Nasal airway obstruction is the source of significant patient discomfort and financial burden; hence, otolaryngologists encounter this symptom on an almost daily basis. This article provides a thorough yet concise summary of common and more specialized techniques that are instrumental in diagnosing nasal obstruction. The article begins with a brief overview of significant nasal anatomy and physiology. Ultimately, the main focus is on exploring the role of nasal endoscopy, radiographic imaging, acoustic rhinomanometry and other diagnostic tests that assist in the diagnosis of nasal airway obstruction.
Nasal obstruction is an important symptom of many underlying disorders and is a common cause of otolaryngology visits. Kimmelman has estimated that approximately 5 billion dollars are spent annually to relieve nasal airway obstruction, and an estimated 60 million dollars are spent on surgical procedures intended to relieve nasal airway obstruction. Patients will often use the term congestion, which may either refer to mucus secretions or obstructive nasal pathology. This article describes diagnosis of the latter.
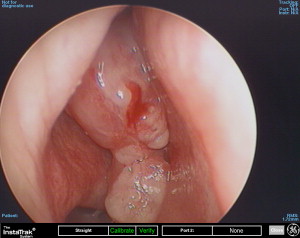
Differential diagnosis
Nasal obstruction is a symptom and not a diagnosis. The evaluation of nasal obstruction has both objective and subjective measures. Nasal patency can be quantified objectively based on the anatomy of the nasal cavity or the physiology of nasal airflow. The subjective feeling of nasal obstruction depends on additional factors such as pressure receptors, thermal receptors, pain receptors, secretions, and others. Ultimately, the etiology of nasal obstruction is polyfactorial. For this reason, the differential diagnosis of nasal obstruction ( Fig. 1 ) is broad, including physiologic and anatomic pathology. It is important to remember that patients may have a combination of these factors contributing to the symptom of nasal obstruction.
Anatomic Causes
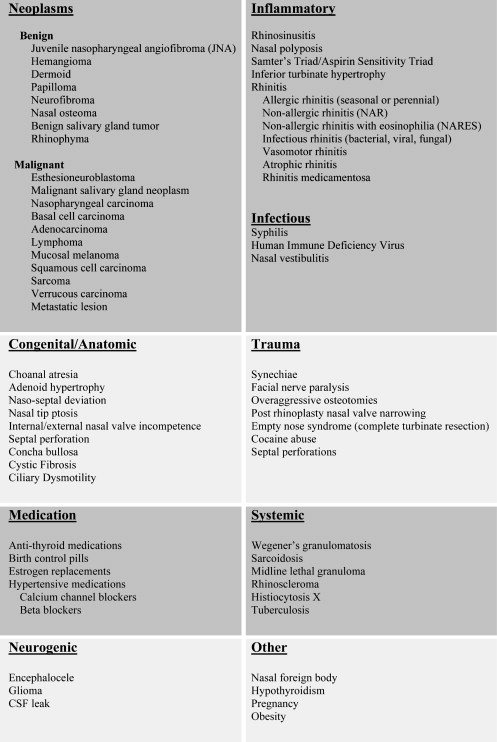
The nasal valve is described as the narrowest portion of the human airway. Anatomically, it is broken down into an internal and external nasal valve. The endonasal anatomic region of the internal nasal valve was first described by Mink in 1903. The anatomic boundaries of this internal nasal valve include the dorsal nasal septum medially, the internal caudal edge of the upper lateral cartilage laterally, and the anterior head of the inferior turbinate as the posterior boundary. Normally the angle between the nasal septum and upper lateral cartilage is 10 to 15 degrees in the leptorrhine nose, and is usually a little wider in the platyrrhine nose. This internal nasal valve, the narrowest segment of the nasal airway, has a cross-sectional area of approximately 40 to 60 mm 2 . It accounts for approximately two thirds of total nasal airway resistance, and hence, collapse or stenosis of this area is thought to be one of the most common causes of nasal obstruction ( Fig. 2 A–C ).
The boundaries of the external nasal valve, also known as the nasal vestibule, includes the caudal edge of the lateral crus of the lower lateral cartilages, the alar fibro-fatty tissue, and the membranous septum. The nasal vestibule is the first component of the nasal resistor. Studies have shown 30 L/min as the limiting flow during inspiration at which nasal airway collapse occurs in this area. It is important to differentiate between the nasal valve proper and the nasal valve area. The nasal valve area, as described by Kasperbauer and Kern, is the area extending posteriorly from the actual nasal valve to the bony pyriform aperture and extending inferiorly to the nasal floor.
On inspiration, the high velocity of air passing through the nasal valve will cause a decrease in intraluminal pressure. These Bernoulli’s forces create a vacuum effect on the upper lateral cartilages, ultimately causing collapse of the upper lateral cartilage. The resiliency of the upper and lower lateral cartilages counteract Bernoulli forces during deep inspiration and prevent internal and external nasal valve collapse. Airway collapse of the external nasal valve is prevented by activation of the dilator naris muscles during inspiration, whereas positive pressure is the driving force for nasal vestibule dilation during expiration.
Previous trauma, especially previous rhinoplasty, is the most common cause of a weakened nasal valve. The already narrowed nasal valve can further be limited as a result of a deviated nasal septum. As stated by Poiseuille’s law, airflow through the nose is proportional to the radius of the airway raised to the fourth power. As air is inhaled through the nasal cavity, airflow accelerates as it enters the nasal valve. It follows that any small deflection of the nasal septum can lead to exponential effects on nasal airflow, and hence, influences nasal obstruction.
Septal deviation has also been associated with significantly longer mucociliary clearance times than normal controls. Notably, normalization of mucociliary clearance has been observed after septoplasty. It is important to remember, however, that not every abnormality of the septum requires correction, as anterior deviations in the nasal valve region are more likely than posterior deviations to cause symptoms of obstruction.
Pneumatization of the middle turbinate, or concha bullosa, is a common anatomic variant found in approximately 25% of the population. A study reviewing 202 consecutive CT scans found pneumatization of the vertical lamella of the middle turbinate in 46.2%, of the inferior or bulbous segment in 31.2%, and the lamella and bulbous portion in 15.7% of cases. Most concha bullosae are small and asymptomatic. However, a large concha bullosa or massive bilateral concha bullosa is thought to contribute to nasal obstructive symptoms. Concha bullosa is thought to be a significant etiology of nasal middle meatal obstructive syndrome, the symptoms of which include headaches, impaired nasal breathing and anosmia. Septal deviation and middle turbinate concha bullosa often occur concurrently. Nearly 80% of patients with a dominant concha bullosa have a concurrent deviated septum. There is also a strong association between unilateral concha bullosa and contralateral septal deviation. Naturally, the influence of septal deviation and concha bullosa on the symptom of nasal obstruction will depend on several factors, including the degree of anatomic compromise and inflammatory comorbidities.
Patients with fixed anatomic obstructions may experience intermittent symptoms secondary to the nasal cycle and other autonomic phenomena. The phenomenon of the nasal cycle was studied by Lang and colleagues who measured fluctuations in nasal cross-sectional area during the nasal cycle using acoustic rhinometry. They were able to show changes in unilateral nasal cross-sectional area during the nasal cycle; however, little variation was noticed at the nasal valve itself. This may explain why the nasal cycle is often unnoticed unless other pathology exists, such as septal deviation, allergic rhinitis, and so forth. Nasal resistance is also affected by physical exertion. Physical exertion is thought to decrease nasal resistance either by sympathetic stimulation or by a simple redistribution of blood to the heart, lungs and peripheral muscles. In accordance with Ohm’s Law, a decrease in nasal airway resistance requires less work to produce the same amount of flow, which is beneficial during times of physical exertion. This may also account for episodic symptomatic improvement in patients with fixed obstructive pathologies.
Many anatomic causes of nasal obstruction can be understood in the context of measures used to correct or compensate for the abnormal anatomy. The site of anatomic compromise can also be gleaned from the effect of nonsurgical maneuvers. For example, Portugal and colleagues demonstrated a reduction in nasal airway resistance with external nasal dilators (also referred to as the Breathe-Right device), with better results in the Caucasian nose. The study was limited to only 20 subjects, 10 Caucasian and 10 African American, whose airway resistance and minimal cross-sectional areas were analyzed using anterior rhinomanometry and acoustic rhinometry at rest and 15 minutes after exercise. The Breathe-Right device was found to exert its main effect in the upper lateral cartilage region of the nasal valve, with an overall airway improvement of 21%.
Precise anatomic assessment is also important to predict which patients may benefit from improvement of nasal obstruction through rhinoplasty, and what maneuvers will be necessary. Boccieri and colleagues reported the use of spreader grafts in a series of 60 subjects undergoing primary rhinoplasty. All subjects fell into one of three groups who are prone to internal nasal valve collapse after primary rhinoplasty: those with narrow nose syndrome, with a narrow nasal vault and bulbous tip, and those with a crooked nose. Preoperative and postoperative rhinometric analysis indicated significant improvement in nasal valve obstruction, particularly in subjects with narrow nose syndrome or narrow nasal vault and bulbous tip. Subjects with a crooked nose had a less significant improvement. Boccieri and colleagues concluded that preoperative evaluation can identify patients who may be prone to nasal valve collapse after primary rhinoplasty, and that primary use of spreader grafts can support the internal nasal valve and alleviate need for a second surgery in the future.
Given the dynamic nature of the nasal valve, neuromuscular anatomic causes of nasal obstruction must also be considered. This may be a significant factor in patients with loss of facial musculature tone due to aging or facial paralysis. Facial paralysis results in a nonfunctional dilator naris muscle and aging can weaken the fibroareolar tissues of the nasal sidewalls, each leading to collapse of the nasal valve during inspiration. The impact of facial musculature tone upon nasal obstruction is well illustrated by Vaiman and colleagues who published two studies reporting on the treatment of nasal valve collapse with transcutaneous and intranasal electrical stimulation of the nasal musculature. The first was a prospective trial with electrotherapy versus placebo. Electrotherapy consisted of three 15-minute sessions per week for 10 weeks, with 10 to 12 months of follow-up. Sixty percent of subjects in the study group had a subjective improvement and 40% had objective improvement. Comparatively, 35% of the placebo group noted subjective improvement and 5% had objective improvement. Follow-up showed rapid decline in benefits and they concluded that electrotherapy alone was not a beneficial treatment of the nasal valve collapse. The second study built upon the first but focused more on muscle-building therapies. The report included three cohorts of subjects with clinical nasal valve collapse. Group one received transcutaneous and intranasal electrical stimulation of the nasal muscles only. For group two, treatment included biofeedback training and a home exercise program for specific nasal movements. Treatment for group three included the home exercises, electrical stimulation, and surface and intranasal electromyographic biofeedback-assisted specific strategies for nasal muscle education. Group two and three had 80% and 75% objective improvement, respectively. Group one had poorer results. They concluded that for select patients wanting to avoid surgery, relief of nasal valve collapse can be achieved with nonsurgical means. This data exemplifies the significant contributions of nasal and facial neuromusculature toward patency of the nasal valve.
Sinonasal Inflammatory Disease
Allergic rhinitis is the most common allergic condition in the world, and nasal congestion is notable for one of its most prominent and troublesome symptoms. Rhinitis patients appear to be more sensitive to decreases in cross-sectional nasal area. For example, nasal obstruction when lying down is a frequent complaint by patients. Nasal resistance is highest when the patient is in the supine position, and decreases as the head is elevated. This is most likely attributed to a nasal mucosal reaction to venous changes that alter local blood flow, secondary to compression of the neck veins or hydrostatic pressures. When the patient is in the lateral decubitus position, the dependent inferior turbinate is engorged and the turbinate in the superior position is constricted. Two other studies attributed the increase in nasal obstruction while in the supine position to the activities of the central autonomic nervous system or the autonomic shoulder and axillary sensory information linked to nasal reflexes. The perception of positional nasal obstruction is noted to be significantly higher in patients with rhinitis symptoms when compared with normals.
A study by Ciprandi and colleagues in June 2008 evaluated 100 subjects: 50 with short-term and 50 with long-term persistent allergic rhinitis. This study is the first to conclude that duration of persistent allergic rhinitis may lead to progressive worsening of nasal airflow, as determined by rhinomanometry (discussed later). It is important to recognize that asthma and allergic rhinitis are important comorbid factors, such that allergic rhinitis should be managed empirically in any patient with asthma and nasal obstructive symptoms while any additional workup is pending. The incidence of allergic rhinitis in patients with asthma may be as high as 80%. Although a complete discussion of rhinosinusitis is beyond the scope of this issue, it should be noted that nasal obstruction is a major symptom in all forms, acute and chronic.
Medical and Hormonal Causes
Because those with allergic rhinitis and chronic rhinosinusitis often self-medicate before specialty evaluation, patients must be queried regarding chronic intranasal decongestant use, including sympathomimetic amines (ephedrine/phenylephrine) and imidazoline derivatives (oxymetazoline and xylometazoline). These medications risk development of the syndrome of rhinitis medicamentosa with rebound nasal congestion, which typically occurs 5 to 7 days after use of the intranasal medication. Knipping and colleagues note that a loss and destruction of ciliated epithelial cells results in the disruption of mucociliary clearance and an increase in vascular permeability resulting in interstitial edema.
Systemic medical therapies may result in increased nasal obstructive symptoms. The most common of these include antihypertensive medications such as reserpine, hydralazine, guanethidine, methyldopa, and prazosin. Beta-blockers, such as propranolol and nadolol, and antidepressants and antipsychotics, including thioridazine, chlordiazepoxide amitriptyline and perphenazine, can also cause congestion. Hypothyroidism may result in nasal obstruction. Chavanne noticed an increase in nasal congestion and secretions in subjects who had undergone total thyroidectomy. The exact etiology of hypothyroid rhinitis is uncertain and is estimated to occur in approximately 40% to 60% of patients in a hypothyroid state. One proposed mechanism of effect is secondary to vascular dilation of the nasal mucosa. Antithyroid medications can mimic these symptoms, which should resolve upon withdrawal of the offending substance.
Rhinitis of pregnancy, also called rhinopathia gravidarum, has been frequently discussed in the literature; yet, the exact etiology of this is unknown. It is thought to occur in 5% to 32% of pregnant women, and is most prevalent during the first trimester. Isolated pregnancy rhinitis should resolve after the gestational period, such that ongoing symptoms should prompt additional workup. The assumed etiology is a combination of generalized increases in interstitial fluid volume, compounded by the direct effect of estrogen on the nasal mucosa, which causes increased vascularity and mucosal edema. Electron micrographic and histochemical studies performed by Toppozada and colleagues on the respiratory epithelium of pregnant women have suggested that an over activity of the parasympathetic system leading to increased glandular secretion and vascular congestion is responsible for the state of nasal congestion. This over activity of the parasympathetic system may be an allergic response to placental proteins, fetal proteins, or a woman’s own sex hormones. Bowser and Riederer noted a possible direct influence of progesterone on fibroblasts, and therefore, on the consistency of the nasal extracellular matrix. Additionally, this group proposed that estrogen and progesterone might cause rhinopathic symptoms indirectly by changing the concentration of neurotransmitters (eg, substance P, nitric oxide) and their receptors. Wolstenholme and colleagues recently studied 11 women on day 1 and 14 pre- and postcombined oral contraceptive therapy. These women had anterior rhinoscopy, peak inspiratory flow rate, acoustic rhinometry, anterior rhinomanometry, mucociliary clearance time, and rhinitis quality-of-life questionnaire scores recorded. The study concluded that modern day combined oral contraceptive pills have no effect on nasal physiology.
Traumatic Causes
Accidental trauma and sinonasal surgery may result in complications such as septal perforations, adhesions, nasal stenosis and empty nose syndrome. These conditions may precipitate obstructive symptoms through three mechanisms: (1) physical blockage of airflow, (2) induction of sinusitis, and (3) impaired sensation of airflow.
A detailed discussion of nasal trauma is beyond the scope of this issue, but it deserves mention that over resection of the inferior (or even middle) turbinates may result in empty nose syndrome, which, paradoxically, presents with nasal dryness or a sensation of nasal congestion. Causes for the symptom of nasal obstruction in these patients include disruption of normal airflow patterns, lack of surface area responsible for sensation of airflow, and ozena. These observations underscore the need for turbinate preservation during rhinoplasty and sinus surgery.
Neoplastic Causes
The entire spectrum of sinonasal neoplasms may present with nasal obstruction, which is the most common presenting complaint. This symptom, which may be associated with other nonspecific symptoms such as unilateral epistaxis or anosmia, often triggers otolaryngology referral for endoscopy or imaging. It is also noteworthy that the diagnosis of malignancy is often delayed as the most common symptoms, including facial pain/numbness, nasal obstruction, and epistaxis, are vague from the patient’s perspective. Squamous cell carcinoma is the most common malignant tumor of the sinonasal tract. The most common benign tumors include osteomas, which are rarely the primary cause of nasal obstruction, and inverting papillomas, which may transition to squamous cell carcinoma in 5% to 15% of cases. Two other entities deserve mention: juvenile nasopharyngeal angiofibroma and pyogenic granuloma. Juvenile nasopharyngeal angiofibroma must be considered in young patients with epistaxis. Nasal obstruction is still the most common symptom, seen in 80% to 90% of these cases. The finding of a large obstructing lesion along the anterior nasal septum, especially in a pregnant patient, likely represents a pyogenic granuloma, which is a reparative vascular lesion rather than a true neoplasm.
Atypical and Idiopathic Lesions
Atypical inflammatory disorders including Wegener’s granulomatosis, tuberculosis, sarcoidosis, rhinoscleroma, and rhinosporidiosis may present with nasal lesions, friable mucosa, or crusting, and hence, symptoms of obstruction. Cocaine abuse must be ruled out in patients with such findings. An important diagnosis to consider in the differential is extranodal NK/T-cell lymphoma, which may initially manifest as an intranasal purple granulomatous mass with bleeding. This rapidly progresses to widespread local tissue destruction involving the midface. A finding of nasopharyngeal lymphoid hypertrophy in an adult should be further investigated and an HIV test should be recommended. The prevalence of nasopharyngeal lymphoid hypertrophy in patients with early stages of HIV infection is anywhere from 56% to 88%. This hypertrophy and nasal obstruction may improve as the patient’s immunocompromised state declines.
History and physical examination
A complete history and head and neck examination are critical to accurately diagnosing the underlying etiology of a patient’s nasal obstructive symptoms. It is important to query patients about over the counter medication use, possible allergic triggers (eg, pets) and previous surgery, as some will deny prior aesthetic procedures. Observations that may be present on physical examination include midface deformities that may result from chronic mouth breathing. Patients with allergic rhinitis may exhibit the classic allergic shiners or allergic salute. Facial nerve function should be assessed, as paralysis of the splinting muscles of the nasal ala may result in a functional nasal airway obstruction. Middle ear effusions may be a manifestation of chronic nasopharyngeal inflammation, adenoid hypertrophy, or an obstructing mass near the eustachian tube. Purulent discharge or facial tenderness suggests sinusitis.
The nose should be examined with consideration of airflow dynamics and the sites of increased resistance. A suggested method is to focus on external support structures, followed by an assessment of internal support structures, and lastly evaluate internal soft- tissue structures. If the patient has a prior history of rhinoplasty, note if the patient’s nasal bridge has been overly narrowed by osteotomies. Severe tip ptosis can also contribute to nasal airway obstruction because it may redirect airflow superiorly, which can be perceived as nasal airway obstruction. If nasal tip ptosis is indeed contributing to symptoms, tilting the tip superiorly will considerably improve the patient’s symptoms. The patient should be observed during quiet and deep inspiration and the physician should assess upper and lower lateral cartilage competency. Early collapse during inspiration would suggest valve incompetence.
The first area of interest endonasally is the internal nasal valve which is the smallest cross-sectional area in the nasal cavity. Care must be taken not to distort the valve with the nasal speculum, and often the valve can be adequately examined by simply lifting the nasal tip superiorly. The Cottle maneuver, a test of nasal valve integrity, can be performed by retracting the cheek laterally, pulling the upper lateral cartilage away from the septum and widening the internal nasal valve angle (see Fig. 2 A–C). If the patient’s symptoms are relieved with this maneuver, this suggests the cause of the nasal airway obstruction is related to the nasal valve area (eg, dorsal septal deviation, lack of upper lateral cartilage integrity). False negatives can be seen with synechiae in the nasal valve which prevents the valve from opening during the maneuver. Aggressive lateral osteotomies can result in over medialization of the ascending process of the maxilla resulting in a decrease in the cross-sectional area of the posterior lateral nasal valve area, also resulting in a false negative finding during the Cottle maneuver. Another simple technique involves using a cotton swab or nasal speculum to lateralize the upper lateral cartilage from inside the nose, and the patient is again asked if their symptoms are improved. This technique enables direct observation of the nasal valve area as it widened.
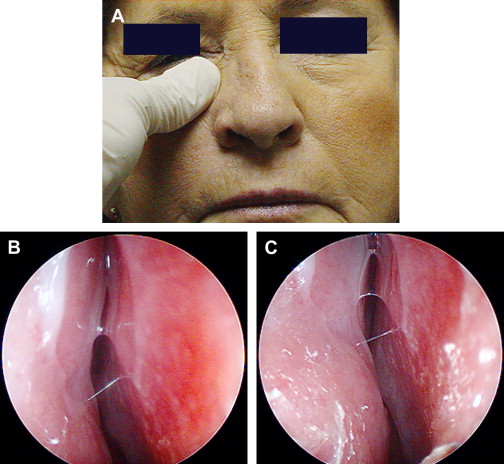
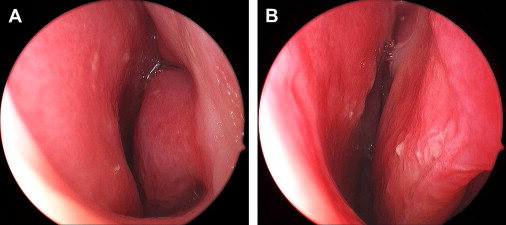
Complete examination of the septum, turbinates, meati, and internal valve is best accomplished with diagnostic nasal endoscopy. This should be performed before and after decongestion ( Fig. 3 A, B ) to assess the decongestant response and to rule out posterior septal deviations, middle turbinate resection or scarring to the lateral nasal wall, inflammatory disease, polyps, foreign bodies, and neoplasms. If the nasal airway obstruction improves with decongestion alone, this suggests a mucosal inflammatory disorder of the inferior turbinates. No response suggests the etiology of the obstruction is of a rigid, structural nature such as nasal valve obstruction, septal deviation, or bony hypertrophy of the inferior turbinate. It should be noted that some mucosal inflammatory disorders may also exhibit lack of decongestive response, including rhinitis medicamentosa or diffuse nasal polyposis. Recently, Lanfranchi and colleagues published a report on the importance of nasal endoscopy in the preoperative examination of patients with nasal obstruction who present for rhinoplasty. This series of 96 subjects undergoing rhinoplasty revealed that preoperative endoscopy allowed the diagnosis of pathology requiring additional surgery in 28 subjects (30%). The pathologies included concha bullosa, posterior septal deviations, adenoid hypertrophy, choanal stenosis, and one intranasal tumor. During endoscopy, the surgeon must maintain vigilance to rule out neoplasia ( Fig. 4 ) and to recognize subtle signs of atypical inflammatory disease such as mucosal nodularity, crusting, friable mucosa, or synechiae. An algorithm is presented ( Fig. 5 ).
Radiologic Evaluation
Because the source of obstruction is not always evident by patient history and physical, radiography may be required to assist with diagnosis. CT can be used to evaluate structural/bony abnormalities such as a deviated septum, nasal bone fractures, choanal atresia, and sinus disease. CT may also reveal unexpected anatomic findings such as concha bullosa of the inferior turbinate or foreign body. MRI, because of its soft tissue detail, is better suited for evaluating the integrity of the dura and for further assessment of certain nasal masses (such as encephalocele or glioma).
Objective Evaluation and Diagnostic Studies
Although subjective evaluation of nasal obstruction can be accomplished using a nasal obstruction visual analog scale (NO-VAS), it is often preferable to obtain quantitative objective assessment. Hygrometry was one of the first objective measures of the nasal airway. This technique was described by Zwaardemaker in 1894 and involved having the patient breathe onto a mirror. The diameter of the fog produced by each nostril was compared. In 1902, Spiess described the “hum-test,” a technique where he used the change in the timbre of sound produced during humming while externally occluding the decongested nasal side to assess nasal airway patency.
Today, methods for objective assessment of nasal airway include:
- •
Peak nasal inspiratory flow (PNIF)
- •
Acoustic rhinometry (AR)
- •
Rhinomanometry (RM)
- •
Software-based analysis of acoustic signals is also in evolution. These objective measures have uses in both research, and less frequently, in clinical settings. For example, these studies can be used pre- and postdecongestion in an attempt to predict the efficacy of certain medical and surgical therapies. Lund stresses the importance of objective testing because of the high patient dissatisfaction rate (30%) after surgery to resolve nasal airway obstruction. Acoustic rhinometry and rhinomanometry can also be used for nasal provocational studies in patients with suspected allergic rhinitis and recently has been used for assisting in the diagnosis of obstructive sleep apnea and sleep disordered breathing. These studies are commonly used in the research setting, but clinical use is not widespread in the United States due to expense, availability of equipment, variability of operator, and inconsistencies with consensus data correlating subjective measures with objective measures.
Peak Nasal Inspiratory Flow
PNIF is a noninvasive, easy to perform method commonly used to assess nasal patency. It is a physiologic measure indicating the peak nasal airflow in liters per minute achieved during maximal forced nasal inspiration. Given that the transnasal pressure differences are not recorded, PNIF is thought to be susceptible to high variability based on effort and cooperation from the subject and correct instructions from the investigator. This use of maximum effort also increases the incidence of turbulent airflow. Another concern with PNIFs is the lack of this measurement representing true physiologic conditions, as normal breathing starts at a significantly lower tidal volume. Ultimately, the method is suggested to be reliable for assessment of nasal patency as it has proved to be reproducible and in concordance with other objective tests. Furthermore, respiratory comorbidity could potentially affect the PNIF measurements by limiting the inspiratory effort.
Acoustic Rhinometry
In 1989, Hilberg and colleagues were the first to use AR to measure the cross-sectional area in the nasal airway. AR is a simple, noninvasive, and relatively cheap way to measure nasal airway cross-sectional area as a function of longitudinal distance along the nasal passageway following the path of an acoustic impulse. It is the most common method used for measurements of nasal cavity geometry. Nasal passage volumes can be calculated from contiguous cross-sectional values. The method is appropriate for anatomic assessment and structure of the nasal airway, drug actions and surgical changes in the nasal cavity including change in the mucovascular components of the nasal valve area, and changes based on certain pathology such as nasal polyposis or septal deviation.
The technology of AR was originally devised for oil investigation, however, it wasn’t until the 1970s that it was first used in the field of medicine to perform measurements in the distal airway. The acoustic rhinometer consists of a sound source, wave tube, microphone, filter, amplifier, digital convertor, and a computer. A sound wave is transmitted into the nasal cavity which is then reflected back from the nasal passages and converted into digital impulses, which are then constructed on a rhinogram. This rhinogram provides a two-dimensional anatomic assessment of the nasal airway. The cross-sectional area of the nose differs at different points from the nasal rim, and these variances are detected by changes in acoustic impedance. Each notch on the rhinogram represents a different anatomic constriction in the nasal cavity ( Fig. 6 ). The first notch represents the nasal valve and is usually the minimal cross-sectional area (MCV) in the normal nose. The second notch represents anterior portions of the inferior turbinate or middle turbinate, while the third notch is estimated to be in the area of the middle/posterior end of the middle turbinate. Each notch identifies a site of limitation of nasal airflow and can be used to locate the site of obstruction in the nose (see Fig. 6 ).



