Purpose
To compare retinal thickness and choroidal thickness at increasing retinal eccentricity in individuals with early age-related macular degeneration (AMD) and in healthy controls using enhanced choroidal penetration, 3-dimensional optical coherence tomography at 1060 nm.
Design
Cross-sectional study.
Methods
Individuals with early AMD (n = 16; mean age, 71.6 ± 8.5 years) and a comparison group of healthy controls (n = 16; 67.6 ± 5.4 years) were recruited. Three-dimensional (20 degrees × 20 degrees) long-wavelength optical coherence tomography (1060 nm) images (approximately 8-μm axial resolution; 47 000 A scans/second, centered on the fovea) were obtained from all participants after pupil dilation. Retinal thickness was measured between the inner limiting membrane and the retinal pigment epithelium. Choroidal thickness was measured between the retinal pigment epithelium and the choroid–scleral interface. Thickness measurements were obtained subfoveally and at 0.5-mm intervals to a maximum of 2.0 mm nasally, temporally, superiorly, and inferiorly. The main outcome measures were retinal and choroidal thickness (measured in micrometers) at different eccentricities on vertical and horizontal meridians.
Results
Mean retinal thickness was reduced significantly in the group of participants with early AMD compared with the control group at multiple locations within 2.0 mm of the fovea. This difference was most significant at the fovea, where the mean retinal thickness of the early AMD group was 179 ± 27 μm and that of the control group was 202 ± 18 μm ( P = .008). There was no significant difference in choroidal thickness between groups at any location.
Conclusions
Retinal thickness is reduced in early AMD, but choroidal thickness seems to be unaffected by the early disease process.
Age-related macular degeneration (AMD) is the leading cause of blindness in the United Kingdom, and is responsible for more people being registered as sight impaired or severely sight impaired than all other ocular conditions combined. The prevalence of AMD is expected to increase globally between 2005 and 2050 because of a predicted 3-fold increase in the number of people older than 60 years. AMD manifests either as choroidal neovascularization (wet AMD) or geographic atrophy (dry AMD), whereas early AMD, also known as age-related maculopathy, is characterized by soft drusen and focal pigmentary changes only. Currently, treatment is available only for the wet (neovascular) type of AMD, usually in the form of antiangiogenic pharmacotherapy. Although no treatment currently exists for dry AMD and early AMD, there is some evidence to suggest that nutritional supplements may slow the progression of the disease. The ability to diagnose the onset of AMD accurately and to monitor disease progression is vital in the early identification of patients suitable for therapy and in evaluating the outcomes of the treatment.
Historically, the diagnosis and grading of AMD largely has been based on visual acuity and stereoscopic fundus photographs. However in recent years, detailed analysis of retinal microstructure has become possible through optical coherence tomography (OCT), which offers an extra dimension to the evaluation of age-related macular disease. OCT is a technique that uses the optical equivalent of the echo time delay in ultrasound to construct a cross-sectional image of the retina in vivo, analogous to a histologic section.
Frequency-domain (FD) OCT traditionally has used light sources with a bandwidth based at approximately 800 nm. The limitation of this band of wavelengths is partly that ocular opacities can degrade the quality of the collected image (which is especially important in the assessment of elderly individuals), but also that the high level of scatter by retinal tissue and increased absorption by the retinal pigment epithelium (RPE) results in limited visualization of sub-RPE layers. An alternative light source, with a bandwidth based at approximately 1060 nm, has been shown to allow deeper penetration into the choroidal tissue and better signal-to-noise ratio in the presence of media opacities.
Although the longer-wavelength 1060-nm OCT is the first system that allows a reliable assessment of in vivo choroidal thickness in all patients, it has been used to date only to assess outer retinal features and choroidal structure in patients with the neovascular form of AMD, where the structural changes to the choroid–Bruch’s membrane–RPE complex already are marked. There is substantial evidence to suggest that the dynamics of the choroidal circulation are affected earlier in the disease process (see Harris and associates for a review ), and histologic studies have found evidence of a difference in choroidal structure in eyes with early and advanced AMD compared with age-matched control eyes, such as reductions in choriocapillary density and choroidal thickness. However, histologic evidence regarding choroidal thickness in AMD is mixed, with some evidence to suggest a reduction, particularly in the advanced stages of the disease, whereas another study found no significant change in choroidal thickness, even in advanced AMD.
The aim of this study was to use the 1060-nm enhanced choroidal penetration OCT to investigate retinal and choroidal thickness as a function of eccentricity in patients with early AMD (drusen or pigmentary changes only) as a means of determining the potential clinical value of the 1060-nm OCT in assessing early macular disease and of providing insight into the earliest structural changes occurring in AMD.
Methods
Participants
Control participants (n = 16) and those with early AMD (n = 16) were recruited for this study from among staff, students, and volunteers attending the eye clinic at the School of Optometry and Vision Sciences and the eye unit at the University Hospital of Wales. All participants had a corrected visual acuity (VA) of 0.3 logarithm of the minimal angle of resolution units (approximately 20/40) or better assessed using an Early Treatment Diabetic Retinopathy Study sight chart and a refractive error of less than ± 6 diopters. Participants were excluded if they had secondary retinal disease, significant cataract (Lens Opacities Classification System III grade 4 or more for any criteria ), or narrow iridocorneal angles (grade 1 or less assessed by Van Herick). Each participant was given a full explanation of the procedures involved, and their written informed consent was obtained before participation in the study.
Participants were categorized into either a control or early AMD group, depending on the assessment of 37-degree digital fundus images (CR-DGi nonmydriatic retinal camera; Canon Inc, Lake Success, New York, USA) and 20-degree 1060-nm OCT images. Images were assessed for AMD-related features located within a 6000μm diameter centered on the fovea. Definitions were based on the International and the Age-Related Eye Disease Study AMD classification systems. Control participants exhibited no features associated with AMD, with any drusen present being less than 125 μm in diameter (hard drusen). Early AMD was defined as the presence of soft drusen (> 125 μm diameter), pigment changes, or drusenoid pigment epithelial detachment in the absence of any feature of advanced AMD (wet or dry) as defined by the Age-Related Eye Disease Study grading system. Classification was carried out by on of the authors (A.W.) and was confirmed independently by 2 other authors (A.B. and T.M.). One drop of tropicamide 1.0% was instilled into both eyes of each participant, ensuring pupil dilation of at least 7 mm before obtaining fundus photographs and OCT images. Images were obtained from both eyes of all individuals to determine their AMD status. One eye was selected for analysis from each participant; this was the eye with a diagnosis of early AMD or, in the case of bilateral early AMD or controls, the eye with the better VA, with the left eye used as default.
Imaging
Three-dimensional OCT imaging at 1060 nm was performed with less than 2.5 mW at the cornea, below the maximum power limit for a 10-second exposure. OCT volumes were acquired across a 20 × 20-degree (5.76 × 5.76-mm) field consisting of 512 × 512 A-scans obtained at a rate of 47 000 A-scans/second (approximately 8-7 μm axial resolution). OCT volumes were centered on the fovea, aligned by participant fixation. Axial length (cornea to RPE) measurements were acquired using optical biometry (IOL Master; Zeiss, Jena, Germany) for each eye by averaging 5 measurements.
Image processing and analysis was undertaken using ImageJ software (ImageJ, Bethesda, Maryland, USA). Raw OCT images were enhanced digitally to improve the visibility of the retina and choroidal boundaries. Postprocessing procedures were carried out subjectively and included adjustments to brightness and contrast, B-scan registration, despeckling or noise removal, and application of Gaussian or convolving blur (ie, controlled blurring of the image between adjacent b-scans). Measurements were made using the caliper function in the axial plane of the images. The thickness represented by each pixel was calculated assuming a refractive index of 1.4.
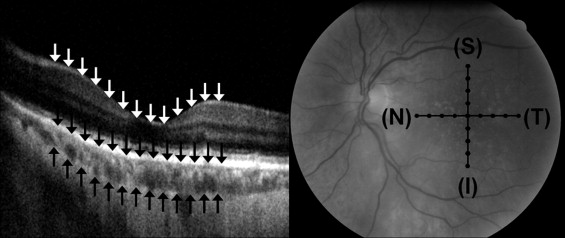
Retinal thickness was measured from the most anterior hyperreflective line, which corresponds to the inner limiting membrane, to the center of the most posterior hyperreflective line, which corresponds to the RPE. Choroidal thickness was measured from the RPE to the choroid–sclera boundary. Thickness measurements were obtained for both the retina and the choroid at the fovea and then at 0.5-mm intervals to 2 mm nasally (N), temporally (T), superiorly (S), and inferiorly (I; see Figure 1 ). This produced thickness measurements at 17 individual retinal locations for each eye. At each location, the distribution of thickness measurements was checked for normality, and an independent t test was conducted between the control and early AMD groups.
Additionally, the fundus and OCT images were assessed subjectively; specifically, the participants regarded at the highest risk of progression to advanced AMD (ie, those with drusenoid pigment epithelial detachment, confluent drusen, or a fellow eye with advanced AMD ) were compared with those at lowest risk (ie, those with normal fellow eyes and none of the high-risk features listed above).
Results
The study involved 32 participants consisting of a control group (n = 16) and an early AMD group (n = 16). The control group (n = 16) had a mean age of 67.6 ± 5.4 years and a mean axial length of 23.7 ± 0.8 mm. The early AMD group (n = 16) had a mean age of 71.6 ± 8.5 years and a mean axial length of 23.2 ± 0.7 mm. The mean age ( P = .12, independent t test) and axial length ( P = .09, independent t test) of the 2 groups were not significantly different. The clinical features of the participants with early AMD are shown in Table 1 .
| Participant | Presence of Clinical Feature | Contralateral Eye Status a | |||||
|---|---|---|---|---|---|---|---|
| No. | Age (y) | Tested Eye | Drusen Diameter > 125 μm | Drusen No. > 10 | Hyperpigmentation or Hypopigmentation | Drusenoid PED | |
| 1 | 56 | R | N | N | Y | N | Normal |
| 2 | 64 | R | Y | N | N | N | Normal |
| 3 | 80 | L | Y | N | Y | N | Normal |
| 4 | 79 | L | N | N | Y | N | Early |
| 5 | 70 | L | Y | Y | N | N | Early |
| 6 | 67 | L | Y | N | N | N | Early |
| 7 | 58 | L | Y | N | Y | N | Early |
| 8 | 87 | L | Y | N | N | N | Early |
| 9 | 73 | L | Y | Y | N | N | Early |
| 10 | 65 | L | N | N | Y | N | Wet |
| 11 | 74 | L | N | N | Y | N | Wet |
| 12 | 65 | L | Y | Y | Y | N | Wet |
| 13 | 75 | R | Y | Y | N | N | Wet |
| 14 | 78 | R | Y | Y | Y | Y | Wet |
| 15 | 79 | R | Y | N | N | Y | Wet |
| 16 | 75 | L | Y | Y | N | Y | Wet |
a Early or wet denotes the subtype of age-related macular degeneration.
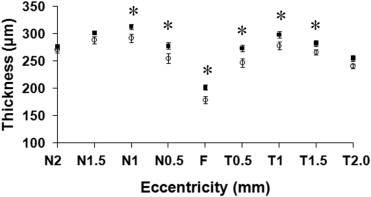
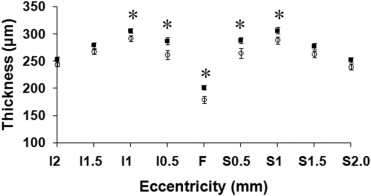
The mean retinal thickness for participants in the control and early AMD groups was plotted for each retinal location and is shown in Figure 2 for the horizontal meridian and in Figure 3 for the vertical meridian. The mean retinal thickness was found to be smallest at the fovea (F) for both groups, increasing with eccentricity in both vertical and horizontal meridians to reach a maximum at 1 mm, before declining with further increase in eccentricity. Central retinal thickness, measured at the fovea (F), was 202 ± 18 μm for the control group and 179 ± 27 μm for the early AMD group. This difference was significant ( P = .008). Table 2 shows mean retinal thickness at each retinal location and the P value for the difference between the groups. The early AMD group was found to have significantly thinner retinal thickness values at the fovea and eccentricities to 1 mm, extending to 1.5 mm temporally.
| Location a | Control Retinal Thickness (μm) | Early AMD Retinal Thickness (μm) | t Test b (* P < .05) | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| F | 202 | 18 | 179 | 27 | .008 |
| T0.5 | 274 | 24 | 247 | 31 | .011 |
| T1.0 | 299 | 23 | 278 | 27 | .030 |
| T1.5 | 282 | 22 | 267 | 20 | .038 |
| T2.0 | 255 | 22 | 241 | 18 | .055 |
| N0.5 | 278 | 24 | 255 | 35 | .040 |
| N1.0 | 313 | 19 | 292 | 30 | .028 |
| N1.5 | 302 | 15 | 289 | 27 | .092 |
| N2.0 | 276 | 20 | 271 | 22 | .480 |
| S0.5 | 288 | 22 | 265 | 37 | .039 |
| S1.0 | 306 | 23 | 288 | 25 | .045 |
| S1.5 | 277 | 23 | 263 | 24 | .090 |
| S2.0 | 252 | 19 | 239 | 21 | .083 |
| I0.5 | 287 | 24 | 261 | 33 | .018 |
| I1.0 | 306 | 15 | 292 | 22 | .036 |
| I1.5 | 279 | 21 | 267 | 19 | .104 |
| I2.0 | 253 | 23 | 244 | 15 | .205 |
a Measurement locations identified as fovea (F), nasal (N), temporal (T), superior (S), or inferior (I) with eccentricity of 0.5, 1.0, 1.5, or 2.0 mm.
b Independent t test; P values for differences between groups at each location are in boldface where a difference is significant at the P = .05 level.
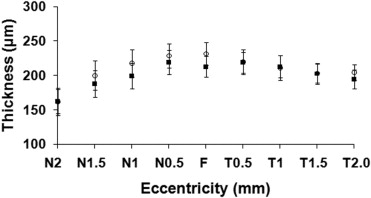
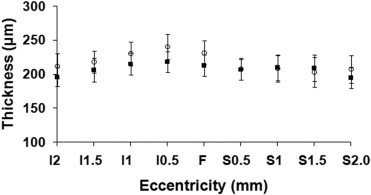
Mean choroidal thickness was plotted for each retinal location measured along horizontal and vertical meridians ( Figures 4 and 5 ). In the horizontal meridian, choroidal thickness was found to be greatest at the fovea (F), decreasing to a minimum nasally and showing a more modest reduction in thickness temporally. There was less variation in choroidal thickness in the vertical meridian. Central choroidal thickness, measured at the fovea (F), was 213 ± 63 μm for the control group and 231 ± 70 μm for the early AMD group. This difference was not significant ( P > .05, independent t test). Table 3 shows mean choroidal thickness at each retinal location and the P value for the difference between each group. The difference between groups was not significant at any location for choroidal thickness.
| Location a | Control Choroid Thickness (μm) | Early AMD Choroid Thickness (μm) | t Test ( P < .05) | ||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| F | 213 | 63 | 231 | 70 | .429 |
| T0.5 | 219 | 60 | 220 | 72 | .974 |
| T1.0 | 213 | 65 | 211 | 71 | .940 |
| T1.5 | 203 | 62 | 203 | 54 | .982 |
| T2.0 | 195 | 54 | 204 | 47 | .593 |
| N0.5 | 219 | 71 | 229 | 71 | .710 |
| N1.0 | 199 | 74 | 218 | 80 | .505 |
| N1.5 | 188 | 77 | 200 | 85 | .678 |
| N2.0 | 162 | 70 | 162 | 80 | 1.000 |
| S0.5 | 207 | 62 | 207 | 65 | .973 |
| S1.0 | 210 | 75 | 208 | 79 | .952 |
| S1.5 | 209 | 76 | 203 | 86 | .830 |
| S2.0 | 195 | 63 | 207 | 83 | .640 |
| I0.5 | 218 | 62 | 240 | 74 | .360 |
| I1.0 | 215 | 64 | 230 | 69 | .529 |
| I1.5 | 206 | 72 | 218 | 65 | .624 |
| I2.0 | 196 | 54 | 212 | 73 | .487 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


