This article provides a review of contemporary techniques in nasal septal surgery. Relevant anatomy and physiology of the nose and nasal septum are discussed. The essentials of a complete diagnostic evaluation are outlined. The evolution of surgical approaches to the correction of a deviated septum, including classic submucosal resection, traditional septoplasty, and open techniques, is covered. Complications of septoplasty are reviewed, with an emphasis on prevention and treatment. The recently popularized endoscopic septoplasty, a significant advance in septal surgery, is addressed elsewhere in this issue.
The nasal septum is a central support structure for the nose. When significantly deformed, the septum may cause dysfunction and cosmetic deformity, potentially having an impact on the many functions of the nasal cavity.
Nasal obstruction is the most common complaint in an average rhinologic practice, and a deviated nasal septum is the most common cause of nasal obstruction. It has been estimated that as many as one third of the population has some nasal obstruction, and as many as one quarter of these patients pursue surgical treatment. Often, the patient provides a history of trauma to the nose; however, many times, there is no clear history of an inciting event. The initial insult to the nasal septum may have been caused by birth trauma or by microfractures occurring early in life that have led to asymmetric growth of the septal cartilage.
The evaluation of a septal deviation causing nasal obstruction depends heavily on physical examination and, possibly, imaging. Interestingly, studies have shown that the degree of septal deviation has little correlation with subjective ratings of nasal obstruction. Once a septal deviation is diagnosed, however, medical management targeting the nasal mucosa is typically attempted first with topical nasal steroids, antihistamines, and decongestants as tolerated. If the patient fails medical therapy, a surgical intervention to correct the underlying septal deformity is considered.
Apart from nasal obstruction, a significantly deviated nasal septum has been implicated in epistaxis, sinusitis, obstructive sleep apnea, and headaches attributable to contact points with structures of the lateral nasal wall. These conditions are also accepted indications for septoplasty, although some, such as facial pain or headache, may be controversial. Additionally, if the deviated nasal septum impairs access to the middle meatus, which is necessary to perform effective sinus surgery or endoscopic orbital procedures (eg, dacryocystorhinostomy, orbital decompression), or if a transseptal transsphenoidal hypophysectomy is pursued, a septoplasty may be advantageous as well.
Embryology and anatomy of the nasal septum
During development of the face, five facial prominences form the nose:
- 1.
Frontal prominence
- 2.
Paired medial prominences
- 3.
Paired lateral prominences
The nasal septum begins as a downward growth of the frontal prominence. As the primary and secondary palatal shelves join, the descending septum fuses with the palate to separate the nasal cavity into two distinct nasal passages.
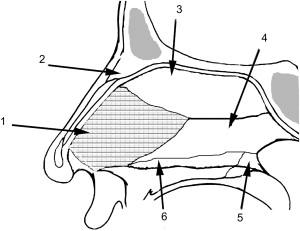
The nasal septum consists of a membranous component anteriorly, a cartilaginous component, and an osseus component posteriorly. The membranous septum is located between the columellar lower lateral cartilages and the quadrangular cartilage posteriorly. It is composed of fibrofatty tissue. The septal cartilage, also known as the quadrangular cartilage for its geometry, is located just posterior to the membranous portion of the septum. Posteriorly, the nasal septum becomes osseus and consists of the perpendicular plate of ethmoid, the nasal crest of palatine and maxillary bones, and the vomer dividing the posterior choanae ( Fig. 1 ). The lateral surfaces of the septal cartilage and bones are invested with the mucoperichondrium and mucoperiosteum, respectively. There is a decussation of fibers from these investing layers, which is particularly thick and densely adherent inferiorly, where the quadrangular cartilage meets the maxillary crest. The mucosa of the septum is composed of a pseudostratified columnar respiratory epithelium along the inferior two thirds and often contains olfactory epithelium along the superior one third.
The arterial supply of the nasal septum stems from the internal carotid and external carotid systems. The anterior and posterior ethmoidal arteries, which are branches of the ophthalmic artery, comprise the internal carotid component. The sphenopalatine artery, the terminal branch of the internal maxillary artery, and the superior labial artery (a branch of the facial artery) comprise the external carotid component. These arterial branches create an extensive plexus along the septum bilaterally that is especially evident during periods of epistaxis, which most commonly occurs along the anterior nasal septum in a region known as Kiesselbach’s plexus. This rich anastomotic network is also responsible for the excellent healing properties of the mucoperichondrium or mucoperiosteum.
The nervous supply to the nasal septum originates from the trigeminal nerve (CN V). The posteroinferior half of nasal mucosa is innervated by the nasopalatine nerve, a branch of the maxillary nerve (CN V2). The superoanterior half of nasal mucosa is innervated by anterior ethmoidal nerves, branches of the nasociliary nerve from the ophthalmic nerve (CN V1). Superiorly, the mucosa is innervated by the olfactory nerve (CN I), with nerve endings traversing the cribriform plate through multiple tiny foramina.
Functionally, the internal nasal valve is of great significance. This region is the narrowest point of the upper airway and is defined by a two-dimensional plane slicing through the caudal end of the upper lateral cartilages superiorly; the alae laterally, along with the head of the inferior turbinate; and the bony nasal floor inferiorly. The septum defines the medial aspect of the internal nasal valve. The internal nasal valve is a point at which small changes in the nasal septal structure can have significant effects on airflow resistance and the sensation of obstruction.
History of septoplasty
Written accounts describing correction of nasal septal deformities date back to the beginning of medical literature in the Egyptian papyri. The Edwin Smith papyrus suggests treating the broken nose by placing two plugs of linen coated with grease within each nostril and then applying stiff rolls of linen externally to fix the fracture. In the late 19th century, the Bosworth operation was the most common procedure to correct septal deviation. This procedure required the surgeon to amputate the deviation, along with the mucosa of the convex side. It was recognized at that time that the contralateral mucosa needed to be preserved; nonetheless, this technique resulted in frequent perforations. Around this period, Adams and Asch advocated fracturing the septum, followed by splinting. Asch additionally suggested using full-thickness cruciate incisions to eliminate the resilient memory of the septal cartilage. Shortly thereafter, Killian and Freer published a technique involving raising the subperichondrial flaps and resecting the septal cartilage while leaving the overlying mucosa intact.
They emphasized that an L-shaped cartilaginous strut must be left dorsally and caudally for nasal support. This technique is known as the submucous resection (SMR) and is still widely used today. In 1929, Metzenbaum addressed the issue of the caudal septal deviation. He used a vertical incision to mobilize the caudal strip of cartilage back to the maxillary crest in the midline, where it was fixed with suture. Several years later, Peer recommended modifying this procedure when the caudal segment was curved or fractured. In this situation, Peer advised to resect the caudal segment and to graft a separate piece of septal cartilage in its place. In 1948, Cottle and Loring described conservative resections of deflected septal cartilage as well. Complications of significant cartilage resection and the SMR procedure, including large septal perforations and saddle nose deformity, were encountered, and a more conservative approach eventually gained popularity.
These developments provide the foundation of modern nasal septal surgery. Newer innovations, such as endoscopic septal surgery and extracorporeal septoplasty (in which a portion of the septal cartilage is removed, modified, and replaced), have built on the established tenets of intact flap elevation and careful reapproximation, preservation of dorsal and caudal support mechanisms, conservative resection, and meticulous surgical technique. With the proliferation of endoscopic techniques, the use of the endoscope to examine the nasal cavity and septum closely and also to correct deformities successfully has been gaining acceptance as a sound alternative for pathologic conditions not involving the anterocaudal septum. In its varied forms, septoplasty has grown to become one of the most commonly performed procedures in otolaryngology.
History of septoplasty
Written accounts describing correction of nasal septal deformities date back to the beginning of medical literature in the Egyptian papyri. The Edwin Smith papyrus suggests treating the broken nose by placing two plugs of linen coated with grease within each nostril and then applying stiff rolls of linen externally to fix the fracture. In the late 19th century, the Bosworth operation was the most common procedure to correct septal deviation. This procedure required the surgeon to amputate the deviation, along with the mucosa of the convex side. It was recognized at that time that the contralateral mucosa needed to be preserved; nonetheless, this technique resulted in frequent perforations. Around this period, Adams and Asch advocated fracturing the septum, followed by splinting. Asch additionally suggested using full-thickness cruciate incisions to eliminate the resilient memory of the septal cartilage. Shortly thereafter, Killian and Freer published a technique involving raising the subperichondrial flaps and resecting the septal cartilage while leaving the overlying mucosa intact.
They emphasized that an L-shaped cartilaginous strut must be left dorsally and caudally for nasal support. This technique is known as the submucous resection (SMR) and is still widely used today. In 1929, Metzenbaum addressed the issue of the caudal septal deviation. He used a vertical incision to mobilize the caudal strip of cartilage back to the maxillary crest in the midline, where it was fixed with suture. Several years later, Peer recommended modifying this procedure when the caudal segment was curved or fractured. In this situation, Peer advised to resect the caudal segment and to graft a separate piece of septal cartilage in its place. In 1948, Cottle and Loring described conservative resections of deflected septal cartilage as well. Complications of significant cartilage resection and the SMR procedure, including large septal perforations and saddle nose deformity, were encountered, and a more conservative approach eventually gained popularity.
These developments provide the foundation of modern nasal septal surgery. Newer innovations, such as endoscopic septal surgery and extracorporeal septoplasty (in which a portion of the septal cartilage is removed, modified, and replaced), have built on the established tenets of intact flap elevation and careful reapproximation, preservation of dorsal and caudal support mechanisms, conservative resection, and meticulous surgical technique. With the proliferation of endoscopic techniques, the use of the endoscope to examine the nasal cavity and septum closely and also to correct deformities successfully has been gaining acceptance as a sound alternative for pathologic conditions not involving the anterocaudal septum. In its varied forms, septoplasty has grown to become one of the most commonly performed procedures in otolaryngology.
Submucous resection
The textbook and surgical atlas descriptions of SMR have not varied significantly in the past 50 years ( Table 1 ). The basic procedure removes most of the quadrangular cartilage, leaving an inverted L-shaped strut for structural support ( Fig. 2 ). Bony portions of the septum that are significantly deformed are also resected. The SMR procedure can leave a large defect in the cartilage and osseous portions of the septum. These large defects have been associated with increased risk for complications. Other researchers have made the point that removal of most of the quadrangular cartilage decreases the need for repeat surgery. Most surgeons now blend SMR and septoplasty techniques to address the unique deformities encountered in each patient.
| Source Title | Editor | Year | Page |
|---|---|---|---|
| Atlas of Head and Neck Surgery | Lore JM | 1962 | 90–102 |
| Scott Brown’s Otolaryngology, 5th Edition | Kerr AG | 1987 | 154–169 |
| Principles and Practice of Rhinology | Goldman J | 1987 | 385–394 |
| Atlas of Head and Neck Surgery | Johns ME | 1990 | 109–120 |
| Atlas of Head and Neck Surgery–Otolaryngology | Bailey BJ | 1996 | 828–831 |
| Operative Otolaryngology–Head and Neck Surgery | Myers E | 1997 | 21–37 |
| Otolaryngology Head and Neck Surgery, 3rd Edition | Cummings CW | 1998 | 921–948 |
| Otolaryngology–Head and Neck Surgery, 4th Edition | Bailey BJ | 2006 | 307–334 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


