Nasal obstruction is one of the most common complaints evaluated by the otolaryngologist. The differential diagnosis is broad, ranging from benign reversible causes to life-threatening diseases. In addition, patients may suffer from a combination of etiologies, further confusing the diagnosis. Surgical management is directed at the underlying origin of obstruction. The clinician therefore must use a careful history and physical examination as well as appropriate sinonasal imaging in accurately identifying the causes of nasal obstruction. To further illustrate these principles, we present two interesting cases of patients presenting with nasal obstruction.
Nasal obstruction is one of the most common complaints evaluated by the otolaryngologist. In addition to being an important risk factor for obstructive sleep apnea, nasal obstruction is associated with such extranasal symptoms as headache, fatigue, sleep disturbance, and daytime somnolence, and contributes to overall diminished health and quality of life. The differential diagnosis is extensive, ranging from anatomic malformation to unusual but life-threatening disease states. Patients often suffer from a combination of etiologies, further confounding the clinician’s ability to establish a diagnosis. Treatment planning therefore depends on careful history-taking; detailed physical examination, including nasal endoscopy; and the appropriate use of sinonasal imaging. Medical therapy focuses on treatment of the underlying mucosal disease, whereas surgical intervention is directed towards the areas of anatomic obstruction. In this discussion, we present two unusual cases of nasal obstruction.
Case 1: 31-year-old with nasal obstruction and epistaxis
A 31-year-old female presented with a 2-month history of nasal obstruction, swelling along the right nasal dorsum, and intermittent, self-limited epistaxis. Her sense of smell was unaltered, and there was no associated discomfort.
On physical examination, the patient was found to have fullness along the right nasal dorsum and a submucosal mass obstructing the right nasal cavity and displacing the nasal septum to the left.
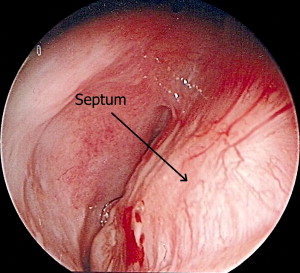
Rigid nasal endoscopy was performed, demonstrating a mass originating from the right nasal septum and abutting the right lateral nasal wall with no overt invasion.
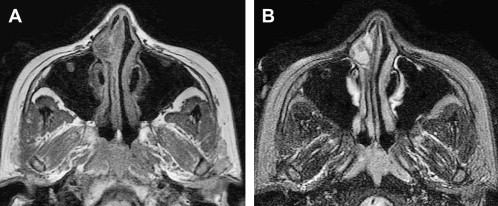
MRI revealed a well-circumscribed soft tissue mass measuring 1.0 × 0.7 cm ( Fig. 1 ). The mass originated from the right nasal septum and extended to the right lateral nasal wall with remodeling of the nasal process of the maxilla. No bone erosion was seen and the septum appeared intact.
A biopsy was obtained and it was consistent with a pleomorphic adenoma. The patient underwent an endoscopic wide local excision of the mass with resection of septal perichondrium as the deep margin. Final pathology showed that all margins were negative and the patient is without evidence of disease at 12-month follow-up ( Fig. 2 ).
Although the majority of pleomorphic adenomas are found in the major salivary glands, many examples of intranasal benign mixed tumors have been documented and described. One of the largest series to date was an analysis of more than 10,000 salivary gland tumors by Compango and Wong. In their review, 40 patients with nasal pleomorphic adenoma were identified. The vast majority of tumors (90%) originated from the nasal septum. Other sites included the lateral nasal wall and nasopharynx. The majority of tumors were noted in the third to sixth decades of life and, although these investigators did not find a disparity between male and female patients, others have reported a female predilection. Nasal obstruction and epistaxis are the most common presenting symptoms. However, nasal swelling, nasal mass, epiphora, and mucopurulent rhinorrhea may also be seen. Rhinoscopy generally shows a submucosal polypoid mass, which may bleed easily. CT often demonstrates a well-circumscribed mass with bony remodeling, whereas MRI typically exhibits a mass with low to intermediate signal intensity on T1-weighted images and high signal intensity on T2-weighted images. In contrast to those tumors that originate within major salivary glands, intranasal pleomorphic adenomas histologically exhibit increased myoepithelial cellularity with little stromal component. Recurrence rates have been reported from 2.4% to 7.5%.
Case 2: 44-year-old with unilateral nasal obstruction
A 44-year-old female presented with unilateral nasal obstruction without significant rhinorrhea. A detailed history revealed that she recently recovered from meningitis and had experienced a previous episode of meningitis several years before. There was no prior history of head and neck surgery or trauma. Her other medical history was significant for hypertension and seizures.
Physical examination demonstrated a large nasal mass lateral to the left middle turbinate extending outside the middle meatus, filling the nasal cavity ( Fig. 3 ). There was no evidence of clear rhinorrhea and the mass was not pulsatile.
An MRI showed a right lateral lamella cribriform encephalocele measuring 1 × 3 cm ( Fig. 4 ). CT evaluation showed a skull-base defect in continuation with the nasal mass ( Fig. 5 ).
The encephalocele was approached endoscopically for resection and skull-base reconstruction. The middle turbinate was medialized and the area of the frontal recess was serially dilated with Afrin-soaked neurosurgical pledgets.
Once adequate exposure was obtained, the stalk of the encephalocele was amputated with bipolar electrocautery at the level of the skull base. Several dural veins were identified entering the meningocele and cauterized with bipolar electrocautery.
The encephalocele was then removed en bloc for pathologic evaluation. At this point, the brain was noted to be herniating through a 1-cm defect in the lateral lamella of the cribiform plate. The defect was sequentially fulgurated along its inferior aspect with bipolar electrocautery to reduce the herniation into the anterior cranial fossa. Following this, the skull base surrounding the defect was denuded in preparation for grafting.
A mucosal graft was harvested from the right middle turbinate, and the mucosal surface marked with ink to ensure proper positioning over the defect. Anterior ethmoid bone was harvested, shaped, and carefully placed into position in an underlay fashion. The mucosal graft was then placed ( Fig. 6 ) and held in position with Gelfoam (Pfizer Inc., New York, New York) soaked in tissue sealant. Bioresorbable dressing was then placed to allow for additional support of the graft.



