Chapter 114 Retinopathy of Prematurity
Introduction
Retinopathy of prematurity (ROP) affects thousands of children each year. Fortunately, ROP causes blindness in only a small percentage. ROP was previously called “retrolental fibroplasia.” The original work in the 1950s of Kinsey et al.1 and Patz and Kinsey2 showed that oxygen contributes to the tissue change described as ROP. It was believed that if the arterial oxygen was kept within prescribed guidelines, ROP might be eliminated. However, with the ability of neonatologists to keep alive newborns of very low birth weight and very young gestational age, there has been a resurgence of ROP despite tight control of the partial pressure of oxygen.
Oxygen’s role in ROP has come under extensive investigation. Many workers have shown in animal models, that immature vessels characteristic of ROP can be produced but not retinal detachment.3–6 Clinical observations by many investigators have shown that ROP can be seen in 85–90% of children of low birth weight when exposed to oxygen.7 Similar clinical pictures have been seen in full-term infants, in familial exudative vitreoretinopathy, and in infants of mothers who are cocaine users.8,9
Recently, the role of vascular endothelial growth factor (VEGF) in ROP has been more appreciated. VEGF under control of oxygen concentration or retinal ischemia can overcome the genetic mandate to form normal retinal vasculature and instead contribute to neovascularization or development of abnormal intraretinal vascular patterns in the retinal periphery.10
Classification system
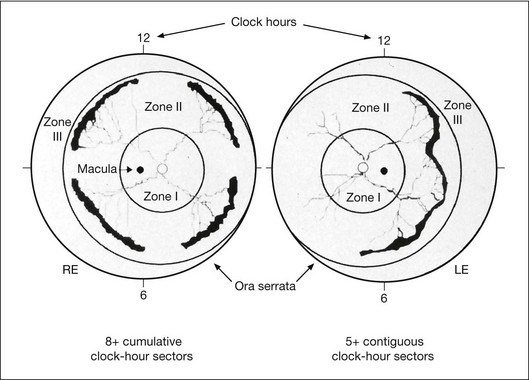
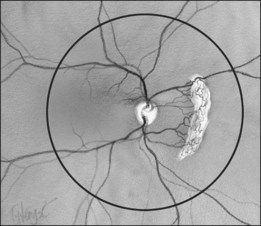
In the past, there were several classifications of ROP, which led to much confusion between ophthalmologists, neonatologists, and pediatricians. However, an International Classification of Retinopathy of Prematurity (ICROP) has now been adopted. It describes three zones of the eye. Zone I uses the optic nerve as the center of a circle, and the radius is defined as twice the distance between the foveola and the optic nerve. Zone II uses as a radius, the distance between the nasal ora serrata in the horizontal meridian and the center of the optic nerve. All of the remaining retina is zone III (Fig. 114.1); that is, zone III is present in all meridians except at the nasal horizontal meridian.
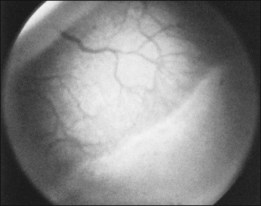
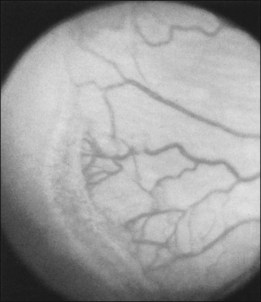
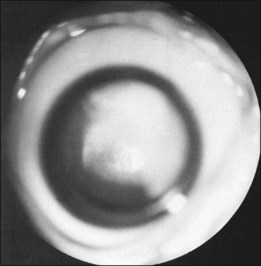
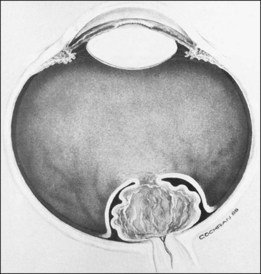
The ICROP defines five stages of ROP. The process of ROP begins at the junction between the vascular and avascular retina. ROP is described as stage 1 if a narrow white line is present at the junction. Stage 2 is a ridge of activity that shows thickening of this line (Fig. 114.2). In addition to this thickening, there is sometimes a ruddy appearance of a shunt within this ridge. Stage 3 involves the growth of vessels from the retina toward the vitreous cavity immediately posterior to and contiguous with the ridge (Fig. 114.3). Stage 4 is a partial retinal detachment and is subclassified as 4A, with the macula attached, and 4B, with the macula detached. Stage 5 implies a total detachment of the vascularized retina (Fig. 114.4) and can be classified further depending on the opening or closure of the anterior and posterior aspects. Even with significant retinal detachment causing a white retrolenticular appearance, the very far peripheral avascular retina often remains attached (Fig. 114.5). The avascular peripheral retina, however, may not be visually functional.
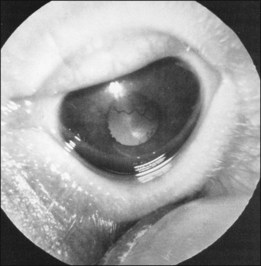
Finally, the ICROP addresses the problem of “plus disease.” It is not a disease different from ROP but is a descriptive term for dilated and tortuous vessels of the posterior pole. In addition, the anterior segment in plus disease often shows dilated iris vessels (Fig. 114.6). These iris vessels may not be true neovascularization of the anterior segment but may represent dilation of an existing tunica vasculosa lentis.11–13 This anterior segment vessel dilation appears to be a manifestation of a generalized intraocular increased VEGF concentration.
• First, ROP presenting completely in zone 1 or posterior zone 2 as mentioned above usually has a more aggressive course and this type of ROP may require more aggressive ablative treatment.
• Second, the stage 3 neovascularization of ROP may appear differently depending on the zone of involvement: (1) mid and anterior zone 2 and zone 3 neovascularization is always posterior to the ridge tissue and growing into the vitreous cavity and (2) zone 1 and posterior zone 2 can be flat, lying along the retinal surface, without the typical ridge tissue features.
• Third, plus disease is a function of an open shunt vessel contained deep within the ridge tissue. As this arteriovenous shunt is established, the vessels become dilated in the periphery. With the advent of wide-angle photography, this image can be easily appreciated. Although “plus disease” is a posterior pole finding and should remain so, the dilated peripheral vessels have been referred to as “pre-plus” and suggests that the eye is at higher risk of developing frank “plus disease.”
In order to try to identify eyes at high risk of progression, the authors have adopted a modification of the ICROP system. Namely, we designate the number of clock hours of vessels that are entirely in zone 1 by a subscript. For example, if all 12 clock hours are in zone 1 that would be written zone 112. Additionally, if flat neovascularization is present, we use another subscript, “F.” Stage 3F denotes flat neovascularization is present. Since these vessels lie flat on the retina and appear anterior to the shunt vessels, the drawing of the findings show the extent of the clock hours of the flat stage 3 (Fig. 114.7).
Histophysiologic features, clinically relevant cell biology, and pathophysiology
Stages 1 and 2
Much work has been done to promote the understanding of the early changes at the junction of the vascular and avascular retina. Foos8 speaks of a vanguard and rearguard of cells that contribute to the tissue changes.3,11 These cells have been infrequently studied in their active form because most of these neonates survive and the eyes do not become available for study. Other authors13 have described the cells in this region as “spindle shaped.” These spindle-shaped cells are found in many proliferative processes, and this descriptive term does not help define the cell biology. Histologic features of the avascular and vascularized retina reveal a difference in the retina’s thickness, with the posterior vascular retina being somewhat thicker than the more peripheral avascular retina.
Terry14 was perhaps the first to note vitreous abnormalities in children with ROP. The vitreous, which is normally firm and dense in the newborn, is synergetic and organized into fluid lacuna and sheets of collagen in ROP. This vitreous abnormality seems to be present in children with lesser stages of ROP and certainly is present in children with more advanced stages. The significance of these vitreous abnormalities may relate to both development of exudative and tractional detachments and to development of late rhegmatogenous retinal detachments. ROP should be thought of as a vascular vitreoretinopathy. Stage 1 ROP is the visible white line that separates the vascular from the avascular retina. In stage 2 that line widens and may become a salmon color as the shunt vessel opens.
Stage 3
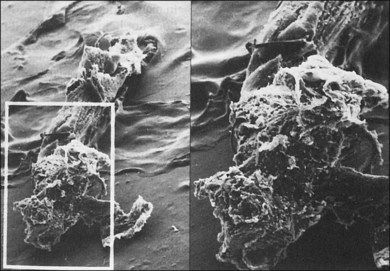
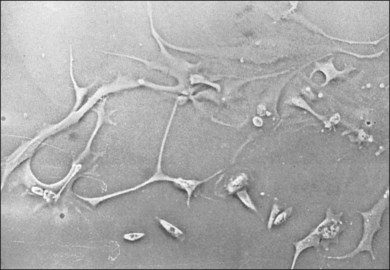
The classical concept of neovascularization in ROP is that a retinal vasoconstriction secondary to oxygen administration or an increase in oxygen concentration as seen with birth alone is followed by vasodilation and associated vascular budding after oxygen withdrawal. However, some infants show significant vasodilation or plus disease even while receiving supplemental oxygen. No matter what the mechanism, the neovascularization that develops in stage 3 ROP has interesting features. One is that the active vessels are usually present at the posterior ridge of tissue. Also, there is often a directional orientation of the vessels toward the posterior apex of the lens in zones 2 and 3. One of the most curious findings of the more posterior ROP is the lack of ridge tissue seen in eyes with extensive shunts and plus disease. The concept of Foos and spindle cells is based on eyes with changes in mid-zone 2 and the absence of ridge tissue is a posterior finding. One suggestion is that the angioblast cells and the astrocyte cells do not meet until the progenitor cells have progressed from the area of the disc into mid-zone 2 in the animal models of ROP.15 This still leaves the difference in appearance of the flat stage 3 neovascularization in zone 1. It may be that the secondary vitreous formed by vascularized retina may dictate at least in part the position of the neovascular fronds. The more posterior smaller-volume vitreous cavity may produce enough secondary vitreous to press the frond along the retinal surface. As is known from diabetic retinopathy, these fronds tend to grow on the posterior hyaloid surface. As the vascularized retina expands, the volume of secondary vitreous needed to fill the hemisphere of the vitreous cavity may not keep pace and allow vessels to grow along the anterior surface of the developing secondary vitreous toward the center of vitreous cavity or toward the lens. This organization of vitreous collagen or hypocellular gel contraction requires few cells to organize large amounts of collagen, as seen in eye tissue samples with stage 5 ROP (Fig. 114.8). In tissue culture, cells have been identified that have the ability to organize large amounts of collagen (Fig. 114.9). It is believed these cells organize anterior vitreous collagen into a plane that allows the vessels to grow on a surface anteriorly toward the posterior aspect of the lens.
Distortion of retinal vascular architecture
Machemer16 suggested that avascular retina is more elastic because it lacks retinal vessels and that this helps explain why the peripheral avascular retina can stretch over large areas of retinal pigment epithelium (RPE). In contrast, we believe that the organization of the cortical vitreous collagen, which is formed by and intimately attached to the vascularized retina, makes this stretching of the vascularized retina difficult. This inelastic cortical vitreous collagen and retinal ridge inhibits stretching of the vascularized retina. It is the absence of the cortical collagen over areas of avascular retina that allows the avascular retina to be stretched over large areas of RPE. Circumferential stretching of the retina is often recognized because of distortion of retinal vessels and is associated with an incomplete retinal ridge.
Stages 4 and 5
ROP has both exudative retinal detachments and tractional retinal detachments. In the evolution of retinal detachments of ROP, at least three factors are involved. The first is the existence of permeable, leaky blood vessels, as seen in stage 3 ROP. These vessels, within the shunt and posterior to the ridge, are capable of supplying large amounts of proteinaceous fluid to both the vitreous cavity and subretinal space. Second, as shown by Ashton and Cook,17 the neovascularization that is commonly thought of as growing only into the vitreous cavity also can be seen growing into the subretinal space (Hirose, pers. comm.). Third, these blood vessels can bleed into both the vitreous cavity and subretinal space. Foos18 showed that eyes with vitreous hemorrhage are susceptible to retinal detachment and seem to have a worse prognosis for total retinal detachment.
Okamoto et al.19 have shown in a murine model that neovascularization into the subretinal space from the retina is produced in areas of VEGF promoter. Cells from the retinal ridge or regressing hyaloid and tunica vasculosa lentis organize vitreous collagen that is tightly attached to the retina. This creates traction on these permeable vessels and results in additional leakage of fluid or blood from these vessels. In children who develop stage 4 ROP, the retinal ridge is the most common location for retinal detachment to begin. Detachments without traction in the area of the ridge often settle spontaneously.20
In eyes with ROP, cells that organize the vitreous appear to migrate into the vitreous cortex from the ridge of retina between avascular and vascular retina and from the area of the optic disc. This means that manipulation of these two areas is important to resolve the tractional component of retinal detachment. It also may be that the cells of the primary vitreous or tunica vasculosa lentis, or both, now called “ocular fetal vasculature,” may contribute cells to this hypocellular gel contraction. The genetically determined apoptosis of the cellular elements of the primary vitreous and tunica vasculosa lentis may be clinically slowed or reversed under the influence of increased VEGF. The higher the concentration of VEGF, the less the apoptosis proceeds, and the more cells are available to organize vitreous collagen and contribute to retinal traction.21
We, and colleagues, have grown cells in tissue culture from the retrolenticular membrane of stage 5 ROP eyes. These cells have been studied by immunofluorescent techniques and appear to be predominately neuroglial in origin. Some cells seemed very immature, perhaps representing multipotential cells that have migrated from the retina into the vitreous cavity. These cells show the ability to organize large amounts of collagen in vitro, as well as the ability to produce collagen. When these cells are tested for collagen organization against cells from both proliferative vitreoretinopathy and tractional diabetic retinal detachment, the cells of ROP are able to organize much more collagen than the proliferative vitreoretinopathy cells.22,23 This organization of vitreous collagen into sheets is supported by the original observations of Terry14 in eyes with ROP.
Development of stage 4A ROP retinal detachments
In stage 4A ROP, the detachment begins at the ridge of the retina. Fluid can leak posteriorly under the retina and cause the posterior retina to detach as well. When a primarily exudative retinal detachment develops, the retinal surface is smooth and shows no evidence of epiretinal proliferation or peaked folds. This is a significant observation in our clinical experience, eyes with smooth anterior retinal surfaces, despite large areas (four disc areas) of retinal detachment, sometimes flatten spontaneously over several months. When the retina flattens, however, the RPE is often disrupted, and many eyes do not have useful vision. As cells migrate into the vitreous cortex along the surface of the vascularized retina, both anteriorly from the ridge and posteriorly from the disc, they can form folds in the retina. These cells can convert a predominately exudative retinal detachment to a predominately tractional detachment. Machemer,16 Charles,24 and others often discussed the peripheral retinal “trough,” or anterior loop traction, associated with ROP. The vitreous is organized in a fashion that allows the retina to form a trough in the far periphery. As retinal detachment in ROP evolves, its configuration depends partly on the symmetry of the retinal ridge. A ridge that contracts evenly and is located an equal distance from the disc in all meridians results in a detachment that closes centrally.
Subretinal fluid can have several clinical manifestations. It can be opalescent or red, being either serum or blood in the subretinal space. This fluid may have a toxic effect on the neurosensory retina and RPE, in addition to the expected degenerative effect on the photoreceptors from retinal detachment itself. This subretinal fluid has been found to have high concentrations of hemoglobin and iron, both bound and unbound.25,26 In addition, cholesterol is often found in the subretinal space, either crystallized or in solution. Opaque subretinal fluid, after even spontaneous reattachment, appears to leave the eye with disrupted RPE and presumably a poor visual result.
Clinical considerations
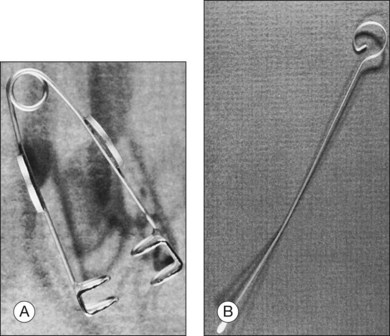
In the results of the Cryotherapy for Retinopathy of Prematurity study,27 and Early Treatment for Retinopathy of Prematurity study,28 a positive treatment effect was reported, and it was suggested that infants be examined at 4–6 weeks after birth and before 31 weeks PMA if they are 1500 g or less birth weight. These infants need to be examined meticulously, including indirect ophthalmoscopy, for vascularization of the anterior segment, pupillary dilation, plus disease, zone of eye involvement, and stage of the disease process. The authors have found that the Alfonso lid speculum (Fig. 114.10A) and Kelge swab (Fig. 114.10B), accompanied by the indirect small pupil ophthalmoscope and 28 diopter lens, are the best instruments to examine the peripheral retina in the neonate. We do not use topical anesthesia because this can cause clouding of the cornea.
Photographic imaging
The Photo-ROP (Photographic Screening for Retinopathy of Prematurity) study and that of Ells et al. evaluated and confirmed the utility of photographic imaging in ROP screening.29,30 This photographic imaging allows a very good representation of the posterior pole and the mid periphery of the eyes of premature infants. Photographic documentation in diabetes, age-related macular degeneration, and other retinal vascular disease is well known.31–33 and photographic documentation of ROP has been available for several years and is equally valuable. Treatment in ROP in large part is driven by zone 1 and particularly zone 2 findings, well seen with photography.29
The interpretation of these pictures requires they be obtained and managed in a timely fashion and read by a qualified reader. Retinopathy of prematurity is a time-dependent disease, allowing development of stage 1 to stage 5 to occur in as little as 2 weeks.34–36 FocusROP (FocusROP, LLC, Troy, MI), an internet-based, HIPAA-compliant, secure website using certified and expert readers, has been developed to handle these images. This website (www.FocusROP.com), receives the uploaded digital information obtained by trained individuals in the neonatal care centers and immediately notifies a previously certified local ophthalmologist to read these images. The follow-up algorithm contained in the software program allows only a very conservative examination schedule.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


