This article addresses the challenge of persistent nasal airway obstruction following septoplasty, specifically as it relates to revision septoplasty. Emphasis is on the importance of and the steps to be taken in making a complete and correct diagnosis of the problem before any surgery is performed. The authors present two categories of revision surgery: surgery involving the cartilaginous septum and surgery involving the bony septum, because they believe the evaluation and management of these areas are distinct. This article presents a discussion of airflow dynamics, options to objectively assess nasal volume and patency, examination of the septum, and surgical approaches and techniques.
Septoplasty, turbinoplasty, and nasal valve surgery are all done in an effort to improve patients’ complaints of nasal airway obstruction. Septoplasty for nasal airway obstruction is perhaps the most common of these procedures performed by otolaryngologists in their adult patient population. It can be a challenging and complex procedure to do well, as evidenced by numerous contributions to the literature of different mechanisms to correct nasal airway obstruction brought about by a deviated septum. Efforts to improve the nasal airway by manipulating the septum began with Ingalls in 1882 and Freer and Killian in 1902 and 1904, respectively. Some of the most famous names in surgery—Metzenbaum, Cottle, Goldman, Converse—and still others are credited with describing and improving septoplasty techniques. Despite advances and techniques that include closed, open, and endoscopic approaches, septoplasty is not always successful. In 2002, Dinis and Haider found by questionnaire that only 42% of septoplasty patients thought they had a good to excellent result. A moderately successful result was found in 35%; a poor to mediocre result in 23%. A study recently published by Becker and colleagues found that lack of improvement after primary septoplasty was often due to factors that affect the airway other than the septum, such as the nasal valve.
The purpose of this article is to address the challenge of persistent nasal airway obstruction following septoplasty, specifically as it relates to revision septoplasty. This article divides revision surgery into two categories: surgery involving the cartilaginous septum and surgery involving the bony septum, because the evaluation and management of these areas are distinct.
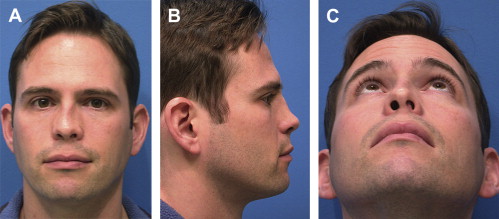
A revision septoplasty is usually spawned by the patient’s feeling that he or she is still not breathing as well as possible. Sometimes this is noticed in the first several months after surgery by the surgeon or by the patient. Usually, however, the request for a revision septoplasty occurs well over a year after the initial surgery, oftentimes following a period in which the patient had felt significant initial improvement in their nasal airway. Septoplasty may also unmask tension in the nose that then allows an unexpected change in appearance to occur long after the initial surgery ( Fig. 1 ).
When a patient complains of nasal obstruction following septoplasty, it is incumbent on the surgeon to determine whether this is a medical or surgical issue. Patients who have anatomic nasal obstruction may also have underlying inflammatory disease (allergic, infectious, or both) that is not being adequately treated. Revision surgery may not be effective, even when there are residual anatomic abnormalities, unless concomitant medical therapy is optimized ( Fig. 2 ).

Airflow dynamics are complicated, and air does not travel through the nose in a laminar pattern. Airflow generally occurs in an arc-wise fashion, with creation of turbulent, eddy currents that likely are responsible for the “sensation” of airflow. When air passes through the nasal valve (the flow-limiting anatomic region of the nasal cavity), it arcs superiorly over the anterior end of the inferior turbinate toward the head of the middle turbinate. Air passes medial and lateral to the middle turbinate and subsequently through the posterior choanae ( Fig. 3 ). Therefore, evaluation of the inferior and middle turbinates and the nasal valve is essential because these structures often are additional sources of airflow obstruction.
There are several means by which to objectively assess nasal volume and patency. Acoustic rhinometry and CT can give static measures of nasal volume, whereas anterior active rhinomanometry provides information on dynamic airflow. These techniques have been shown in some studies to correlate well with findings on physical examination, including nasal endoscopy, and can document improvement in objective measures following treatment, whether medical or surgical. One must exert caution, however, in the interpretation of cross-sectional minima with acoustic rhinometry, because these do not always correlate to specific anatomic structures. After the determination is made that anatomic nasal obstruction involving the septum exists, revision septoplasty can be considered.
In general, there are several challenges in revision septoplasty. Patients are often frustrated and want to know why the initial surgery did not work. This question is always important to answer, as is the question of what will be done differently in a subsequent procedure. Further, a more challenging dissection in compromised tissue with an unknown amount of cartilage or bone present must be done, and done in a fashion so as not to create unanticipated external changes or a subsequent perforation. The surgeon must also accept the responsibility of exposing the patient to another anesthetic along with similar risks inherent to the initial operation.
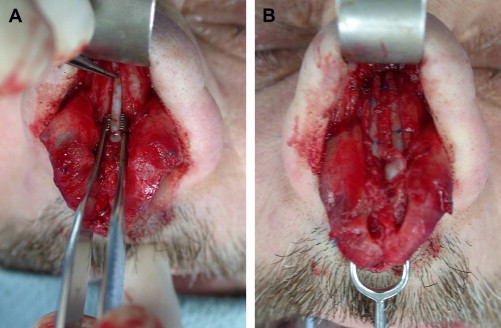
The etiology of a persistent airway blockage by the septum following an initial surgery is commonly multifactorial. Perhaps there was simply incomplete resection of the bony or cartilaginous septum that was not obvious at the time of surgery. Especially in the traumatic nose, initial resection of the septum may be adequate, but release of tension previously caused by the traumatized septum, allows another portion of the septum and possibly the external nose to reposition in a non-anatomically favorable direction ( Fig. 4 ). Of course, there is the possibility of re-injury in a nose that is less well supported due to resection of septal cartilage and bone. Tension may also be created by inappropriate or varying planes of dissection that are noted only after healing. And, certainly, the patient’s airway complaints may have initially been due to more than simply the septal deviation and, despite a successful septoplasty, airway obstruction persists. This etiology is the most common reason for patient visits to the authors’ office asking for a revision.

A common reason for an initially corrected septal deviation to “redeviate” is failure of the primary surgeon to realize that “the cartilage always wins” (Tom Wang, MD, personal communication, 1999). Multiple techniques have been fostered to change the shape of a curved piece of cartilage, including scoring, sutures, repositioning, and bolstering. Sometimes these techniques can work, but if the memory of the cartilage is not altered sufficiently, it often returns over time to its initial curvature and “wins.” Breaking this memory commonly demands a much more invasive operation, sometimes including complete autotransplantation and perhaps challenging the skill set of the general otolaryngologist.
A closer analysis of the anatomy in a revision case is imperative. One must evaluate whether the septum is still a cause of airway obstruction or a cause of a change in the external appearance of the nose. The examination must include the external nose as well as the internal nose.
Is the problem due to the bony or cartilaginous septum?
Is the caudal septum blocking the airway in the dorsal or ventral direction and causing the tip to deviate?
Is the nasal spine the culprit?
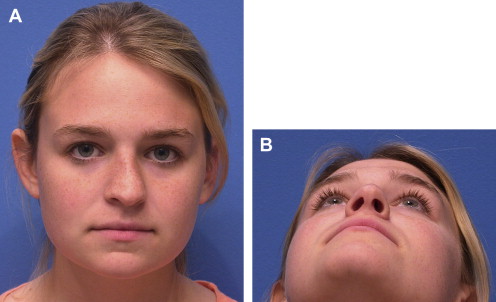
Is the patient’s face simply asymmetric congenitally, creating a difference in the nostril size or position? ( Fig. 5 )

Fig. 5
Congenital asymmetry of facial platform resulting in nasal and septal deviation.
Are there also cosmetic issues as a result of the initial septoplasty?
Has the caudal septum been removed, creating tip ptosis and excessive loss of columellar show?
Asking these questions and making a thorough examination, including an endoscopic evaluation, are necessary to determine whether a revision may be helpful. The surgeon must be assured that no other cause of obstruction such as polyps, turbinate hypertrophy, adenoids, concha bullosa, nasal valve, or congenital deformity exists. Or, perhaps, the decision must be made that a revision septoplasty is necessary in addition to other adjunct procedures.
The quadrangular cartilage can be manipulated extensively in an effort to improve the nasal airway initially or even in a revision case. The key elements involve maintaining support with attachment at the nasal spine and an adequate “L strut” caudally and dorsally. The size of the L strut can vary depending on the inherent strength of the cartilage and the weight of the nasal skin but usually needs to be 7 to 8 mm in width.
Surgical approaches to cartilaginous septal deformity
The surgical approach to revising a cartilaginous septal deformity can be performed through a “closed” incision (hemitransfixion, full transfixion, or Killian) or through a standard open rhinoplastic approach, accessing the septum between the medial crura of the lower lateral cartilages. Historically, techniques of moving the nasal spine and caudal septal resection, like that advocated by Peer and colleagues, were fairly effective at straightening the caudal septum initially. Rarely, however, were the needs of resupporting the nose accomplished, often resulting in loss of appropriate columellar show and other cosmetic deformities such as a pollybeak ( Fig. 6 ).

“Swinging Door” Technique
Another closed technique introduced by Metzenbaum is called the “swinging door,” in which a caudally deviated septum is released from the nasal spine and maxillary crest, adjustments are made to any excess of cartilage along the nasal floor, and the ventral caudal septum is “swung” to the other side of the nasal spine and sewn into place. This technique can be very effective for the ventral aspect of the caudal septum but does not change the inherent twist or bow of the septum. The nasal tip may remain deviated, and again, resupporting the nasal tip must be considered in this procedure ( Fig. 7 ).

Cartilage Scoring
Performed in conjunction with other techniques or separately, cartilage scoring is done to weaken the concave side of a septal deviation, to remove the inherent twist or bend, and to “allow” the cartilage to straighten. Scoring is done perpendicular to the orientation of deviation, often requiring light incisions into the cartilage in both directions and perhaps on both sides of the septum. This technique has found favor historically and in the literature for primary and revision septoplasty; however, rarely can the cartilage be weakened enough to straighten and still provide the necessary support for long-term favorable results.
Open Approach
Due to the limitations of the closed approaches and the generally greater complexity in revising the cartilaginous septum, the authors primarily use the open approach. Most of the revisions they see involve the caudal septum, and the authors commonly add spreader grafts ( Fig. 8 ) or make attempts to straighten the nose, which are accomplished with greater facility by the open approach. A standard inverted V transcolumellar incision ( Fig. 9 ) is made, and dissection to expose the upper and lower lateral cartilages is completed. The medial crura are retracted laterally, and dissection is carried down onto the caudal septal angle. Meticulous dissection ensues to ensure exposure of the cartilage in the submucoperichondrial plane. Access to the complete dorsal and ventral aspects of the caudal septum and nasal spine is achieved ( Fig. 10 ).


When the dorsal septum is deviated or the nose is crooked, the upper lateral cartilages are separated from the septum. The mucoperichondria of both sides are dissected to release all forces of scarring and contraction. This is a tedious dissection but gives excellent visualization and often allows simultaneous repair of perforations that may have resulted from primary septoplasty. Not infrequently, total release of the mucoperichondrium also releases external forces created by previous healing or trauma, setting “free” the crooked cartilage to straighten automatically.
This approach also gives excellent access to placing spreader grafts, batten grafts, or both to address a commonly compromised nasal valve that was not recognized initially or was caused by weakening of the septal cartilage in the initial operation.
Graduated Series of Techniques
The authors’ approach for revision of the cartilaginous septum, therefore, is generally open and follows a graduated series of techniques. Any deviated portions of the quadrangular cartilage not occupying the L strut area are removed and maintained for grafting purposes. When the L strut is mildly deviated, the concave side is scored, and a straight, reinforcing graft of harvested septal cartilage is sutured across the deviation to maintain the correction and add support. When scoring is not effective to break the cartilage’s “memory,” the deviation is divided at its maximum point of curvature and then grafted. The preferable graft is septal cartilage, but autologous rib, thin perpendicular plate of the ethmoid bone (PPE), donor rib, and Porex (Porex Corporation, Newnan, Georgia) may also be used. Porex is well tolerated so long as it is well covered, usually by adjacent cartilage, and not directly underlying skin.
Extracorporeal Septoplasty
A more common presentation for the authors is the patient who has a poorly supported nose and virtually no straight septal cartilage. In this case, extracorporeal septoplasty is advocated. This method involves removal of most of the septal cartilage after making careful measurements of the appropriate dorsal length and caudal height. A portion of the dorsal septum at the junction of the nasal bones (keystone area) is left intact to have an area to which to sew. The harvested cartilage is then carved and fashioned using sutures into an adequate L strut and introduced back into the nose, securing it to the keystone area and upper lateral cartilage. The configuration is made such that the caudal strut also functions as a columellar strut and is sewn to the nasal spine in addition to the medial crus of the lower lateral cartilage for tip support. In the last few years, the authors have found that a more efficient and effective variation of this method is to maintain the dorsal strut, even when crooked. Any deviations are effectively scored and then straightened by applying bilateral “extended” spreader grafts, which are then sewn to an “extended” columellar strut. Commonly, a tip graft is then applied to tie the support units together even further. This process nicely straightens the dorsum, addresses the nasal valve, and resupports the nose adequately ( Figs. 11–13 ).