Retinopathy of Prematurity
J. Arch Mcnamara
William Tasman
HISTORY
Retinopathy of prematurity (ROP) was first described in 1942 by Terry.1 He named the disease retrolental fibroplasia (RLF). Many different etiologies were proposed for RLF, including an infection that was either primary or transmitted from the mother,2 vitamin E deficiency,3 and anoxia.3,4 In the early 1950s, hyperoxia was implicated in the growing incidence (described as an “epidemic”) of RLF. Kinsey and Zacharias5 reported retrospective data that implicated oxygen, vitamins, and iron in the increasing incidence of RLF. Campbell6 in Australia and Crosse and Evans7 in England presented both prospective and retrospective evidence that supported oxygen as a causative factor. Ashton8 verified these clinical findings by producing RLF changes in kittens exposed to high oxygen concentrations. In the mid-1950s, controlled clinical trials showed a significant decrease in the incidence of RLF by limiting the amount of inspired oxygen. Patz and colleagues,9,10 Lanman,11 and a national multicenter clinical trial in the United States coordinated by Kinsey12 concluded that limiting oxygen was essential.
Over the next several years, oxygen use was curtailed, and the incidence of RLF dropped dramatically. However, brain damage and death among premature infants rose. Cross13 estimated that, in the United States, for every case of possible blindness from RLF that was prevented, 16 infants died. As a more rational approach to the use of oxygen in premature infants was adopted in the mid-1960s, RLF reappeared.14 This, however, coincided with dramatic advances in technology that allowed smaller and smaller babies to be saved. During the 1970s and 1980s, an increasing incidence of RLF occurred despite increasingly sophisticated techniques of monitoring blood oxygen levels. Phelps15 suggests that both a relative and absolute increase in the incidence of ROP has occurred. It was in the 1980s that ROP became accepted as the name for RLF, a term that has now been discarded.
EPIDEMIOLOGY AND DEMOGRAPHICS
From 1943 to 1951, an estimated 7000 infants in the United States were blinded by ROP. Phelps15 estimated that approximately 546 babies were blinded by ROP in 1979. In 1950, the survival rate of infants with a birth weight of less than 1000 g was 8%, but Phelps16 reported that the survival rate rose to approximately 35% in 1980. Currently, a fetus at or beyond 25 weeks of gestation or with a weight of 700 g or more has a better than 50% chance of survival.17 These small infants are most susceptible to ROP. Campbell and colleagues18 found that the incidence of acute ROP among surviving premature babies who weighed less than 1000 g at birth was three times that of survivors with birth weights between 1001 and 1500 g.
Despite meticulous monitoring of oxygen therapy with current sophisticated techniques, ROP still occurs.19 No safe means to prevent ROP has been found.20 In a prospective, randomized, double-masked trial comparing vitamin E (tocopherol) to placebo, no difference was found in the incidence of ROP between the treated and the placebo group.21 Light exposure has been offered as a factor in causing ROP, yet a prospective, randomized, multicenter study comparing infants in typical nursery lighting to those in reduced light failed to show any difference in the incidence of ROP.22 Five hundred infants are blinded by ROP each year in the United States. Prematurity per se and its associated low birth weight is the cause of most cases of ROP in contrast to the implied overzealous use of oxygen, as had been suggested. Other factors associated with the development of ROP (but not necessarily causally related) include sepsis, hypoxia, acidosis, and intraventricular hemorrhage.
Smith has pointed out that ROP occurs in two phases.23 In the first phase, the infant experiences a relative hyperoxia in room air. Retinal vasculature stops growing, and vascular endothelial growth factor (VEGF) decreases. In the second phase, peripheral maturing retina becomes hypoxic because it is nonperfused, and VEGF increases. Neovascularization then responds to the increased VEGF. Smith has shown that in the retina of the mouse model, the VEGF usually is ahead of the neovascularization.23 Indeed, she postulates that regression of persistent fetal vasculature may be related to increased VEGF.
A growing concern is the increasing incidence of ROP in middle-income countries. Because living conditions and access to medical technology have improved in these countries, more premature infants are surviving. Hence, there is a greater incidence of ROP. In North and South America and Europe, it is becoming the major cause of infant blindness.24,25,26,27
NATURAL HISTORY
The Multicenter Trial of Cryotherapy for Retinopathy of Prematurity reported an incidence of ROP of 65.8% in the 4099 infants weighing less than 1250 g at birth who were examined within that study.28 Of infants weighing less than 1000 g at birth, the incidence of ROP was 81.6%. ROP incidence and severity were higher in lower birth weight and gestational age categories. In Tasman’s study on the natural history of ROP, all babies who became blind weighed under 1000 g.29 In the report of the Multicenter Trial of Cryotherapy for Retinopathy of Prematurity, the timing of disease development correlated more closely with postconceptional age than with postnatal age, suggesting that level of maturity is more of a determining factor than postnatal environmental influences.28 Disease level of a severity that required treatment (“threshold disease,” see later for definition) occurred in 6% of the overall group. The average postconceptional age of onset of threshold disease was 37 weeks with 95% of infants who reached threshold doing so by 42 weeks. Most infants who develop ROP undergo regression of their disease, and for those who do, ROP lasts approximately 15 weeks.30 Infants who go on to regression from mild ROP (less than stage 2, see later for classification), usually undergo complete resolution.31 There is an increased incidence of strabismus in those infants compared with those who are full term, but this may result from central nervous system effects.
The most common form of regression of ROP is continued growth of the retinal vasculature anteriorly with gradual fading of the disease at the border of posterior vascularized and anterior avascular retina. Another more dramatic sign of regression is the growth of vessels beyond the ridge (Fig. 1). The vessels penetrate into the avascular retina as an arteriole with an accompanying venule. As the vessels grow beyond the ridge, the dilation and tortuosity of vessels just posterior to the shunt and in the posterior pole diminish.
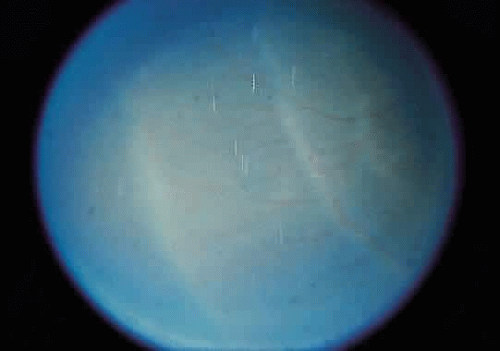 Fig. 1. Regressing retinopathy of prematurity. The vessels have crossed the ridge and are growing into the avascular zone. |
AN INTERNATIONAL CLASSIFICATION FOR RETINOPATHY OF PREMATURITY
A classification system for acute ROP, devised by 23 ophthalmologists from 11 different countries, was published and widely accepted in 1984.20 This system, the International Classification of Retinopathy of Prematurity (ICROP), easily replaced previous classifications32,33,34,35,36,37,38,39,40 because a much greater understanding of ROP had been gained since their publication. Before the 1984 classification, it was not possible to compare treatment results, since it was not clear what stage of the disease was being treated. The 1984 classification clearly defines the location of the disease in the retina as well as the extent of the developing vasculature that is involved.
To define location, the retina was divided into three zones with the optic nerve as the center, since retinal vascular growth proceeds from the disc toward the ora serrata (Fig. 2). Zone I consists of a circle, the radius of which extends from the disc to twice the distance from the disc to the center of the macula (twice the disc-fovea distance in all directions from the optic disc). Zone II extends from the edge of zone I peripherally to a point tangential to the nasal ora serrata and around to an area near the temporal anatomic equator. Zone III is the residual temporal crescent of retina anterior to zone II. This is the zone that is vascularized last in the premature eye, and it is the zone most frequently involved with ROP. The extent of disease is specified as hours of the clock (see Fig. 2). The second parameter specified in the 1984 classification is staging of the disease, that is, the degree of abnormal vascular response observed. Four stages were recognized, and staging for the eye as a whole receives the stage of the most severe manifestation of ROP present. Stage 1 (demarcation line) is defined as a thin but definite structure that separates avascular retina anteriorly from the vascularized retina posteriorly. Abnormal branching or arcading vessels are seen leading up to the line. It is flat and white and is in the plane of the retina. Stage 2 (ridge) is present when the line of stage 1 has grown, has height and width, and occupies a volume extending up out of the plane of the retina. The ridge may be pink or white, and vessels may leave the plane of the retina to enter it. Small tufts of new vessels may be seen on the surface of the retina posterior to the ridge. These vessels do not constitute fibrovascular growth, which is a necessary condition for stage 3 ROP. Stage 3 (ridge with extraretinal fibrovascular proliferation) exists when extraretinal fibrovascular proliferation is added to the ridge of stage 2 ROP (Fig. 3). Stage 3 is arbitrarily further subdivided into mild, moderate, and severe. Stage 4 (retinal detachment) is the addition of retinal detachment to stage 3 findings. Traction or exudation cause the retinal detachment.
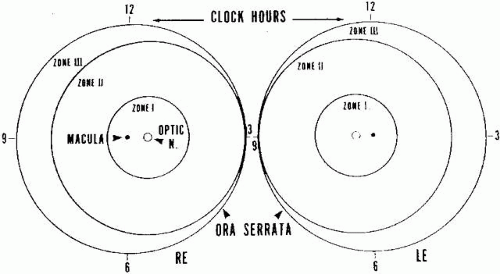 Fig. 2. Zones I, II, and III of retinopathy of prematurity. |
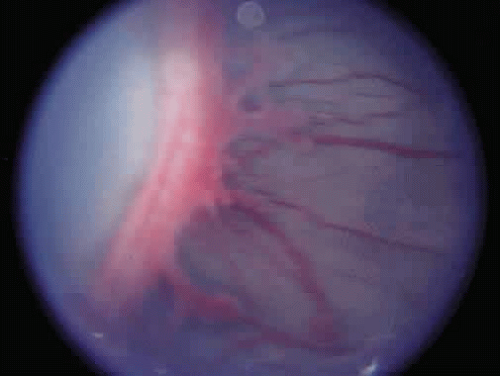 Fig. 3. Stage 3 retinopathy of prematurity. |
Progressive vascular incompetence, occurring with the changes at the edge of the abnormally developing retinal vasculature, is noted by increasing dilation and tortuosity of the peripheral retinal vessels, iris vascular engorgement, pupillary rigidity, and vitreous haze. When the vascular changes are so marked that the posterior veins are enlarged and the arterioles are tortuous, a plus sign is added to the ROP stage number (Fig. 4). Subsequent to the initial ICROP report, completion of the classification of ROP led to the publication of the classification of retinal detachment.41 Stage 4 was expanded to stage 4A and 4B. Stage 4A (Fig. 5) represents extrafoveal retinal detachment, which is a concave traction type of retinal detachment in the periphery without involvement of the macula. These detachments generally are located in anterior zone II or III. Stage 4B (Fig. 6) is a partial retinal detachment including the fovea, which usually extends in the form of a fold from the disc through zone I to involve zones II and III. Stage 5 retinal detachments are total and always funnel shaped. Stage 5 is subdivided based on the shape of the funnel. The funnel is divided into anterior and posterior parts, allowing for four subdivisions, depending on whether the funnel is open or narrow in both parts of the funnel.
 Fig. 4. Marked “plus” disease. |
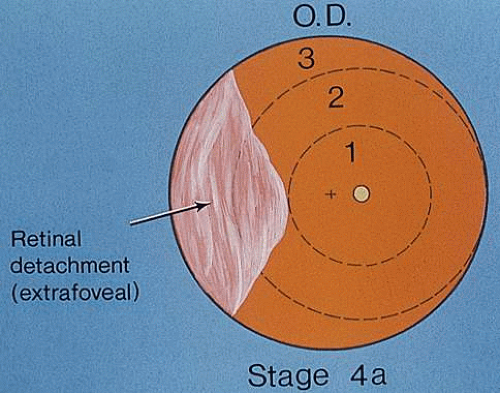 Fig. 5. Stage 4A retinopathy of prematurity. |
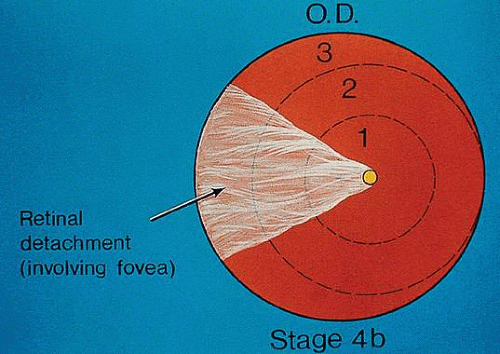 Fig. 6. Stage 4B retinopathy of prematurity. |
Although regression was not part of the classification, the committee recognizes that it is the most common outcome of ROP. The various patterns of regression were believed to be too numerous to classify; they are listed in (Table 1).
TABLE 1. Findings in Regressed Retinopathy of Prematurity | |
|---|---|
|
SCREENING FOR RETINOPATHY OF PREMATURITY
A useful screening protocol for ROP has been reported through a joint statement of the American Academy of Pediatrics, the American Association for Pediatric Ophthalmology and Strabismus, and the American Academy of Ophthalmology.42,43 These guidelines represent a work in progress, and further modifications are likely.
Infants recommended for screening are those with a birth weight of less than or equal to 1500 g or with a gestational age of 28 weeks or less. Additionally, infants weighing over 1500 g, with an unstable clinical course believed to be at high risk by the attending pediatrician or neonatologist, should have a dilated indirect ophthalmoscopic examination. Considering that the guidelines are a work in progress, Wright and colleagues44 point out that a gestational age cutoff of 28 weeks or less may be overly restrictive. In their retrospective study of 707 infants, 10 of 74 infants with stage 2 ROP, 5 of 63 with stage 3 ROP, and 1 of 4 with stage 4 ROP had a gestational age greater than 28 weeks. The British guidelines are more inclusive than the American, recommending screening for infants weighing 1500 g or less or those born at a gestational age of 31 weeks or less.45
The American guidelines further state that the examination should be done between 4 and 6 weeks of chronologic age or between 31 and 33 weeks’ postconceptional age. Follow-up examinations are determined by the findings at the first examination using the ICROP. For example, if the retinal vasculature is immature and in zone II but no disease is present, follow-up examination should be planned at approximately 2- to 4-week intervals until vascularization proceeds into zone III. Infants with ROP in zone I should be seen at least every week until involution of ROP occurs and normal vascularization proceeds to zone II. Infants with immature vessels (without ROP) detected in zone I should be seen at least every 1 to 2 weeks until normal vascularization proceeds to zone III or the risk of attaining threshold has passed.
Follow-up examinations should be performed until either complete retinal neovascularization occurs or two successive 2-week examinations show stage 2 ROP in zone III. Infants then should be followed every 4 to 6 weeks until fully vascularized. Infants who develop threshold disease (see later) should be considered for ablative therapy of at least one eye within 72 hours of diagnosis.
Examinations usually take place in the intensive care nursery (ICN). Monitoring of infants by the ICN staff is essential. Examination should take place no sooner than 1 hour after feeding to avoid the risk of vomiting and aspiration. We use homatropine hydrobromide 2% and phenylephrine hydrochloride 2.5% every 15 minutes three times 1 hour before examination. This allows for an adequate interval of dilation and frequently overcomes iris vascular engorgement in cases of severe stage 3+ ROP. Topical anesthesia with proparacaine or tetracaine is administered, and a lid speculum is inserted. Anterior segment examination followed by indirect ophthalmoscopic examination with a 20, 25, 28, or 40 diopter (D) lens then is performed.
The degree of dilation should be noted on anterior segment examination. Poor dilation may reflect iris vascular engorgement, implying active ROP. This often is mistaken for iris neovascularization. Careful record keeping, preferably on a standardized form, noting the zone, the stage of each 30-degree sector, and the presence or absence of “plus” disease, should be performed. When regression occurs, those signs also should be noted. Noting follow-up arrangements is important, preferably in the doctor’s orders, so that future examinations are not missed.
TREATMENT
Japanese investigators were the first to describe successful treatment of the active stages of acute ROP.46,47,48,49,50 Investigators in Israel51 and Canada52 later showed positive results with cryotherapy.
Initially, acceptance of this form of therapy was slow, but it later gained acceptance in the United States.32,53,54,55,56,57,58 To resolve any doubt concerning the value of cryotherapy for ROP, the National Eye Institute supported a multicenter prospective randomized clinical investigation called the Multicenter Trial of Cryotherapy for Retinopathy of Prematurity (abbreviated as CRYO-ROP Study). The preliminary results were so favorable that a special expedited publication was released in 1988.59,60
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


