of eyes have a tear.18,19,20
The presence of pigment clumps in the anterior vitreous or anterior chamber (“tobacco dust”) should also alert the clinician that the odds of finding a retinal tear are increased. This finding signifies the presence of RPE cells that have been liberated through a retinal break.
A careful retinal examination is essential when a patient presents with PVD symptoms. Indirect ophthalmoscopy with scleral depression and/or fundus biomicroscopy with a 3-mirror contact lens or other widefield contact lens should typically be performed. When a VH limits the fundus view, B-scan ultrasonography is a helpful tool that can be used to rule out a larger retinal tear or detachment. While a skilled ultrasonographer can identify (usually larger) retinal tears, a negative study does not adequately rule out a retinal tear.
Careful follow-up is suggested for such patients until the vitreous hemorrhage has cleared enough to allow a complete retinal examination. If an RRD or tear is present in the setting of dense vitreous hemorrhage, pars plana vitrectomy can be performed to allow visualization and treatment of the retinal tear or retinal detachment.
It is intriguing that only one in 70 eyes with retinal breaks goes on to develop an RRD.6,21 A number of mechanisms normally keep the retina attached. The physical interdigitation of the apical portions of the RPE cells with the photoreceptors of the neurosensory retina is one mechanism that keeps the retina attached.22 Actin contained in the cell sheaths of the RPE cells is believed to play an active role in this process.23 A second active mechanism is the removal of subretinal fluid by the RPE. There are a variety of ion channels and cotransporters involved in this process.24
Several passive mechanisms also play a role in keeping the retina attached. First, the interphotoreceptor matrix between the RPE and the neurosensory retina acts as a “biologic glue” that secures the two surfaces to one another.25 Further resistance to the development of a retinal detachment is provided by the high oncotic pressure in the protein-rich choroid that promotes the absorption of fluid from the inner ocular structures.23 Since the retina offers hydraulic resistance to the diffusion of fluid from the vitreous to the choroid, the relative pressure of the vitreous helps to hold the retina in place.26,27,28 Finally, in eyes with little vitreous liquefaction, the formed cortical vitreous impedes the flow of fluid into the subretinal space in the event of a retinal break.29
When a retinal break occurs, several factors can catalyze detachment of the retina. In particular, horseshoe-shaped tears are associated with a higher risk of RRD than other retinal breaks because the breaks are held open, facilitating the flow of fluid from the vitreous cavity into the sub retinal space (Fig. 27.2). Additionally, liquefied vitreous can pass through retinal breaks more easily than more formed vitreous, especially if the flow of the vitreous is turbulent.30 In the case of an operculated retinal tear, the traction on the surrounding retina is relieved, and the risk of subsequent RRD is minimized (Fig. 27.3).
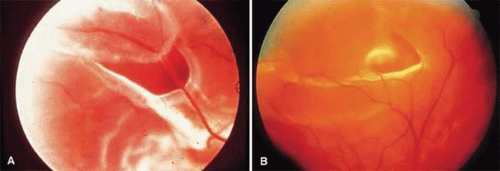 FIGURE 27.2. A. Flap (horseshoe tear) with a rolled posterior edge. Bridging vessels can be seen. (Courtesy of William E. Benson.) B. A flap tear associated with a small rhegmatogenous retinal detachment. |
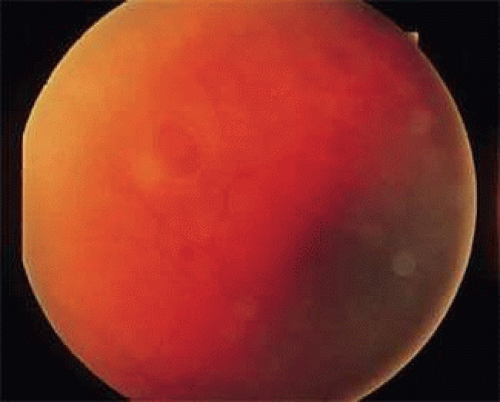 FIGURE 27.3. Operculated break with a cuff of subretinal fluid. |
Retinal Dialysis
A retinal dialysis is a tear at the junction of the neurosensory retina and the nonpigmented epithelial layer of the pars plana. While not strictly a retinal tear, a retinal dialysis allows liquefied vitreous to enter the subretinal space, causing an RRD. Retinal dialyses frequently result from blunt trauma to the globe, and they are most likely to occur inferotemporally or superonasally (Fig. 27.4).31,32,33
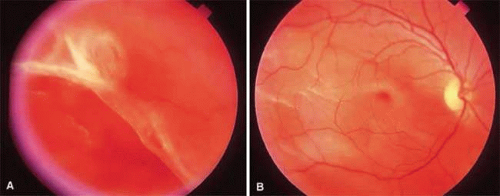 FIGURE 27.4. A. Traumatic retinal dialysis resulting from blunt trauma. B. Retinal detachment in the same eye. |
Round Holes
Retinal holes arise from atrophy of the retina, or tangentially oriented forces that create a dehiscence in the retina. Atrophic retinal holes are prone to occur in areas of lattice degeneration and in the walls of retinoschisis cavities. Atrophic holes are far less prone to cause retinal detachments than retinal tears.6,8,34
Risk Factors for Retinal Tears and Detachments
Lattice
Lattice degeneration of the retina is characterized by focal thinning of the inner retinal layers associated with liquefaction of the overlying vitreous and strong vitreous attachments to the margins (Fig. 27.5). Hyalinized blood vessels in areas of lattice often take on the characteristic lattice appearance for which this condition is named. Areas of lattice are frequently (but not exclusively) elliptical in shape and oriented parallel to the ora. These patches are often multiple and occur most often in the superior and the inferior retinal periphery.39 Some variants of lattice are oriented perpendicular to the ora, often straddling the peripheral retinal vessels—a configuration that is referred to as radial or meridional lattice.
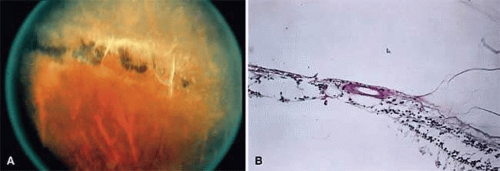 FIGURE 27.5. A. Lattice degeneration with pigmentation. Hyalinized blood vessels are seen within the lattice. B. Photomicrograph of lattice degeneration demonstrating focal thinning of the inner retinal layers and associated liquefaction of the overlying vitreous with vitreous attachments to the margins. (Courtesy of William Tasman.) |
One third of all retinal detachments are associated with lattice, although lattice is estimated to occur in only 6% to 10% of the general population.39,40,41,42,43 This condition is bilateral in one third of those affected, and it is more prevalent in myopic compared to hyperopic eyes.39,40,41,42,43 Two forms of retinal breaks are frequently associated with lattice: atrophic holes within the lattice, and flap tears at the posterior border or at the ends of the patch.
Atrophic holes occur in about one third of the patients with lattice and are frequently present in young patients. Retinal detachment is a rare complication of atrophic holes in lattice which, when it occurs, tends to progress slowly.41,44,45 Because of their relatively benign nature, treatment is rarely warranted for these atrophic holes. Horseshoe tears associated with lattice, in contrast, have a more ominous prognosis. The detached cortical vitreous generally adheres to the retinal flap and holds the tear open. These flap tears, especially when they are symptomatic, can cause rapidly progressive retinal detachments.8,34,41,46,47
Myopia
While present in only 10% or less of the general population, significant myopia is associated with 42% of all retinal detachments.40 This association of RRD among myopic eyes has been attributed to a variety of causes. The incidence of posterior vitreous detachment is higher for any given age group in people with myopia compared to those with emmetropia and hyperopia.48 Lattice degeneration is also more prevalent in myopes than in the general population.44 Finally, the peripheral retina is more vulnerable to developing retinal tears in myopic eyes.23 When symptomatic retinal tears are present in patients with moderate to high myopia, prophylactic treatment should be considered.
Cataract Extraction
Cataract extraction is an independent risk factor for RRD with an incidence of retinal detachment being increased for up to 20 years after cataract extraction.49,50 The incidence of RRD following intracapsular cataract extraction (ICCE) is greater than after extracapsular cataract (ECCE) surgery. Following uncomplicated surgery, the risk of RRD is estimated to be 2% to 5% with ICCE and about 1% with ECCE. In contrast, the incidence of RRD is between 0.01% and 0.05% in the general phakic population.7,51,52,53,54
Vitreous loss during cataract surgery increases the risk of RRD 4.5-fold to about 5%.51,55 Likewise, YAG capsulotomy increases the risk of RRD 3.9-fold.56 Other risk factors that increase the risk of RRD with cataract extraction include the following: myopia, young age, white race, prior RRD surgery, and RRD in the fellow eye. The causative retinal break is most frequently located superotemporally in phakic, pseudophakic, and aphakic retinal detachments. Nonetheless, both superonasal breaks and breaks that go undetected at the time of intervention are more common following cataract extraction.49,57,58,59,60
The tendency for pseudophakic breaks to be smaller in size and more anterior in location combined with the postsurgical changes in the anterior segment combine to make tears difficult to localize. Overall, the rate of missed breaks following cataract surgery ranges from 5% to 16% versus 2% to 5% in phakic patients.40,49,61 While careful localization of breaks is always a critical step in RRD repair, particular attention must be paid in patients who have had cataract extraction.
Blunt Trauma
Three quarters of traumatic retinal detachments occur in men largely because they are more likely than women to engage in contact sports or fighting.63,65 The leading cause of retinal detachment in children and adolescents is blunt trauma.63,65,66 Blunt trauma generally compresses the contents of the eye in an anteroposterior direction causing a compensatory expansion of the globe in an equatorial plane. Despite the elastic nature of the vitreous, rapid compression of the eye due to trauma can transmit severe traction to the vitreous base causing many types of pathology. Linear or horseshoe tears at the posterior vitreous base, tears in the nonpigmented epithelium of the pars plana at the anterior vitreous base, and retinal dialyses are the most common forms of tears that follow such trauma.63,65,67
The most common location for retinal breaks following trauma are inferotemporal and superonasal.68,69 Most traumatic retinal breaks are believed to occur at the time of impact.67,70 Because of the formed nature of the vitreous in young patients, the progression of retinal detachments following trauma tends to be relatively slow.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


